Article Text

Abstract
Background Iodine deficiency can have adverse health effects in all age groups affecting growth, development and cognitive functions as well as the incidence of goitre. Worldwide, the most important dietary source of iodine is iodised salt. In Tanzania, iodine intake has varied due to multiple salt suppliers producing iodised salt with varying quality. Zanzibar has faced challenges with the packing, storing and monitoring of salt iodisation, and universal salt iodisation has not been achieved. Furthermore, the number of available studies on the iodine status in Zanzibar are sparse.
Objective The main objective of this study is to describe the iodine status of euthyroid female adult patients with and without goitre in Zanzibar.
Design and methods A single-centre matched case-control study was conducted among 48 female patients at the ear, nose and throat clinic of Mnazi Mmoja Hospital, Zanzibar. Blood samples were drawn for serum-analysis of the thyroid hormone profile to confirm that all patients were euthyroid prior to inclusion. Urinary iodine concentrations and the iodine concentration in household salt samples were analysed. A semiquantitative food frequency questionnaire (FFQ) was used to describe trends in the dietary intake of iodine-rich and goitrogenic foods. Clinical examinations were conducted, and the patients were categorised into goitre (cases) and non-goitre (controls) groups.
Results A moderate iodine deficiency (median urinary iodine concentration between 20 and 49 µg/L) was found in patients both with and without goitre. In total, only 35 % of the salt samples were adequately iodised. The salt samples from the cases had a lower average concentration of iodine compared with the controls. The FFQ revealed that the daily consumption of marine fish and the weekly consumption of raw cassava were more frequent in the cases than the controls.
Conclusion These findings suggest that iodine deficiency may be a problem in both patients with and without goitre in Zanzibar. The salt iodisation programme may require monitoring and implementation of satisfactory quality control practices as universal salt iodisation is yet to be achieved in Zanzibar.
- nutrient deficiencies
- nutrition assessment
- dietary patterns
- malnutrition
- nutritional treatment
Data availability statement
Deidentified participant data are available from Hanne Rosendahl-Riise (Hanne.rosendahl-riise@uib.no/ORCID 0000-0002-1497-416X) on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
Suboptimal iodine nutrition among females in Zanzibar.
Unsatisfactory salt iodisation programme emphasising the need for quality control.
Introduction
Iodine is an essential micronutrient with a central role in thyroid hormone production and regulation. It is introduced into the food chain via seawater, soil and drinking water. Worldwide, the most important dietary source is iodised salt.1 Adequate iodisation of salt is essential in countries where the iodine content in soil and drinking water is insufficient and access to marine foods is limited. Iodine deficiency disorders remain an important health problem in some areas.1–3 The most characteristic physical symptom is an enlargement of the thyroid gland called goitre.4 5 In women of reproductive age (WRA), iodine deficiency during pregnancy can result in abortion, stillbirth or congenital abnormalities in the fetus.1 5 The consequences in children and adolescents include growth, developmental and cognitive impairments, and decreased educability and reduced work capacity in adults.1 4 6
In 2016, Tanzania had an optimal iodine intake at the national level.3 7 In WRA, the household coverage of iodised salt was reported by 80% of the participants, yet adequate iodisation was found in only 61% of the analysed salt samples.7 Nationally, iodine intake has varied due to hundreds of suppliers producing iodised salt of varying quality.3 Zanzibar was formerly not included in Tanzanian surveys partly due to the assumption that islands surrounded by the ocean have adequate iodine intake from marine foods.8 However, significant iodine deficiencies have been documented in coastal areas.1 In 2011, the Food Security and Nutrition Act promoted the use of iodised salt in Zanzibar.9 Despite this, Zanzibar still faces challenges as the packing and storage of iodised salt is not controlled.9
There are uncertainties regarding the iodine status in general in Zanzibar and its importance regarding goitre in women. Thus, the present study investigated the iodine status of female patients with and without goitre attending Zanzibar’s largest hospital to address the need for larger preventive and clinical studies.
Material and methods
Study design, recruitment and study population
The present study was a single-centre, matched case-control study conducted at Mnazi Mmoja Hospital (MMH) in Stone Town, Unguja Island, Zanzibar. The study size was based on the number of eligible female patients attending the ear, nose and throat (ENT) clinic of MMH between 8 November and 5 December 2019. All patients were screened according to the inclusion and exclusion criteria presented in box 1. The patients were informed that participation was voluntary, and the subjects were asked to meet at the outpatient clinic once for clinical and biomedical assessments. No further follow-up assessments were planned. Two local health workers at the ENT clinic assisted in patient screening, recruitment and data collection. The cases were patients with a goitre diagnosis, and their thyroid glands were palpated to classify the degree of goitre according to the WHO’s classification system.1 10 The controls were patients without goitre attending the ENT clinic for other reasons such as tonsillitis, throat soreness, ear pain, wax impactions, the common influenza or a combination of these symptoms. Following recruitment of the cases, the controls were enrolled through a selective process which entailed matching 1:1 (patient with goitre and without goitre) by age (±5 years).
Study inclusion and exclusion criteria.
Inclusion criteria
Patient at the ENT clinic of MMH.
≥18 years of age.
Female.
Ability to provide informed consent.
Exclusion criteria
Use of medication interfering with thyroid hormone production.
Hypothyroidism or hyperthyroidism.
Previously operated for goitre.
Pregnant or breastfeeding.
ENT, ear, nose and throat; MMH, Mnazi Mmoja Hospital.
Questionnaire
The patient interview included questions regarding general health, knowledge on goitre and socioeconomic background variables (education level, employment situation, marital status, number of children, area of residence and food preparation practices). Furthermore, the questionnaire included iodine-related information such as source of drinking water, family members that fish or produce salt, type of salt consumed and salt storage practices in the household. The questionnaires and interview instructions were independently translated and back-translated from English to Kiswahili.
Anthropometric measurements
The patients were weighed to the nearest 0.1 kg using a medical scale for mobile use (SECA 877, Hamburg, Germany), and height was measured to the nearest 0.1 cm using a stadiometer (FAZZINI S7200HR, Italy). Body mass index (BMI) (kg/m2) was calculated using the measured weight in kilograms (minus 1 kg for clothing) and height in metres and classified according to WHO’s categories for underweight, normal weight, overweight and obesity.11
Blood sampling
Blood was drawn for an analysis of thyroid hormone profile to determine whether the patients were euthyroid. Patients with results revealing hypothyroidism or hyperthyroidism were excluded from the study and followed-up by health workers at MMH. The laboratory at Tasakthaa Global Hospital used the ichroma fluorescence immunoassay method for the quantitative determination of thyroid stimulating hormone (TSH), thyroxine (T4) and triiodothyronine (T3) in serum according to Boditech Med Incorporated’s protocols.12–14
Urine sampling
Spot urine samples were collected from the study participants in universal urine sampling containers and stored frozen at −250 C at the MMH laboratory before being transported to Dar es Salaam Institute of Technology. Urinary iodine concentration (UIC) was determined using the Sandell-Kolthoff reaction.15 Furthermore, the individual UIC results were aggregated to find the median UIC (MUIC) of the study population and assess iodine status according to WHO’s epidemiological criteria.1
Assessment of dietary iodine intake
All patients answered a semiquantitative food frequency questionnaire (FFQ) designed for the present study that specifically assessed potential iodine-containing and goitrogenic food items that could be of importance for the development of goitre and iodine deficiency. The FFQ assessed dietary intake from the preceding 1 month and included questions on self-reported intake of salt (both iodised table salt and non-iodised rock salt). Household utensils locally purchased in Zanzibar were used to assist participants in estimating portion sizes. Due to the lack of food tables and data on the iodine and goitrogen content of foods in Zanzibar, the FFQ was used to describe trends in the dietary intake of iodine-rich and goitrogenic foods.
Salt analysis
To determine the percentage of participants consuming adequately iodised salt, they were given a zip-lock plastic bag to be filled with approximately 1 tablespoon (10 g) of salt from their household. The salt samples were analysed for iodine content by the Norwegian Institute of Marine Research using inductively coupled plasma mass spectrometry (ICP-MS) with tetramethylammonium hydroxide. Thereafter, the iodine concentration was determined using a standard addition curve. Field trips to local markets and shops and conversations with sellers were used to identify the brands and amount of iodine in rock and table salt that were sold in Zanzibar.
Data analysis
Descriptive statistics included mean values with SD, 95% CI and median with IQR and ranges (minimum and maximum) for continuous variables, and frequencies and percentages for categorical variables. ORs were calculated for bivariable associations using the Mantel-Haenszel OR estimate and mean differences were presented with 95 % CI using t-tests. Data analysis and statistics were performed using Microsoft Excel 2017 for Mac (Microsoft, Redmond, Washington, USA) and IBM SPSS Statistics for Windows V.25 (IBM, Armonk, New York, USA).
Ethical approval and informed consent
The study was conducted according to the guidelines of the Helsinki Declaration and participation only commenced after written informed consent was obtained. Illiterate patients had the consent form read to them and signed using a fingerprint.
Results
Participation and demographics
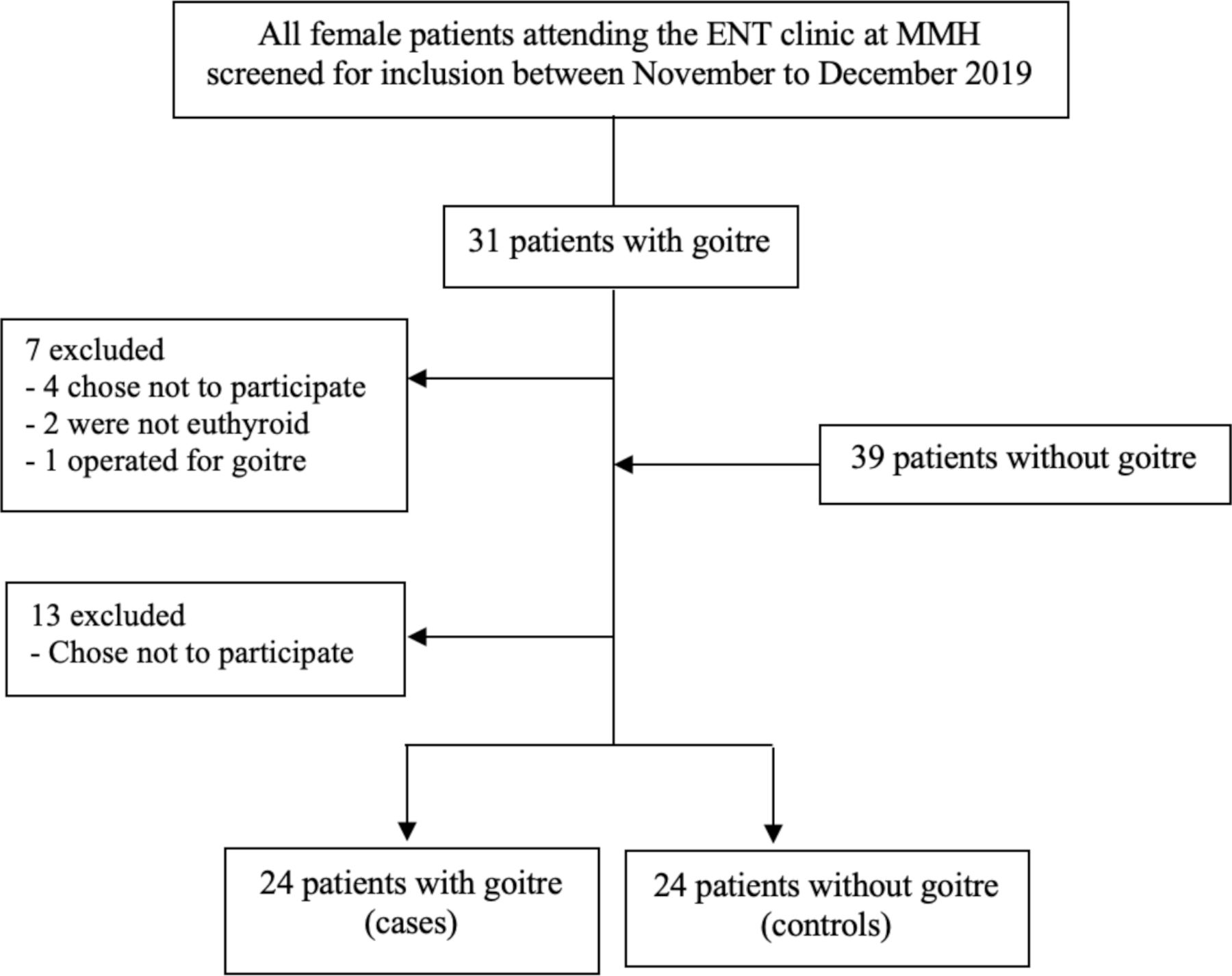
The study population included a total of 48 female patients: 24 with goitre (cases) and 24 without goitre (controls) as presented in figure 1. The average age was 38 years (range 19–60 years) and the average BMI was 25 kg/m2 (range 16–38 kg/m2). The two study groups were similar regarding education level, rate of employment, marital status and number of children. However, the majority of the controls lived in the town area that comprised less than half of the cases. The demographic background characteristics of the study participants are presented in table 1. The blood test results confirmed that the enrolled patients were euthyroid with serum TSH levels within the laboratories normal range (0.34–5.6 μIU/ml) (data not shown).

Flowchart of the patient participation. During enrolment, the patients without goitre were selected in order to match 1:1 in age (±5 years) with the patients with goitre. ENT, ear-nose-throat; MMH, Mnazi Mmoja Hospital.
Demographic background characteristics of the study population, n=48
Urinary iodine concentration
A MUIC of 100 µg/L corresponds roughly to the recommended daily intake for adults of 150 µg of iodine per day.16 The MUIC was below this level for both the cases and the controls, as presented in figure 2, suggesting a moderate iodine deficiency (MUIC between 20 and 49 µg/L) in both study groups. One outlier among the controls increased the MUIC of this group considerably from 21.5 µg/L without the outlier to 31.4 µg/L when included. The mean values were right shifted compared with the median values indicating a skewed distribution (online supplemental table 1). The mean difference was not statistically significantly different (30.7 µg/L, 95 % CI 17.4 to 78.8, p=0.2).
Supplemental material

{kind=link}
{kind=link}
Median urinary iodine concentration of the study population. Cases=patients with goitre, n=24; controls=patients without goitre, n=24. Box plot details: the horizontal black lines indicate the median (43.9 µg/L for the cases, 31.4 µg/L for the controls); the boxes indicate the IQR (25–75th percentiles); the whiskers represent observations within 1.5 times the IQR and the circles mark outliers more than 1.5 times the IQR. The recommended cut-off point for adequate iodine status in adults (100 µg/L) is marked with the red solid line. Values below this line correspond respectively to mild (<100 µg/L), moderate (<50 µg/L) and severe (<20 µg/L) iodine deficiency.
Iodine concentration of household salt samples
The salt samples from the cases had a lower average concentration of iodine compared with the controls as presented in table 2. These concentrations were slightly lower than the recommended iodine fortification level (>15 mg/kg)1 for the cases, compared with an average iodine content slightly above that level for the controls. The majority of the total patient population (n=31, 65%) provided salt from their household that was inadequately iodised. The household salt samples were inadequately iodised (<15 mg/kg) in the majority of the samples from the cases (n=18/24, 75%) and in over half the controls (n=13/24, 54%) (OR 2.5, 95 % CI 0.8 to 8.6).
Mean iodine concentration of household salt samples in the study population, n=48
Salt production, importation and storage practices
The majority of salt consumed in Zanzibar was imported from mainland Tanzania or neighbouring countries such as Kenya. Rock salt was transported to Zanzibar in 50 kg bags and stored in large containers in village centres or placed in smaller plastic bags sold at markets and shops. The iodine contents were unknown as the amount was often not specified on the packaging. Refined table salt was imported in 500 g packets from countries such as Tanzania, Kenya and India. Four commonly sold brands fortified the salt with potassium iodate and iodine concentrations specified on the packaging varied between 30–60 mg of iodine per kg of salt.
Dietary intake
As presented in table 3, the FFQ revealed that the daily consumption of marine fish was higher among the cases compared with the controls. The intake of other seafoods was less frequent in both study groups, and the intake of seaweeds was uncommon. Furthermore, regular consumption of fresh milk was reported more frequently among the cases but not consumed daily among the controls. The intake of yoghurt was similar in both study groups, and the intake of eggs was less common, but the weekly intake was slightly higher among the controls than the cases. Furthermore, the daily and weekly consumption of white bread was slightly higher among the cases than the controls. The daily consumption of iodised table salt was also slightly higher among the controls than the cases. Two of the cases did not cook or purchase their own food and reported ‘unknown’ when questioned about this condiment. In Zanzibar, the concentration of iodine in potentially important dietary sources of the micronutrient are to our knowledge unknown.
Frequency of consumption of some of the potential iodine-containing and goitrogenic foods in the study population, n=48
Of the potential goitrogens, the weekly consumption of both raw and cooked cassava was found in a higher proportion of the cases than the controls. Additionally, sweet potato was used almost as frequently as cooked cassava in both study groups. Intake of cruciferous vegetables was uncommon (data not shown). A difference in daily intake of sorghum and millet was found, where the daily consumption among the cases was higher than among the controls. However, sorghum flour was more frequently used in both study groups than sorghum. A mix of flours including sorghum flour, millet grain and maize flour were frequently combined with water and salt to produce a local porridge called Uji. To our knowledge, the goitrogenic properties of food items in Zanzibar have yet to be investigated.
Discussion
The results from the urine analysis revealed a moderate iodine deficiency in both the cases and controls, presumably caused by an inadequate dietary intake of iodine. These findings suggest that iodine deficiency may be a problem in patients with goitre and also in patients without goitre in Zanzibar. The FFQ raised questions about the iodine and goitrogen content of local foods produced and consumed in Zanzibar, as intakes were similar in both groups. Furthermore, the salt analysis demonstrated that the average concentration of iodine in household salt was lower in the cases than the controls. Thus, an important dietary source of iodine varied between the two study groups. Nevertheless, the salt samples were inadequately iodised in 65% of the total study population, suggesting that the salt iodisation programme in Zanzibar requires monitoring and an implementation of satisfactory quality control practices.
Iodine status
The number of available studies on adult iodine nutrition in Zanzibar are sparse. A few surveys have been performed on school-age children (SAC) both in Zanzibar and mainland Tanzania and one survey has included WRA.7 8 17 The present findings differ from the results of the Tanzania Demographic Health Survey from 2015 (TDHS-15).7 A considerably higher MUIC compared with the present study was reported in WRA on Unguja island7 indicating above adequate iodine nutrition in the population.1 In 2006, a cross-sectional survey on SAC in Unguja also reported adequate iodine intakes where no district had a MUIC below 100 µg/L.8 However, a mild iodine deficiency was reported in SAC on Pemba island with results similar to the present study.8 Similarly, a national survey conducted in 2004 on children in mainland Tanzania reported that 25% of the SAC had a UIC below 100 µg/L.17
The TDHS-15 survey reported that the MUIC for Tanzania (including Zanzibar) declined significantly with increasing age.7 These findings are supported by other studies reporting that UIC declines with age, possibly due to poorer dietary intake among elderly or as a consequence of restricted salt intakes.18 19 A noteworthy difference between the present study and the former studies is an older patient population (range 19–60 years), compared with WRA (15–49 years) and SAC. The lower MUIC levels in the present study could therefore be related to a considerably older study population. Additionally, considering that the UIC of men has been reported to be slightly higher than women,18 the lower MUIC levels found in the present study could be related to gender. Notably, there is also a number of years between the present study and the previous studies where the iodine status of both SAC and WRA may have changed during this time.
Dietary iodine intake
Iodine-containing foods and goitrogens
In the present study, the patients consumed foods commonly known to be good sources of iodine, yet the urine analysis indicated a moderate iodine deficiency. We are not aware of information on the iodine or goitrogenic content of different foods in Zanzibar and thus cannot describe a relationship between the intake reported in the FFQ and the thyroid function, development of goitre or iodine deficiency in this study population. The study observed that the daily consumption of seawater fish was more frequent in the cases than the controls, yet the cases still developed goitre. On the other hand, all cases and 92% of controls consumed marine fish weekly (varying from one to seven times a week). As marine seafood is generally a good source of iodine,20 the results imply that either the amounts consumed were too small to cover adult iodine requirements or that the iodine content of the fish consumed was low.
In terms of goitrogens, they have a major clinical effect when an iodine deficiency is present;5 21 22 hence, the importance of limiting their intake and using appropriate food processing practices in this population is noteworthy. The root vegetable cassava is largely consumed in developing countries20 including the present population. As raw cassava contains goitrin, which metabolises and competes with iodine for thyroidal uptake, it is recommended that it be prepared or processed to reduce the goitrogenic potency.22 Regular consumption of raw cassava is not advised. Despite this, the weekly consumption was reported in 21% of the cases and 13% of the controls.
Iodised salt
In the present study, 69% of the salt samples contained iodine. These proportions differed slightly from the TDHS-15, where 88% and 54% of women in Unguja and Pemba, respectively, lived in households with iodised salt.7 In the present study, the ICP-MS quantification method for iodine revealed that only 35% of the salt samples were adequately iodised (>15 mg/kg). Similarly, the TDHS-15 survey tested 60 salt samples from Unguja using the titration method and found only 46% to be adequately iodised.7 Therefore, when comparing the present results to a recent survey applying similar methods, the findings were more alike. On the contrary, in studies where the rapid test kit method was used, higher proportions of iodised salt were reported.8 17
Nevertheless, the present findings and earlier surveys emphasise that the iodisation programme in Tanzania (and especially Zanzibar) is not satisfactory. In 1994, WHO, The United Nations Children’s Fund and the Iodine Global Network recommended universal salt iodisation (USI) as a safe, sustainable and cost-effective strategy to ensure sufficient iodine intake in populations.6 Several factors can limit progress towards USI. First, enforcing legislation on iodisation of salt and establishing operational monitoring systems can be difficult to accomplish where strong partnerships are required among stakeholders.9 23 Second, one of the main challenges in Tanzania is iodine intakes varying across the country due to salt being supplied by hundreds of small-scale suppliers producing iodised salt with variable quality.3 In most countries, quality control of iodisation methods is feasible as salt production is limited to a few centres.24 Last, supplying populations living in remote areas without easy access to iodised salt remains a challenge.23 Zanzibar is reached by sea or air, and access to iodised salt depends on importation from mainland Tanzania and neighbouring countries. Despite variations in methods, the present study and previous surveys have not documented USI being achieved in Zanzibar, although results from mainland Tanzania have been more promising. The Tanzanian regulations for iodised salt state that the level of iodine should be between 40–80 parts per million (ppm) at production or importation and 25–70 ppm at the point of sale.25 However, the iodisation of salt appears inconsistent, and quality control and monitoring is necessary at the national level. Iodine losses should be determined by investigating local conditions of production, climate, packaging and storage of iodised salt.24
Study strengths and limitations
The present study contributes to new knowledge where the MUIC and iodine content in salt were compared in two female patient populations in Zanzibar. To our knowledge, this is the first case-control study performed on female patients with and without goitre in Zanzibar.
The present study included only female patients and due to differences in thyroid hormone production and dietary intakes between males, females and children, the results may not apply to males of equivalent age or to children. There may also be a difference in the iodine status of patients at a hospital compared with healthy individuals in the general population of Zanzibar. However, the investigated study population had no known severe illnesses that might have had large detrimental effects on their nutritional status and dietary intakes. The design of the present study renders the generalisation of results to the remaining population of Zanzibar questionable due to the small sample size and potential bias in the selection process. Further investigations could aim to include a substantially larger study population with participants outside the hospital setting. Additionally, the FFQ was created for this study and was not validated before use. Although the FFQ was not used to quantitatively assess iodine intake, future research could aim to appropriately validate the FFQ.
Conclusion
The present study revealed a moderate iodine deficiency in a female adult patient population with and without goitre in Zanzibar. There was a difference in average iodine content of household salt samples analysed, which was lower in the cases than the controls. The majority of salt samples were inadequately iodised, emphasising the need for quality control. The findings suggest that Zanzibar does not have optimal iodine nutrition despite being surrounded by the ocean with access to fish and seafoods. Overall, the results emphasise the need for further investigations into the iodine status of the inhabitants of Zanzibar.
Data availability statement
Deidentified participant data are available from Hanne Rosendahl-Riise (Hanne.rosendahl-riise@uib.no/ORCID 0000-0002-1497-416X) on reasonable request.
Ethics statements
Ethics approval
Ethical approval for the study was provided by the Western Norwegian Regional Committee for Medical and Health Research Ethics (ref. no. 2019/759) and from the Zanzibar Health Research Institute (ref. no. ZAHREC/03/ST/NOV/2019/23).
Acknowledgments
We would like to thank the health workers at the ENT clinic of MMH for their assistance and cooperation throughout the data collection in Zanzibar. Furthermore, we would like to thank the study participants for their time, patience and contributions. Last, we would like to thank Tasakthaa Global Hospital, Dar Es Salaam Institute of Technology and the Norwegian Institute of Marine Research for respectively conducting the blood, urine and salt analysis.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ingunnengebret1
Contributors OB contributed to the conception, study design, execution, acquisition of data, analysis and interpretation of findings, wrote the first draft and led the editing of the reviewed article. EMCV contributed to the conception, study design, acquisition of funding and revising and critically reviewing the article. IMSE contributed to the conception, study design and revising and critically reviewing the article. NKM contributed to the execution/data collection and reviewing the article. TS contributed in the conception and reviewing the article. HR-R contributed to the conception, study design, project administration, acquisition of funding and made significant contributions to drafting, revising and critically reviewing the article. All authors gave final approval of the version to be published, agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding This study was supported by the Mohn Nutrition Research Laboratory, Centre for Nutrition, University of Bergen, Norway and the Department of International Collaboration at Haukeland University Hospital, Norway.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed by Dr Surya Bali, AIIMS Bhopal, India.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.