Article Text

Abstract
Background The double burden of malnutrition (DBM), which refers to the coexistence of overnutrition and undernutrition among populations, households or individuals, is a growing problem in low/middle-income countries. The Latin America and the Caribbean (LAC) region has been particularly affected by the DBM, following a nutrition transition and a rapid increase in overweight, obesity and diet-related disease, while high levels of undernutrition persist. This study aims to describe the prevalence of four different DBM definitions in mother–child pairs across nine LAC countries and investigate the socioeconomic determinants of overweight mothers with at least one stunted child (SCOM).
Methods We used cross-sectional data from the Demographic and Health Surveys for all analyses. We used descriptive statistics to obtain prevalence rates and conducted multiple logistic regression analyses to investigate the association between SCOM households and socioeconomic determinants, including wealth index, maternal education, place of residency and whether the mother was working, adjusted for a range of variables.
Results Overweight/obese mothers with at least one anaemic child were the most common type of DBM, with a prevalence of 19.39%, followed by SCOM with a prevalence of 10.44%. Statistically significant socioeconomic predictors of SCOM were households with a lower wealth index, lower maternal education and living in rural areas.
Conclusion This study showed that the overall prevalence of most DBM definitions examined was high, which points to the need for urgent interventions in the LAC region. The unique set of socioeconomic predictors of SCOM identified in this study calls for future double-duty policies that simultaneously target food affordability, nutrition education and access to healthy food.
- malnutrition
Data availability statement
Data are available in a public, open access repository. All data are available through the Demographic and Health Surveys (DHS) Programme at www.dhsprogram.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The double burden of malnutrition is an increasing issue in low/middle-income countries, specifically in Latin America and the Caribbean region. With this study, we add a comprehensive and region-specific insight into the current situation.
WHAT THIS STUDY ADDS
Lower maternal education, lower wealth index, and urban residency were shown to be determinants of households with overweight mothers and a stunted child.
A high prevalence of overweight mothers with at least one anaemic child was found, highlighting the need for further investigation of this issue in Latin America and the Caribbean context.
We identified diversity in the socioeconomic predictors of households with overweight mothers with a stunted child, households with overweight mothers and non-stunted children, and households with stunted children and normal weight mothers stipulating the importance of targeting the double burden of malnutrition as a unique issue.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Future double-duty policies must simultaneously target food affordability, nutrition education and access to healthy food.
Introduction
The double burden of malnutrition (DBM) is an emerging phenomenon, defined as the co-occurrence of undernutrition and overnutrition within populations, households and individuals.1 The DBM has coincided with the accelerated global food and nutrition transition in low/middle-income countries (LMICs) driven by rapid economic development and urbanisation.1 2 The nutrition transition often leads to changes in diet composition towards higher consumption of energy-dense ultra-processed foods,2–5 which results in rapidly increasing overweight and obesity rates, while undernutrition rates are staying constant or are declining at a slower pace.1 6–8
The Latin America and the Caribbean (LAC) region is one of the regions with the greatest DBM prevalence worldwide.9 10 In the last decades, the average prevalence of the DBM at the household level was around 10% globally.11–13 However, a study from 2020 found that from 10 investigated countries in the LAC region, 6 had a prevalence above 10% ranging from 11.24% in Peru to 24.34% in Guatemala.13 Although LAC countries have progressed in decreasing undernutrition and micronutrient deficiencies in the past years, these are still at high and at unequal levels.8 14 At the same time, LAC was one of the first regions to encounter a nutrition transition that changed the nutritional environment, as early as the 1980s, leading to increasing levels of overweight and obesity.15 Further, ultra-processed food sales surged by 43.7% from 2000 to 2013 throughout the LAC region, while sales in carbonated soft beverages even doubled.16 Overall, LAC countries have an elevated added sugar consumption, exceeding up to three times the WHO recommended level.15 17 In a sample of almost 10 000 participants across eight LAC countries, only 7.2% met the recommended serving of fruits and vegetables per day.18
Previous studies already point to possible determinants of DBM; however, these mainly showed heterogeneous results that differ across regions. A study that examined the DBM at the individual level in the Middle East and North Africa and the LAC regions found that the prevalence and social patterning of the DBM differs widely across the regions.19 Further, a global analysis of household-level DBM in LMICs showed that the association between DBM and household wealth differed based on country income, with the probability of DBM being higher among wealthier households in lower-income countries and poorer households in higher-income countries.20 This underscores the necessity to understand the role of socioeconomic determinants on the DBM at the regional level.
As of our knowledge, there is no previous comprehensive analysis of socioeconomic determinants of household-level DBM in the LAC region.5 11 21 Existing studies were only descriptive,6 10 focused on individual-level DBM19 or only included limited countries.5 21 With this study, we would fill this gap by examining the prevalence of different types of household-level DBM in nine LAC countries and investigating associations with socioeconomic characteristics using the most recent Demographic and Health Surveys (DHS) data.
Methods
Study design
For this study, we used observational data from the DHS from nine LAC countries between 2001 and 2017 (www.dhsprogram.com). The DHS is a repeated cross-sectional household survey that collects data from women aged 15–49 years and their children below 5 years for several LMICs across the world.22 It includes demographic, economic, health and nutrition data.22 The surveys are commonly representative at the national, residence and regional levels, and their standardised design allows for cross-national comparison.22 23 The DHS uses a multistage stratified probabilistic sampling design, with households randomly selected from a sample of census enumeration areas.22 23 More information on the sampling strategy can be found elsewhere.22 23 For this study, we used the individual DHS weights considering stratification and clustering, to adjust for sampling design and non-response.
Study population
We selected the most recent surveys available for all LAC countries that included anthropometric data. This results in data from Bolivia, Colombia, Haiti, Honduras, Dominican Republic, Guyana, Guatemala, and Peru between 2001 and 2017. The final dataset included all households with complete anthropometric data for mothers of reproductive age (15–49 years) with at least one child aged 0–5 years of either sex. We excluded pregnant mothers and mothers who had given birth 2 months before the interview to avoid inaccuracies in the measurement of body mass index (BMI). Further, women with a BMI above 60 were considered outliers and excluded. These exclusions yielded a final sample of 48 807 mother–child pairs. For the logistic regression analysis, a further 9433 mother–child pairs were excluded due to missing data of covariates as a complete case analysis was conducted, resulting in a total sample size of 39 374. A detailed flow chart about the exclusion process can be found in online supplemental appendix A and a table stating the missing values per variable can be found in online supplemental appendix B.
Supplemental material
Outcome
As a primary outcome, we used a measure for SCOM households (overweight mother with at least one stunted child), which was coded 1 if the mother was overweight or obese and at least one of her children was stunted, and 0 if the mother was not overweight and/or none of her children were stunted. We also explored SCOM across four categories: first, normal households, with a non-overweight mother and non-stunted children; second, stunted households, with a non-overweight mother with at least one stunted child; third, overweight households, with an overweight mother with non-stunted children; and fourth, SCOM households. We defined overweight or obesity for the mother as having a BMI (BMI=weight in kg/height in m2) equal to or greater than 25 kg/m2, following the WHO for standard practice.22 Further, we defined a stunted child as having a height-for-age z-score that was two SDs below the median, following the most recent WHO international growth reference curves.22 24
In addition to the primary outcome, we also explored the prevalence of several other DBM definitions. These include overweight mothers with at least one wasted child (WCOM), overweight mothers with at least one anaemic child (ACOM) and anaemic mothers with at least one overweight child (OCAM). We defined wasted children as having a weight-for-age z-score with more than two SDs below the median, and overweight children as having a weight-for-age z-score of more than two SDs above the median, following the WHO international age-specific growth reference curves.22 24 We defined children as anaemic if they had a haemoglobin concentration below 110 g/L and non-pregnant mothers as anaemic if they had a haemoglobin concentration below 120 g/L.22
Explanatory variables
The explanatory variables in this study consist of four socioeconomic variables: location of residency (urban/rural); maternal education (no education/incomplete primary, complete primary/incomplete secondary, secondary and higher); whether the mother was working in the last 12 months (categorised as yes if the mother was working in the past 12 months, currently working at the time of the interview, or had a job but was on leave in the last 7 days, and categorised as no, if she did not work in the past 12 months). We also measured relative household wealth, using the DHS wealth index.23 25 The wealth index is a compound indicator of the household’s aggregated living standard. It is estimated based on the household’s ownership of certain goods and services such as television, bicycles, materials used for housing construction, type of water access and type of sanitation facilities.25 The wealth index ranks the households on a continuous scale of relative wealth which was then divided into a categorical variable of five quintiles, namely, poorest, poor, middle, richer and richest.22 25 We further adjusted our analyses for sex (percentage of mothers’ children who are girls), mean age of the children, age of the mother, number of children below 5 years living in the household and whether the husband is living at home.
Statistical analysis
We described population characteristics using weighted means and SDs or N and weighted frequencies. Further, we estimated the prevalence of the different DBM definitions in the LAC region overall and across socioeconomic groups. We tested differences between groups using a X². Afterwards, we performed bivariate and multiple logistic regression analyses to identify predictors of SCOM. First, we tested each socioeconomic variable (wealth index, maternal education, location of residency and whether the mother worked in the last 12 months) individually and combined to check whether they were predictors of SCOM. Second, we adjusted for all covariates and country fixed-effects. Country fixed-effects adjust for unobserved differences between countries. Afterwards, we conducted a multinomial logistic regression analysis to test the probability of observing a SCOM household, overweight household or stunted household compared with a normal household, after adjusting for relevant covariates and country fixed-effects. Lastly, we performed a sensitivity analysis with two age-stratified multiple logistic regression models to estimate associations in children below 3 years (0–2 years) and children aged 3 years and above (3–5 years). This was done due to potential variability in the reliability of anthropometric data for younger children.26 For all analyses, we chose a statistically significant level of 0.05 and reported adjusted ORs with a 95% CI and used robust SEs clustered by country. For all analyses, we used Stata V.15.27
Results
Descriptive analyses
Characteristics of the study population
Table 1 displays a detailed description of baseline household characteristics of SCOM households and non-SCOM households in the sample. Across the different LAC countries, SCOM prevalence ranged from 3.22% to 21.14%. Further country-specific characteristics can be found in online supplemental appendices C and D. All characteristics, besides whether the husband was living at home, showed a statistically significant difference between SCOM and non-SCOM households. Overall, mothers in SCOM households appeared to have a higher average age compared with mothers in non-SCOM households. SCOM households were more likely to live in rural areas and have lower wealth index compared with non-SCOM households. The same pattern was found for maternal education level, with mothers living in SCOM households being more likely to have lower education level compared with mothers in non-SCOM households. Lastly, there were slightly more children below 5 years living in a SCOM household compared with a non-SCOM household.
Characteristics of the study population, overall and by SCOM (overweight mothers with at least one stunted child)
Prevalence of DBM types
Across LAC, SCOM had an overall prevalence of 10.44% from 48 807 examined households. WCOM had a low prevalence, with only 241 of 48 707 (0.48%) examined households having WCOM, while ACOM was observed in 5062 (19.39%) of 25 684 examined households. Lastly, OCAM had a prevalence of 5.76%, with 451 OCAM households from 8507 total households (online supplemental appendix E).
Figure 1 shows the distribution of the different outcomes across location of residency, maternal education level, wealth index and whether the mother was working in the last 12 months. A detailed table can be found in online supplemental appendix F. The distribution of SCOM and OCAM was significantly different between urban and rural households, with more households with SCOM living in rural areas (56.2% vs 43.8%) and more households with OCAM living in urban areas (56.4% vs 43.96%). The DBM also differed across wealth index quintiles, although the patterning of this variation was different across DBM types. The majority of SCOM households were in the poorest quintile, while the majority of ACOM and OCAM households were in the middle and richest quintile, respectively.
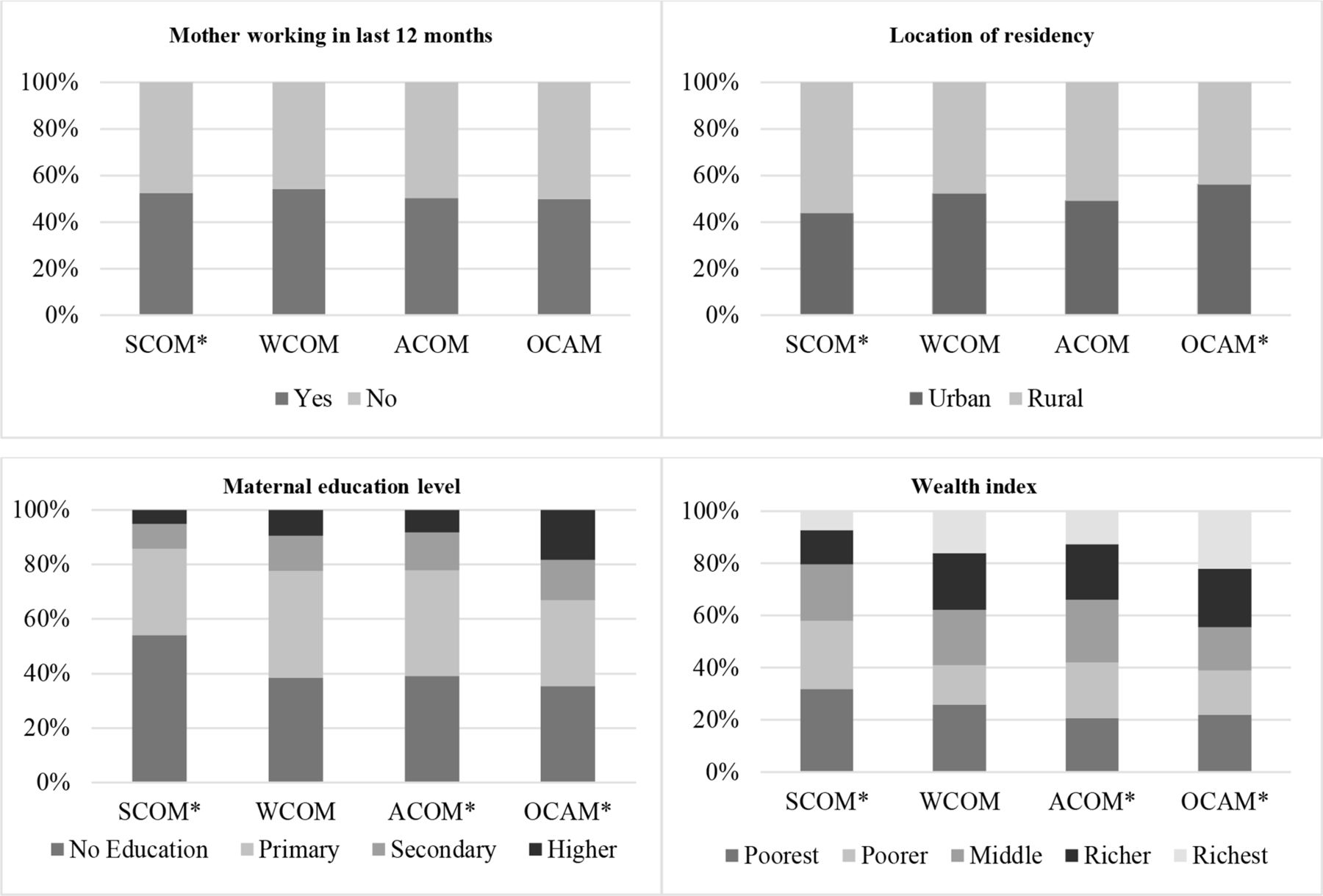
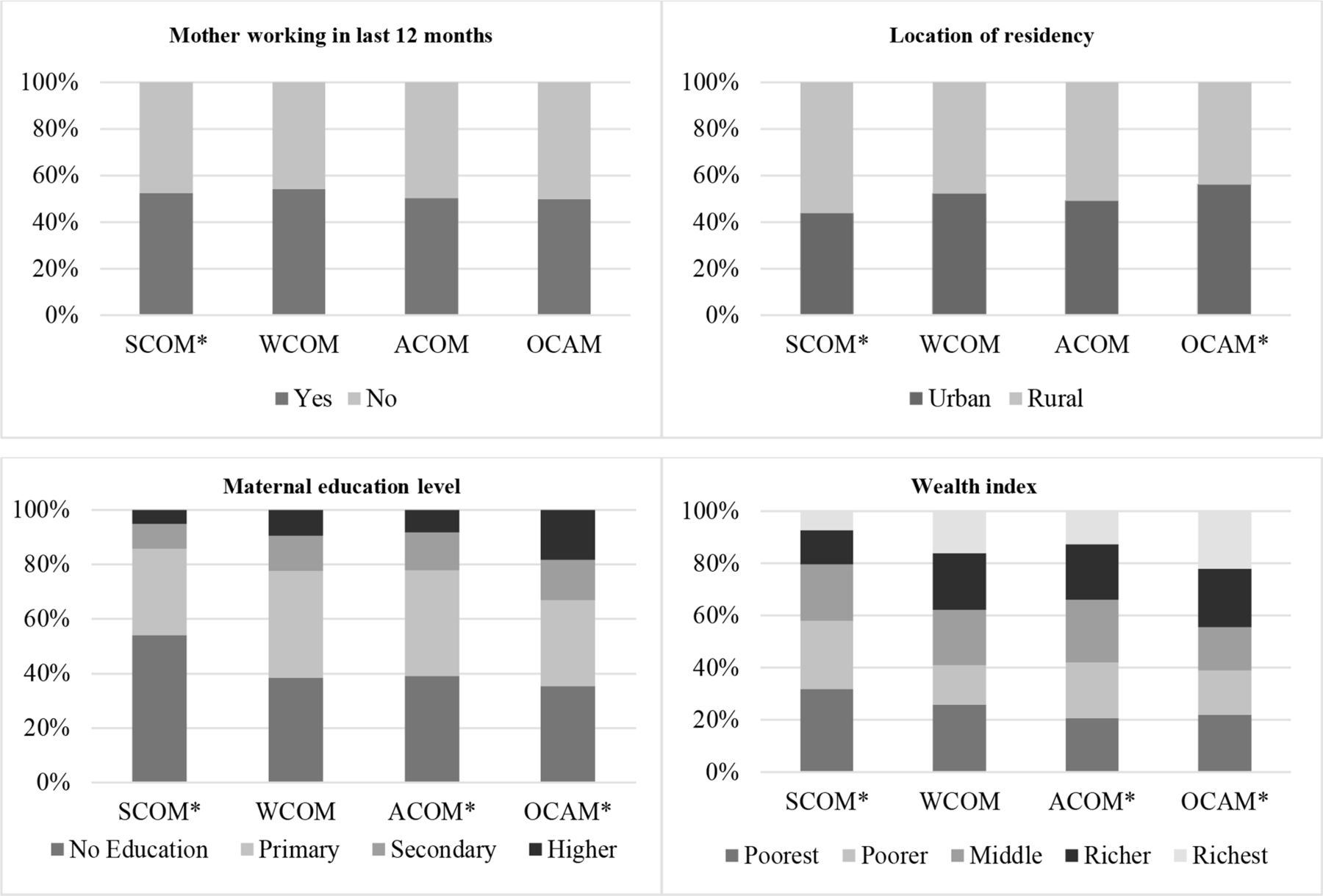{kind=link}
Distribution of overweight mother with at least one stunted child (SCOM), overweight mother with at least one wasted child (WCOM), overweight mother with at least one anaemic child (ACOM), and anaemic mother with at least one overweight child (OCAM) households across location of residency, maternal education level, wealth index, and whether the mother was working in the last 12 months (per column). * indicates significance (Χ2 p<0.05).
Model results
Multiple logistic regression analyses and sensitivity analysis
Table 2 depicts the associations between SCOM households and socioeconomic characteristics. After adjusting for relevant covariates, location of residency and wealth index were predictors of SCOM households, with the richest households and those living in a rural area having a 57% (OR=0.43, 95% CI (0.35 to 0.55)) and 18% (OR=0.82, 95% CI (0.70 to 0.96)) lower probability of being a SCOM household compared with the poorest and urban households, respectively. Further, the mother’s educational level was a SCOM predictor with mothers with higher education being 55% (OR=0.45, 95% CI (0.34 to 0.59)) less likely to be a SCOM household compared with mothers with no/incomplete primary education. Whether the mother was working in the past 12 months was not found to be a SCOM predictor in this study. The stratified sensitivity analysis for children below and above 3 years showed similar results to the unstratified model (online supplemental appendix G) suggesting no significant differences between age groups.
Multiple logistic regression analysis for associations between an overweight mother with at least one stunted child (SCOM) and socioeconomic determinants, n=39 374
Multinomial logistic regression analysis
We used a multinomial model to examine whether determinants of SCOM households were also determinants of other types of household malnutrition, namely, overweight households and stunted households (table 3). Educational level was a predictor of stunted, overweight and SCOM households, with mothers of higher education having a 61%, 36%, and 67% lower probability of being in a stunted, overweight, and SCOM household, respectively, compared with normal households. Further, being in the richest quintile was associated with an 84% and 58% lower probability of being a stunted or SCOM household, respectively, compared with normal households. However, associations between overweight households and wealth index had an opposite direction, with households in the richest wealth quintile having a two times higher risk of being an overweight household compared with a normal one (OR=2.08; 95% CI (1.41 to 3.07)). Further, living in rural areas was associated with a higher probability of being a stunted household (OR=1.16; 95% CI (1.03 to 1.30)) and a lower probability of being a SCOM household (OR=0.81; 95% CI (0.70 to 0.93)), while no associations were observed between the location of residency and being an overweight household. Lastly, whether the mother was working in the last 12 months was associated with a slightly higher probability of being a stunted, overweight and SCOM household.
Multinomial logistic regression analysis for associations between household malnutrition (non-overweight mother/stunted child, overweight mother/non-stunted child, overweight mother/stunted child (SCOM)) and socioeconomic determinants compared with non-overweight mothers and non-stunted children, n=39 374
Discussion
This study aimed to identify prevalence rates of four different DBM definitions and to identify socioeconomic determinants of SCOM households in nine LAC countries. The main results of this study showed that ACOM had the highest prevalence among all DBM definitions, followed by SCOM and OCAM, while WCOM had a low prevalence, potentially due to the low overall wasting prevalence in the LAC region. There were significant differences in the prevalence of DBM across groups of maternal education level, wealth index, location of residency and whether the mother was working in the last 12 months, although the patterning of these differences varied across DBM definitions. Further, a higher maternal education level, a higher wealth index and living in a rural area were associated with a lower probability of SCOM. Lastly, comparing SCOM, overweight and stunted households with normal households showed that while they do share some determinants, overall, they differed.
Our results indicate that the prevalence of SCOM was above 10% across all nine countries with two countries having a prevalence of above 10% and Guatemala reaching a prevalence of 21.14%. This is in accordance with a recent study that found SCOM prevalence ranging from 5.63% to 24.34% in the LAC region.13 Further, our study identified an alarmingly high prevalence rate for ACOM in LAC that needs to be further investigated, especially, given the lack of relevant research, with the majority of previous studies investigating the double burden of overweight and anaemia at the individual level only.28 One study in Ecuador, which did look at household level ACOM, found a prevalence of 12.6%; however, data for other LAC countries lack.29
Our analysis suggests that the risk of being a SCOM pair was lower for wealthier households compared with poorer households. This is in accordance with previous studies that suggest that socioeconomic status, poverty or food insecurity were also associated with higher probability of SCOM in LMICs, in LAC and across the world.30 31 Further, a recent study found that SCOM was associated with a higher household wealth in lower-income LMICs but with lower household wealth in higher-income LMICs.20 Considering that the majority of countries in LAC are higher-income LMICs, this would also reflect the results of our study. In this study, we found that a higher maternal educational level was associated with a lower risk of SCOM compared with a lower education level, which is mostly consistent with previous research.21 30 32 33 Only one study found no association between SCOM and educational level; however, household wealth was not taken into account.11 Our analysis showed that households who lived in rural areas had a lower risk of being a SCOM pair than households who lived in urban areas. Previous studies found quite heterogeneous results regarding the location of residency.5 11 30 34 35 A global study suggested that SCOM was associated with rural residency in Africa and Asia, but urban residency in Latin America.5 As previously suggested, associations between household-level socioeconomic characteristics, including urban/rural residency, and SCOM differ across countries according to country income.20
We identified that lower maternal education level was not only a predictor of SCOM households, but also of stunted and overweight households when compared with normal households. However, this was not the case for wealth index and location of residency which showed inconsistent associations with different types of household malnutrition. Similar analysis among South-East Asian countries further supports diversity between the socioeconomic predictors of SCOM, overweight and stunted households, although identified predictors are not consistent with the findings of this study.36 This suggests that each malnutrition issue may be the result of different socioeconomic circumstances and should be handled uniquely, while it further highlights the importance of region-specific analyses when investigating socioeconomic predictors of the DBM.
Strengths and limitations
A strength of this study is the large sample size from high-quality nationally representative surveys with a standardised methodology that allows comparison between countries.22 The precise focus on the LAC region is valuable given the previously described diversity of socioeconomic determinants of the DBM across regions. Lastly, we included the prevalence of four different household-level definitions of DBM, including anaemia, for which research in the LAC area is currently limited.
However, this study also had some limitations. First, it must be considered that the study design of the DHS data is cross-sectional and no causal relationships can be concluded. Further, due to data availability, our results are based on mother–child pairs with children below the age of 5 years only and cannot provide information for the DBM in older children. Also, we did not differentiate between a mother who had only one stunted child and a mother where all her children are stunted, which may have showed different results. Also, comparisons between wealth index across countries should be interpreted with caution, as wealth index is a measure of relative wealth that is country specific. Lastly, even though we adjusted for several confounders, there is always the possibility of residual confounding due to unmeasured factors.
Implication for future policy
To sustainably tackle the DBM, the WHO recommends double-duty actions that simultaneously target undernutrition and overnutrition.37 They are defined as: actions that ensure no harm is caused on other types of malnutrition by targeting a single malnutrition issue, existing interventions retrofitted to address multiple forms of malnutrition or new interventions that are specifically designed to target DBM.37 38 In the past, the focus of food policy in the LAC region was on undernutrition, and policies regarding overweight and obesity were limited.8 38 39 Some evidence even suggests that policies targeting undernutrition inadvertently increased the risk of overweight and obesity.38 Recently, LAC countries have been global leaders in implementing bold policies targeting obesity.8 15 However, to our knowledge, there is still a lack of double-duty policies in the LAC region which are ultimately needed to tackle the DBM and reach the 2.2 Sustainable Development Goal to end malnutrition in all its forms.37 38
In line with our results suggesting that higher educational level and higher wealth indicate a reduced risk of SCOM, policies that target both are needed to address overnutrition and undernutrition together.37 38 One solution would be the reinvention of existing programmes in LAC to align with double-duty goals. For example, cash assistance programmes should also target health literacy, to avoid an increase in purchases of unhealthy foods. Similarly, school food programmes should not offer ultra-processed foods, as ultra-processed food provision might increase consumption and demand for these products, resulting in unintended side-effects on overnutrition outcomes. Overall, policies should target household food security while also recognising the crucial role of food quality, healthy food access and health literacy in achieving double-duty goals.
Conclusion
In conclusion, with this study, we provide a comprehensive investigation of household-level DBM and its socioeconomic determinants in the LAC region. The study shows that lower maternal education level, lower household wealth and urban location of residency are significant determinants of SCOM. Our study points to the need for appropriate double-duty actions that target the DBM as a single issue.
Data availability statement
Data are available in a public, open access repository. All data are available through the Demographic and Health Surveys (DHS) Programme at www.dhsprogram.com.
Ethics statements
Patient consent for publication
Ethics approval
There was no need for an ethical review in this study, as all data used are openly available to the public. All DHS have been reviewed and approved by the ICF Institutional Review Board (IRB) and by IRBs in each host country. All participants gave informed consent. More detailed information can be found elsewhere.
References
Footnotes
Contributors HSO drafted the manuscript and conducted the statistical analyses. Both authors contributed to the conceptualisation, methodology, editing and revising of the final manuscript. HSO acts as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed by Dr Tulsi Adhikari, ICMR-National Institute of Medical Statistics, New Delhi, India and by Dr Dickson Abanimi Amugsi, African Population and Health Research Center Maternal and Child Wellbeing Unit, Nairobi, Kenya.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.