Article Text

Abstract
Objectives Sedentary behaviour among office workers and the risk of adverse health outcomes are public health problems. However, risk indicators for these outcomes require invasive biochemical examination. A proactive screening tool using a non-invasive, easy-to-use method is required to assess the risk focused on musculoskeletal health for primary prevention. However, middle-aged adults have insufficient awareness of musculoskeletal disorders. This study examined to determine whether the 30-s chair-stand test (CS-30) can be used as a proactive screening index for musculoskeletal disorder risk of sedentary behaviour in office workers.
Design Cross-sectional study using self-administered questionnaires and physical measurements.
Setting Four workplaces located in a metropolitan area of Japan.
Participants 431 Japanese office workers aged 20–64 years. 406 valid sets of results remained (valid response rate: 94.2%).
Primary and secondary outcome measures Musculoskeletal function was measured using the CS-30, quadriceps muscle strength. Receiver operating characteristic curve analysis was used to determine the sensitivity, specificity and optimal cut-off value for the CS-30. The risk of future incidence of musculoskeletal disorders was calculated using current quadriceps muscle strength.
Results In total participants, 47.0% were male and the mean sitting time in work duration was 455.6 min/day (SD=111.2 min). The mean lower limb quadriceps muscle strength was 444.8 N (SD=131.3 N). For the optimum cut-off value of 23 on the CS-30 for all participants, sensitivity was 0.809 and specificity was 0.231. For men, the optimum cut-off was 25, with a sensitivity of 0.855 and a specificity 0.172. For women, the optimum cut-off was 21, with a sensitivity of 0.854 and a specificity 0.275.
Conclusions Sensitivity was high, but specificity was insufficient. The CS-30 may be a potential proactive screening index for musculoskeletal disorder risk of sedentary behaviour, in combination with other indicators.
- musculo-skeletal health
- physical performance
Data availability statement
Data may be obtained from a third party and are not publicly available. Requests for access to data should be addressed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
This empirical study examined the 30-s chair-stand test is a potential proactive screening index for musculoskeletal disorder risk, in combination with the assessment of other adverse health outcome indicators of sedentary behaviour.
This study used objectively assessed musculoskeletal function using physical function test and the device.
This study used a cross-sectional design, and could not clarify the relationship between quadriceps muscle strength change and the onset of lower limb musculoskeletal disorders.
Background
Sedentary behaviour and a physical inactivity are major problems that need to be addressed, especially among adult office workers.1–4 Previous studies have reported that sedentary behaviour is related to negative health outcomes such as cardiovascular disease,5–8 diabetes,5 6 8 metabolic syndrome9 and musculoskeletal disorders.10 Musculoskeletal health is the foundation of a disability-free life. However, middle-aged adults have insufficient awareness of musculoskeletal disorders11 and sedentary behaviour.
Sedentary behaviour is defined as any waking behaviour characterised by an energy expenditure of ≤1.5 metabolic equivalents while in a sitting or reclining posture.12 Previous studies reported the sitting time of Japanese adults to be about 8 hours/day7 13—the longest among 20 examined countries.13 Thus, middle-aged workers are a crucial population for assessing musculoskeletal function index as an indicator of sedentary behaviour.
Limited studies have identified the relationships between lower limb musculoskeletal disorders and sedentary behaviours among office workers.14–17 Previous studies which were conducted in Japan revealed that 22%–40% of residents in their 40s and 25%–49% of those in their 50s had lower limb musculoskeletal disorders.18 19 These findings have highlighted that early detection and intervention for lower limb musculoskeletal disorders is required to sustain musculoskeletal function.
Musculoskeletal functions related to the lower limb musculoskeletal disorders18 are muscle strength14 and speed of motion.20 These lower limb musculoskeletal functions among office workers have been assessed by using surface electromyography,16 21 muscle strength measurement using an optical measurement system17 and with the questionnaire, which includes subjective questions about pain, walking, lifestyle, personal care actions and social activities.11
However, devices such as electromyography and optical measurement systems can produce objective assessments in experimental, non-daily situations but require a great deal of time. A questionnaire can be administered with little time and is easy to use; however, this assessment approach is subjective. An inexpensive and easy-to-use screening index is therefore needed to identify those who could benefit from primary prevention of musculoskeletal function decline among sedentary adult workers.
The 30-s chair-stand test (CS-30) has high test–retest reliability and high criterion-related validity with leg extension muscle strength.22 23 CS-30 was demonstrated by the test’s ability to detect differences between various age and physical activity (PA)-level groups and CS-30 performance was significantly lower for low-active participants than for high-active participants.22 The CS-30 may therefore be usable as a new proactive screening index for musculoskeletal function decline as a measure of sedentary behaviour and may contribute to primary prevention in middle-aged individuals.
The objective of this study was to establish whether the CS-30 is a suitable proactive screening index for evaluating musculoskeletal disorder risk of sedentary behaviour in adult office workers.
Methods
Study design and participants
The study used a cross-sectional design with anonymous, self-report questionnaires and physical measurements. The setting was two local government offices and two companies in a metropolitan area in Japan. The inclusion criteria for the participants were adult office workers aged 20–64 years who answered the questionnaires and provided physical measurements. Study participants were openly recruited via a flyer and poster at each worksite. Researchers and trained research public health nurses visited each worksite, administered a survey and physical measurements from September to November 2018.
Measurements
Questionnaires
Demographic characteristics
Demographic characteristics included age, gender, household composition, educational background and employment status.
Physical and mental characteristics
Participants responded ‘yes’ or ‘no’ to indicate whether they were currently being treated for each listed disease including musculoskeletal disorders. Participants with musculoskeletal disorders were excluded. Mental characteristics were measured using the Japanese version of the Kessler 6 (K6),24 which consists of six items. Each item is scored on a 5-point Likert scale ranging from 0 to 4. The total possible score ranges from 0 to 24, with higher scores indicating higher depression and a K6 score above 5 identifies people at risk of depression.24 Cronbach’s alpha was 0.881 in this study.
Lifestyle characteristics
PA was measured using the Japanese version of the International Physical Activity Questionnaire-Short Form (IPAQ-SF),25 a 7-day self-administered questionnaire.26 The IPAQ-SF asks about three types of PAs: walking, moderate PA and vigorous PA. Computation of the total score requires the summation of the products of the duration (in minutes) and the frequency (in days) of walking, moderate PA and vigorous PA.27 The IPAQ-SF is considered reliable and valid in 12 countries including Japan.26
Commuting and employment situation characteristics that indicate a sitting time were measured using the Worker’s Living Activity-time Questionnaire (WLAQ),4 28 which was designed by the National Institute of Occupational Safety and Health Japan (JNIOSH). The JNIOSH-WLAQ asked the participants about time spent sitting, standing and walking during their working and commuting time, typical domains of workers’ lives.
Physical measurements
Body mass index
Body mass index (BMI) was calculated using height and body weight measurements. Height was measured with a stadiometer (seca 213; seca, Chiba, Japan) and body weight was measured with a digital weight scale (UC-322; A&D, Tokyo, Japan). Overweight was defined as BMI≥25, standard weight was defined as 18.5≤BMI<25 and low weight was defined as BMI<18.5, based on the criteria.29
Musculoskeletal function
The CS-30 involves repeatedly standing up from a seated position in a chair over a period of 30 s, as fast as possible.22 23 This test was developed by Jones et al 22 to evaluate lower limb muscle strength. The test has high reliability using the test–retest method (r=0.92), as well as a strong correlation with leg extension strength (leg press; r=0.71).22 23 Nakatani et al modified the CS-30 and showed that this modified CS-30 can evaluate muscle strength for use in Japanese populations of all ages.23 30 31 The participants were instructed to place one foot slightly in front of the other to help maintain balance when standing and to cross their arms at the wrists and hold them against the chest. The score was the total number of stands executed correctly within 30 s. Incorrectly executed stands were not counted.22
Quadriceps muscle strength (QMS) was measured using the Locomo Scan (ALCARE, Tokyo, Japan). This device was developed based on the method for quadriceps setting training in a knee extension position.32 The Locomo Scan allows chronological measurement of knee extension muscle strength using strain gauge measurement. The smallest measurement unit was 1 N, and the maximum measured value was 1500 N.32 Omori et al 33 have previously reported that the maximum measured values using a prototype of Locomo Scan correlated significantly with the maximum measured values taken using an isokinetic machine (Biodex System 3; Biodex Medical System, Shirley, New York, USA).34 35 We calculated the weight bearing index (WBI) as QMS (in kilogram-force) divided by body weight (in kilograms).
Data analysis
IBM SPSS Statistics V.22.0 was used for the analysis. A critical endpoint calculated by the rates of change in QMS values affected the onset of lower limb musculoskeletal disorders.36 Based on the reference QMS standardised values for adults,32 the rate of change in QMS between each 10-year age group from participants in their 20s to those in their 60s and reference values in older ages showing the onset of lower limb musculoskeletal disorders were calculated separately for men and women. The average QMS value in those showing musculoskeletal disorder onset was clarified by Takagi et al 36 and was used in this study as the QMS value related to the onset of musculoskeletal disorders as the critical endpoint. Those with QMS values below the values recommended for adults to avoid musculoskeletal disorders were categorised as showing musculoskeletal function decline indicating the adverse health outcome of sedentary behaviour (the risk group), and other participants were defined as the non-risk group. Among men, a score of 433 N or below in their 20s, a score of 430 N or below in their 30s, a score of 440 N or below in their 40s, a score of 359 N or below in their 50s and a score of 333 N or below in their ages 60–64 were classified as the risk group. Among women, a score of 419 N or below in their 20s, a score of 368 N or below in their 30s, a score of 334 N or below in their 40s, a score of 293 N or below in their 50s and a score of 242 N or below in their ages 60–64 were classified as the risk group. Receiver operating characteristic (ROC) curve analysis was used to compare the risk and CS-30 score to determine the sensitivity, specificity and validity of the optimal CS-30 cut-off value as a sedentary behaviour index for all participants, and for men and women separately, with cut-off values with 80% sensitivity based on Youden’s Index.37 Two-sided statistical tests were considered significant with an alpha level of 0.05.
Patient and public involvement
Patients or the public were not involved in the design or planning of the study.
Results
A total of 431 people in the four workplaces agreed to participate. After the exclusion of 25 participants (19 participants because of incomplete information and 6 participants because of musculoskeletal disorders), 406 valid sets of results remained (valid response rate: 94.2%). The demographic characteristics of the participants are shown in table 1. Their average age was 44.1 years (SD=10.2 years), 47.0% were male and 72.4% were full-time workers.
Participants’ demographic characteristics
The mental and lifestyle characteristics of the participants are shown in table 2.
Participants’ mental and lifestyle characteristics
In total, 68.5% had a low level of PA according to the IPAQ-SF. The mean one-way commute duration was 55.2 min (SD=26.6 min), and the mean work duration was 577.0 min/day (SD=83.6 min) according to the JNIOSH-WLAQ.
The mean sitting time in one-way commute duration was 20.1 min (SD=21.5 min), and the mean sitting time in work duration was 455.6 min/day (SD=111.2 min).
The participants’ physical measurements are shown by sex in table 3. The mean CS-30 score was 20.1 (SD=4.5), the mean lower limb QMS (either right or left) was 444.8 N (SD=131.3 N), the mean lower limb WBI (either right or left) was 0.74 (SD=0.22). The CS-30 was significantly weakly or moderately correlated with lower limb QMS (r=0.293 in total, 0.186 in men and 0.361 in women, p<0.001) and lower limb WBI (r=0.305 in total, 0.219 in men and 0.487 in women, p<0.001).
Participants’ physical measurement results
In total, 63 men (33.0%) were identified as having a high risk of declining musculoskeletal function. Of these, five participants in their 20s (21.7%) had a low QMS score of 433 N or below, 16 in their 30s (34.0%) had a QMS score of 430 N or below, 27 in their 40s (47.4%) had a QMS score of 440 N or below, 12 in their 50s (24.0%) had a QMS score of 359 N or below and 3 aged 60–64 years (21.4%) had a QMS score of 333 N or below. A total of 48 women (22.6%) had a high risk of declining musculoskeletal function. Of these, 7 in their 20s (33.3%) had a low QMS score of 419 N or below, 16 in their 30s (43.2%) had a QMS score of 368 N or below, 16 in their 40s (16.8%) had a QMS score of 334 N or below, 8 in their 50s (14.5%) had a QMS score of 293 N or below and 1 aged 60–64 years (14.2%) had a QMS score of 242 N or below. The ROC curves for the ability of the CS-30 to assess risk of declining musculoskeletal function as an indicator of sedentary behaviour are shown in figures 1–3.
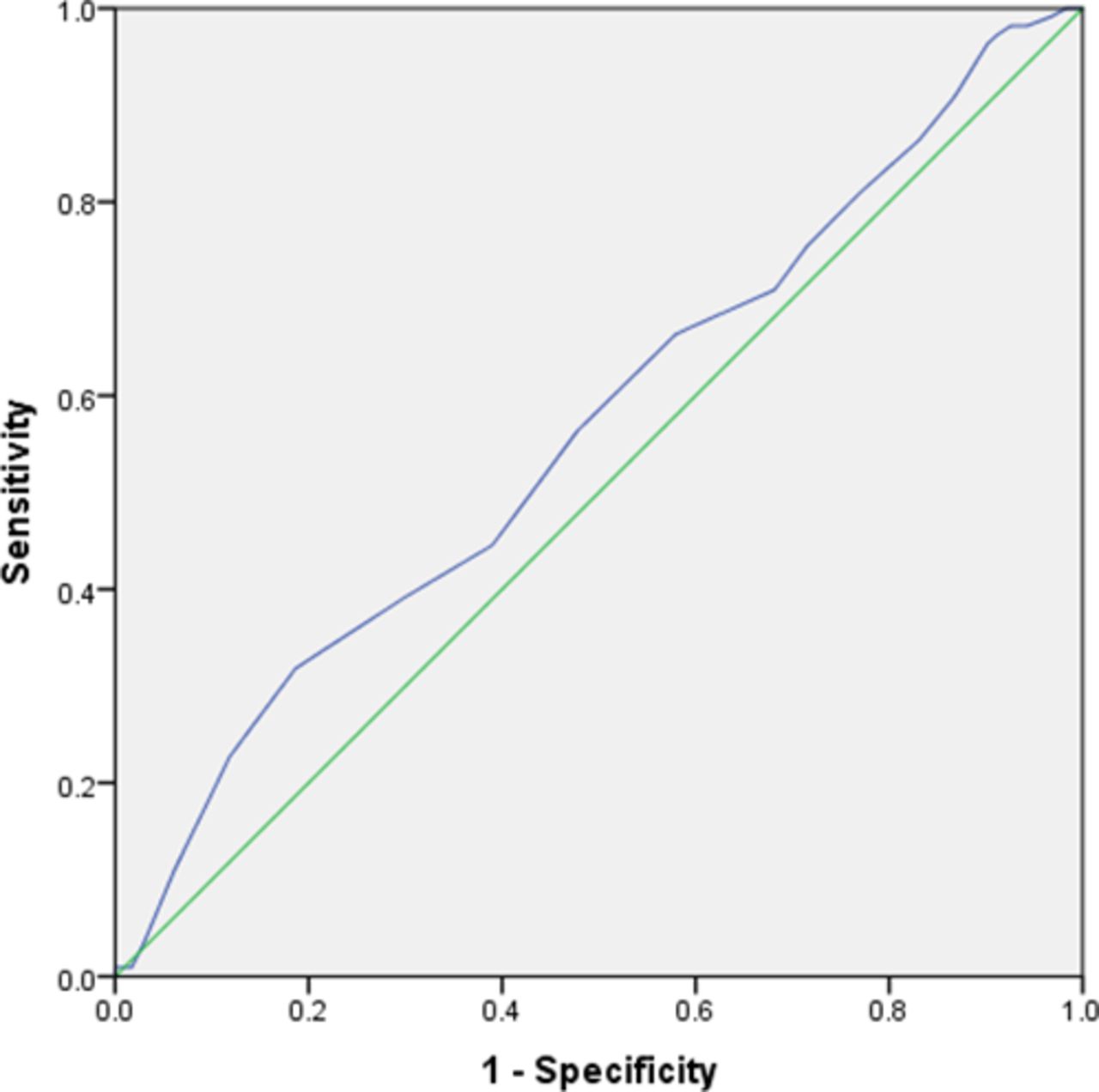
Receiver operating characteristic curves of 30-s chair-stand test (CS-30) as an indicator of sedentary lifestyle in all participants. CS-30 optimal cut-off: ≤23. Sensitivity: 0.809. Specificity: 0.231. Area under the curve: 0.565.
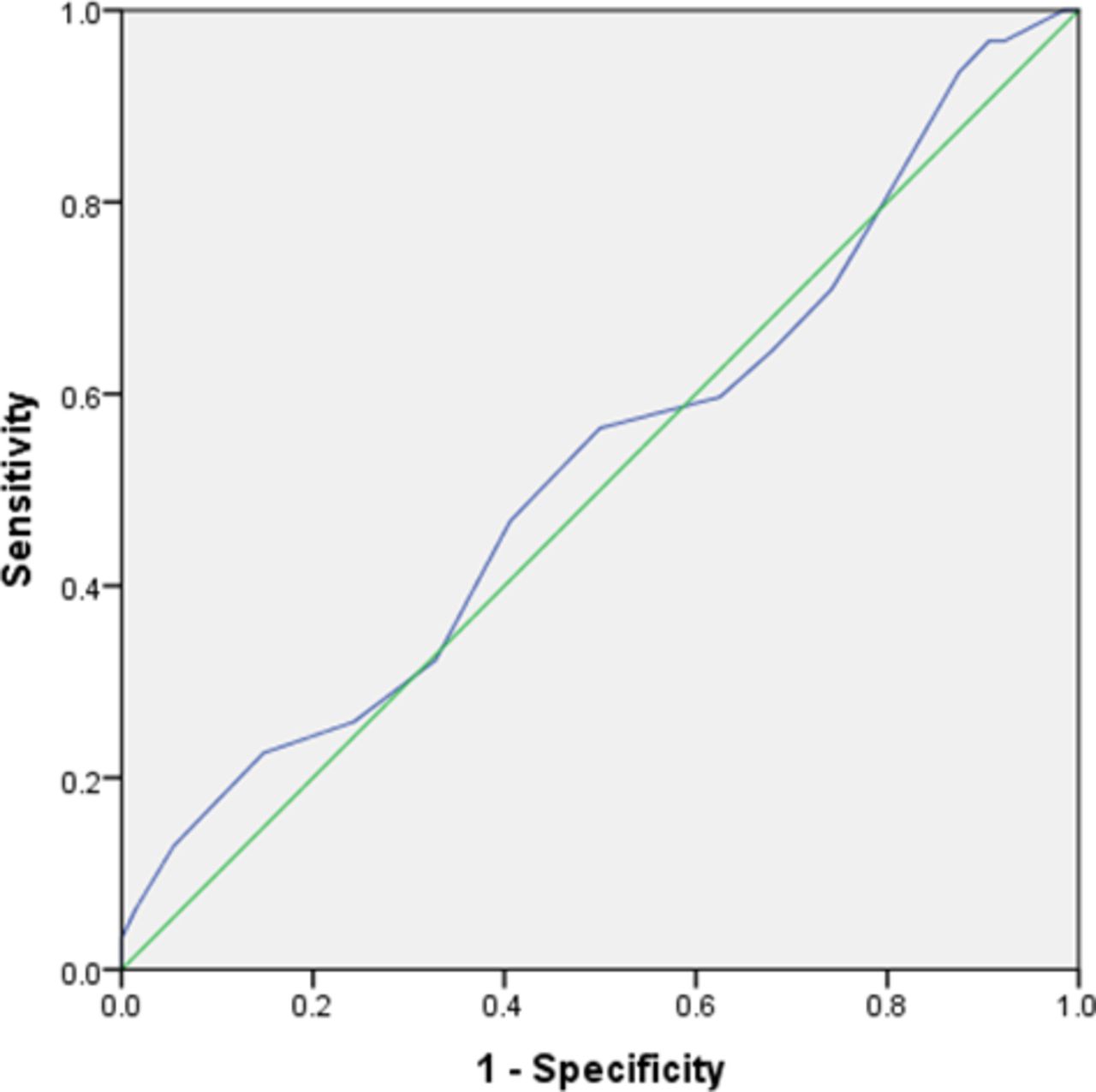
Receiver operating characteristic curves of 30-s chair-stand test (CS-30) as an indicator of sedentary lifestyle in men. CS-30 optimal cut-off: ≤25. Sensitivity: 0.855. Specificity: 0.172. Area under the curve: 0.528.
{kind=link}
{kind=link}
{kind=link}
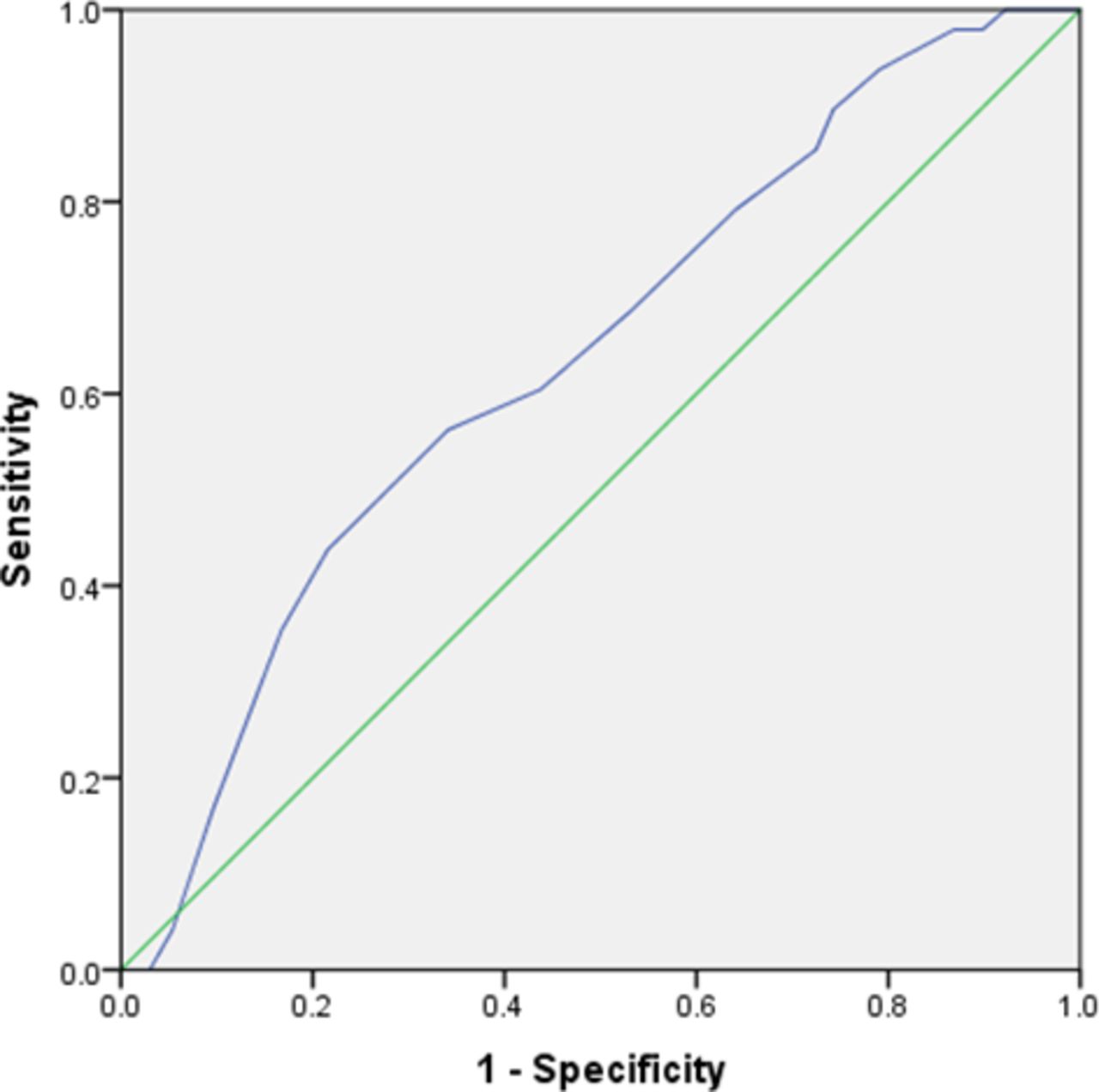
Receiver operating characteristic curves of 30-s chair-stand test (CS-30) as an indicator of sedentary lifestyle in women. CS-30 optimal cut-off: ≤21. Sensitivity: 0.854. Specificity: 0.275. Area under the curve: 0.637.
We determined the sensitivity, specificity and validity of the optimal CS-30 cut-off value for all participants, and for men and women separately, with cut-off values with 80% sensitivity based on Youden’s Index.37 Three cut-off values are shown for the ROC curve for each gender in addition to all participants because both the reference QMS standardised values for adults32 and the average QMS values in those showing musculoskeletal disorder onset clarified by Takagi et al 36 differed by gender. For all participants, the optimum CS-30 cut-off was standing up 23 times, which had a sensitivity of 0.809 and a specificity of 0.231 with an area under the curve (AUC) of 0.565. For men, the optimum cut-off was standing up 25 times, with a sensitivity of 0.855 and a specificity of 0.172 with an AUC of 0.528. For women, the optimum cut-off was standing up 21 times, with a sensitivity of 0.854 and a specificity of 0.275 with an AUC of 0.637.
Discussion
The physical measurement results for the lower limb revealed a mean QMS score of 444.8 N and a mean WBI score of 0.74. One previous study using the same device showed that the mean QMS for participants aged from their 20s to their 60s was 485.7 N.32 Another study reported that a WBI score ranging from 0.6 to 0.8 in the general population indicates no hindrance in daily performance.33 The present study’s total sitting time per day is similar to a previous report of sedentary time among Japanese adult workers (mean: 8.4±3.4 hours/day)7 and longer than a previous study results for sitting time among Japanese adults (median: 420 min).38 Therefore, participants in the present study may be similar to middle-aged workers in the general population in Japan. In both of the previous studies32 33 used to calculate the cut-off value, the middle-aged and older age groups included working people and non-working people. In a previous study19 that included community residents who were not working, 49% of participants in their 50s had lower limb musculoskeletal disorders. It has been shown that middle-aged and older workers have higher levels of health than non-workers. This suggests that workers above 50 years of age in the present study had better QMS values than the reference values.
A physical function index as an indicator of sedentary behaviour risk was estimated from the risk of future incidence of musculoskeletal disorders and optimum CS-30 cut-off values with a sensitivity of over 0.80 were identified as 23 for all participants, 25 for men and 21 for women. These results suggest that there is a low probability of a false negative (determining no musculoskeletal disorder risk when the risk is actually high). The CS-30 could therefore be useful as a proactive screening test for identifying and targeting primary prevention programmes in the large population of healthy individuals with low levels of risk, as an effective public health strategy.39 The specificity of these cut-off points was low, at about 0.20, which is similar to the findings of a previous study that reported a sensitivity of 1.000 when the specificity was 0.196 for using the seated toe-touch test to identify musculoskeletal disorders.34 A performance test to be used before is more expensive and precise diagnostic test, the cut-off value had high sensitivity (0.900), whereas specificity was 0.260.40 These findings suggest that the method of setting cut-off points with high sensitivity is valid. However, the specificity could have been low because we used a hard endpoint that only assessed risk of declining musculoskeletal function as an indicator of sedentary behaviour based on the risk of onset of lower limb musculoskeletal disorders and the QMS score.
The CS-30 only involves counting the number of times the person stands up in 30 s and no complicated calculations are necessary. This measurement is therefore easy to conduct and provides a realistic assessment of an individual’s performance. This study used an examiner to ensure accuracy. However, in practice, self-checks using the second hand on a watch or a timer are also possible. The explanation and practice before the measurement are not time consuming because standing up is a normal part of everyday behaviour. The CS-30 is also very safe and has been used successfully with frail older adults.22 23 The CS-30 is therefore a performance test that can be used to evaluate musculoskeletal function, as an indicator of sedentary behaviour. This method is simple and non-invasive. Even if an individual is judged to be at high risk of declining musculoskeletal function, any physical, mental or economic burden will be caused by the examination, diagnosis or treatment.
The present study had several limitations. First, this study focused on lower limb musculoskeletal disorder onset as an indicator of musculoskeletal function deterioration among the various negative outcomes caused by sedentary behaviour. Other indexes focusing on the additional outcomes of musculoskeletal functional decline can be selected as proactive screening indicators to understand the preliminary stages of musculoskeletal disease onset. Second, this study was cross-sectional in design. A longitudinal study is required to clarify the relationship between QMS change and the onset of lower limb musculoskeletal disorders, as well as to clarify the optimal predictive power of the CS-30 cut-off values identified in this study. Selection bias in this study may have occurred because the target population was limited to employees who worked for four Japanese companies and voluntarily responded to the open recruitment. For example, it is possible that people with a strong interest in health were more likely to cooperate, whereas those with lower limb muscle strength issues may have been less likely to take part. Future studies should be conducted in a wider range of countries, regions and occupations, and with a larger number of subjects. For the CS-30, we considered that the possibility of interviewer bias is relatively low due to training and unified procedures. Future studies will be needed to verify the inter-rater reliability of this method.
Conclusion
This study aimed to establish whether the CS-30 is a suitable proactive screening index for evaluating musculoskeletal disorder risk of sedentary behaviour in adult office workers. The results indicated that the optimal CS-30 cut-off value was 23 overall, 25 for men and 21 for women. Sensitivity was high, but specificity was insufficient. The CS-30 may be a potential proactive screening index for musculoskeletal disorder risk of sedentary behaviour, in combination with other indicators of other adverse health outcomes of sedentary behaviour to facilitate early primary prevention of adverse musculoskeletal health outcomes.
Data availability statement
Data may be obtained from a third party and are not publicly available. Requests for access to data should be addressed to the corresponding author.
Ethics statements
Ethics approval
The Human Genome/Genetic Research Ethics Committee of the Medical Department of Yokohama City University, Japan (A180700001). The questionnaire in this study was unsigned to maintain the anonymity of all participant information. The researchers explained the contents of the survey to the participants, and consent was considered as consent to the survey by answering and submitting a questionnaire.
Acknowledgments
The authors thank all the participants in this study. The authors also thank Assistant Professor K Shiratani, E Ito and all members of the Department of Community Health Nursing, Graduate School of Medicine, Yokohama City University. The authors thank Edanz Group (https://en-author-services.edanz.com/ac) for editing a draft of this manuscript.
References
Footnotes
Contributors AA, SI and ET developed the concept and design of this study. SI and ET were responsible for funding. AA and SI were responsible for the data collection, analysis, drafting and revising the manuscript. ET was responsible for obtaining institutional review board approval, the supervision and for the reporting of study results. All authors read and approved the final manuscript.
Funding This work was supported by research grants from the Health Science Centre Foundation, Japan (Principal Investigator: SI).
Competing interests None declared.
Patient and public involvement statement Patients or public were not involved in the design or planning of the study.
Provenance and peer review Not commissioned; externally peer reviewed by Dr Emmanuel Baah, University of North Carolina System.