Article Text

Abstract
Background Many patients are already malnourished when admitted to hospital. Barriers and facilitators to nutrition care in hospital have been identified and successful interventions developed; however, few studies have explored how to sustain and spread improvements. The More-2-Eat phase 1 study involved five hospitals across Canada implementing nutrition care improvements, while phase 2 implemented a scalable model using trained champions, audit and feedback, a community of practice with external mentorship and an implementation toolkit in 10 hospitals (four continuing from phase 1). Process measures showed that screening and assessment from phase 1 were sustained for at least 4 years. The objective of this study was to help explain how these nutrition care improvements were sustained and spread by understanding the role of the trained champions, and to confirm and expand on themes identified in phase 1.
Methods Semistructured telephone interviews were conducted with champions from each phase 2 hospital and recordings transcribed verbatim. To explore the champion role, transcripts were deductively coded to the 3C model of Concept, Competence and Capacity. Phase 2 transcripts were also deductively coded to themes identified in phase 1 interviews and focus groups.
Results Ten interviews (n=14 champions) were conducted. To sustain and spread nutrition care improvements, champions needed to understand the Concepts of change management, implementation, adaptation, sustainability and spread in order to embed changes into routine practice. Champions also needed the Competence, including the skills to identify, support and empower new champions, thus sharing the responsibility. Capacity, including time, resources and leadership support, was the most important facilitator for staying engaged, and the most challenging. All themes identified in qualitative interviews in phase 1 were applicable 4 years later and were mentioned by new phase 2 hospitals. There was increased emphasis on audit and feedback, and the need for standardisation to support embedding into current practice.
Conclusion Trained local champions were required for implementation. By understanding key concepts, with appropriate and evolving competence and capacity, champions supported sustainability and spread of nutrition care improvements. Understanding the role of champions in supporting implementation, spread and sustainability of nutrition care improvements can help other hospitals when planning for and implementing these improvements.
Trial registration number NCT02800304, NCT03391752.
- malnutrition
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study. As transcripts may be identifiable, interviews are not available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
This study explores how trained local champions supported the sustainability and spread of nutrition care improvements in multiple hospital units across Canada.
Having trained champions who demonstrate continual and evolving understanding of key concepts for implementation was necessary. With appropriate competence and capacity, champions support the sustainability and spread of nutrition care improvements.
As champions are key to implementation, spread and sustainability of nutrition care improvements in hospitals, this in-depth look at their role can support other hospitals to use this implementation strategy when planning for and implementing nutrition care improvements.
Introduction
Hospital malnutrition is common in newly admitted adult patients, with prevalence estimates ranging from 20% to 45%, depending on the population studied.1–3 A number of studies have been conducted to guide and implement a variety of best practices including the implementation of nutrition risk screening, assessment tools such as the subjective global assessment (SGA), and treatment options such as protected mealtimes.4 5 Multicomponent interventions have demonstrated improved nutrition care practices and outcomes, and there is increasing understanding of how to implement these interventions.6–13 However, little is known about how to sustain and spread those improvements, making this study unique in its focus on the role of trained champions in sustaining and spreading nutrition care improvements in hospitals. For this work, Moore et al’s14 definition of sustainability is used as it focuses on five main components regarding: time; continued delivery and implementation of the intervention; maintenance of individual behaviour change; recognition that the programme may continue to adapt; all in order to produce benefits for individual/systems14 (p 6). Spread is defined as ‘replicating an initiative somewhere else (ie, one site to another)’.15
Local champions are a key implementation strategy used to facilitate change,16–20 including for improving or facilitating nutrition care improvements in hospitals.21–23 Champions are included in many implementation frameworks including the Consolidated Framework for Implementation Research (CFIR), where they are defined as ‘individual(s) who dedicate themselves to supporting, marketing, and driving through an implementation, overcoming indifference or resistance that the intervention may provoke in an organization’.24 25 Although champions are mentioned frequently, and some key constructs and characteristics of champions have been explored,17 18 the literature in this field is underdeveloped,20 and details about the champion role are typically minimal, making it difficult to replicate the effect.18 In addition, the focus is typically on the role of champions during initial implementation, rather than how that role continues longer term or facilitates spread to other sites, thus leaving gaps in our understanding of the long-term role of champions and how the role changes over time. From the perspective of trialists of effective diabetes quality improvement interventions, key factors in sustainability and spread include the 3C’s of Concept, Competence and Capacity.26 Trialists suggested the importance of champions understanding the concepts of implementation, sustainability and spread, as well as having the competence and capacity to apply those concepts. The 3C model encompasses the constructs related to training champions and appears applicable for understanding the role of champions, and how they can be trained and supported in sustaining and spreading nutrition care improvements.
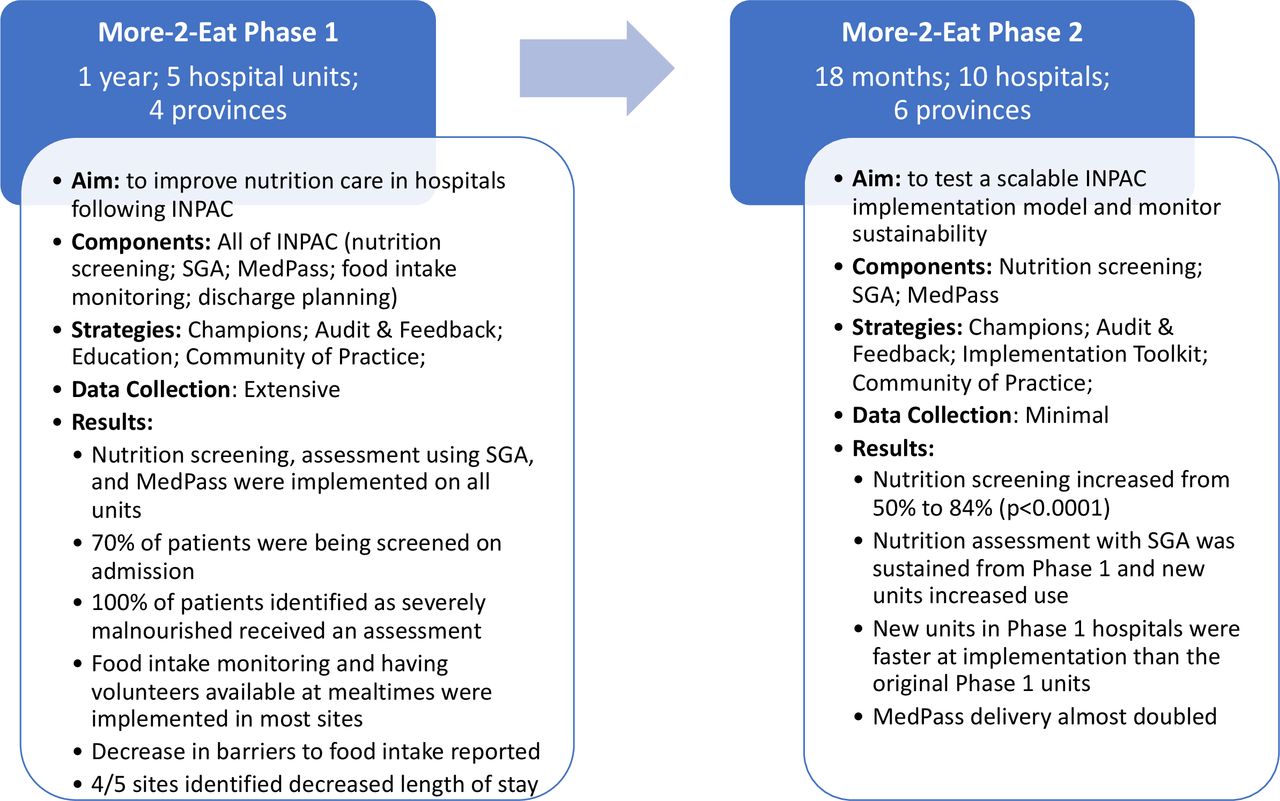
More-2-Eat (M2E) was a theoretically driven implementation study with two phases conducted between 2015 and 2019.27 Phase 1 (2015–2017) demonstrated how to implement the Integrated Nutrition Pathway for Acute Care (INPAC), an evidence and consensus-based pathway to prevent, detect and treat malnutrition in adult patients in hospital.5 28 Phase 2 (2018–2019) demonstrated that a scalable INPAC implementation model could increase uptake of nutrition risk screening, malnutrition assessment and other nutrition care activities in diverse acute care hospitals across Canada.29 In this scalable model, the implementation strategies included local or site champions who had received some training and mentorship in implementation processes and behaviour change techniques; an implementation toolkit based on phase 1 results30; a community of practice; and audit and feedback of relevant data collected through an INPAC audit.29 Quantitative results demonstrated that improvements in screening and assessment rates were sustained for at least 4 years in phase 1 sites, and screening was more readily implemented in new units and hospitals.29 Qualitative results demonstrated how these improvements were implemented, sustained and spread, as described below.31 32 The involvement of dedicated champions in M2E, some of whom were involved in both phases, provides a unique opportunity to deepen our understanding of how initiatives like INPAC can be sustained and spread. Overall results from M2E phase 1 and phase 2 are published elsewhere.29 31–37 Key aims, implementation strategies and results are summarised in figure 1. The objective of this substudy was twofold: (1) to understand the longer term role of champions in sustainability and spread of nutrition care improvements; (2) to determine if themes identified in phase 1 were still applicable or required expansion in phase 2.

Summary of the aims, components, implementation strategies and key results from More-2-Eat phase 1 and phase 2.8 29 53 INPAC, Integrated Nutrition Pathway for Acute Care; MedPass, delivery of oral nutritional supplements; SGA, subjective global assessment.
Methods
The M2E project: hospital recruitment in phase 1 and phase 2
In M2E phase 1, five diverse hospitals from four provinces in Canada were selected through a request for proposal process based on diversity in geography, type of medical patient (eg, stroke, geriatric, general medicine), use of nutrition risk screening tools and use of the SGA. Sites also had to demonstrate commitment from the organisation and core members of the unit team (director of care, lead nurse, physician, clinical nutrition manager, etc) as part of the proposal.38 Three of the five phase 1 hospitals had participated in the Nutrition Care in Canadian Hospitals study, which was a prevalence investigation focused on describing the issues of malnutrition, outcomes and care practices in hospitals.2 39 40
For phase 2, all phase 1 hospitals were invited to participate, and one declined as the champion had left the organisation. The remaining six hospitals were recruited through a request for proposal process held by the Canadian Malnutrition Task Force (CMTF), of which 18 hospitals applied. Selection criteria included: (a) lack of full implementation of screening with the Canadian Nutrition Screening Tool (CNST), SGA and/or MedPass, a model of delivery for oral nutritional supplements which has been shown to increase uptake41; (b) demonstrated capacity to lead implementation, and readiness to implement and sustain practices (eg, organisational support); and (c) diversity in hospitals (eg, regions in the same province, community hospital vs academic centre, size), and medical and surgical units/patients.29 In both phases, the hospital team selected the champions and the unit(s) for implementation.
The M2E project: aims of phase 1 and phase 2
The aim of M2E phase 1 was to see how much of the INPAC components could be implemented in a 12-month period, and how these were implemented. Implementation was led by a hospital-selected local champion and research associate who received training (described below), mentorship and data analytical support from researchers at the University of Waterloo. Sites tailored the order of introduction of INPAC components and how they implemented these care activities. In M2E phase 2, 10 hospitals had 18 months to focus on implementing three key elements of INPAC that phase 1 hospitals had found achievable in 1 year, and activities that drove other improved practices. In phase 2, all sites were required to implement nutrition risk screening using the CNST, nutrition assessment using the SGA and MedPass for delivery of oral nutritional supplements. Sites were also encouraged to focus on other aspects of INPAC, including food intake monitoring and discharge planning, once the three core activities were initiated.41
Implementation strategies: champions
In both phases of M2E, each hospital had a local champion that led an interdisciplinary site implementation team to plan and implement the best practice INPAC activities and worked towards integrating them into the unit routine. Champions were selected by the team submitting the recruitment proposal. These M2E champions were typically dietitians who held a manager/leadership position and was the main point of contact with the research team. Champion responsibilities included: completing ethics review; building the unit implementation team; supporting and empowering unit champions; training staff to complete INPAC audits; leading the unit implementation team to discuss how to implement the best practices; training team members on behaviour change techniques and practising their use; managing the implementation effort; creating or supporting creation of reports based on audits to reinforce best practices; and communicating with the research team and peers on their site’s implementation effort. Champion demographics are provided in table 1; all champions interviewed for this substudy were female and 10/14 held a managerial role.
Interview participant (champions) demographics and hospital details
Two-day, in-person training for M2E champions in phase 1 included an introduction to INPAC, change management, quality improvement and behaviour change, particularly Michie et al’s42 behaviour change wheel, recognising that Capability, Opportunity and Motivation was required to change team behaviour towards best practice.42 For phase 2, this training was conducted through three recorded webinars (1 hour each), including: (a) INPAC and the three targeted activities for implementation, (b) tips on behaviour change techniques learnt from phase 1, and (c) how to complete an INPAC audit.
Implementation strategies
At the end of phase 1, an INPAC implementation toolkit was created, focusing on ‘what’ to change to improve nutrition care, and ‘how’, including steps and resources (templates, examples, discussion group questions, etc) suggested by phase 1 sites. This toolkit was the starting point and guide for phase 2 sites. Audit and feedback, an implementation strategy with known effectiveness,43 was used in both phases, with process measures collected through an INPAC audit. In phase 1, INPAC audit data were analysed and returned as a monthly report generated by a postdoctoral researcher at the University of Waterloo. In phase 2, an automated process was set up so champions would enter their own INPAC audit data into a secure, web-based, data entry system (REDCap; Research Electronic Data Capture), download the data and then upload it to an Excel template which automatically generated reports with visual representations of the data. Both phases included a community of practice including champions and researchers, which mentored champions via monthly telephone calls and an email listserv for questions.
Overall, phase 1 was more intensive with extensive data collection, a research associate for each site and regular researcher involvement.27 Each phase 1 site received $C80 000 in research funds to support implementation and data collection. Phase 2 used a more scalable model with minimal researcher support, no research associate, and data collection only included bimonthly INPAC audits. Each phase 2 site received $C10 000 for completion of INPAC audits. Details of phase 2 sites are provided in the ‘Province’ section of table 1. Sites decided themselves how they chose to spend the money, with a few using the funds to provide protected time to support the champion, in addition to supporting data collection.
Phase 1 qualitative data: baseline
In October/November 2015, baseline interviews (n=40) and focus groups (n=11) were conducted with the five original sites during the 2-day site visits by CL before sites started INPAC implementation. A total of 133 participants were involved, including nurses, physicians, food service workers, dietitians and hospital management, among others. Five main themes were identified: building a reason to change; involving relevant people in the change process; embedding change into current practice; accounting for climate; and building strong relationships within the hospital team.31
Phase 1 qualitative data: post implementation
In 2016, after a year of INPAC implementation, CL completed another round of site visits to conduct interviews (n=45), small group discussions (4 groups; n=10) and focus groups (11 focus groups; n=71) (total n=126) with staff and management. A year after the end of phase 1 (early 2018), another round of telephone interviews (n=12) were conducted to understand if and how sites were, or were planning to sustain and spread INPAC initiatives to other units or hospitals.32 Strategies to sustain changes included: maintaining the new routine; building intrinsic motivation; continuing to collect and report data; and engaging new staff and management. Strategies to spread included: being responsive to opportunities; considering local context and readiness; and making it easy to spread. Strategies that supported both sustaining and spreading included: being and staying visible; and maintaining roles and supporting new champions.32
Phase 2 quantitative results
In phase 2, INPAC audit data from 5158 patient charts found that admission nutrition screening increased from 50% to 84% (p<0.0001).29 Screening practices were sustained on units involved in phase 1, meaning nutrition screening had been sustained for at least 4 years. The new units added from phase 1 sites (spread from phase 1) were faster at implementing nutrition screening than the new phase 2 sites. Nutrition assessment using SGA was also sustained at phase 1 hospitals including in new units in phase 1 sites. The new phase 2 units improved completion of SGA but did not reach the levels of phase 1 units (original or new). Delivery of oral nutritional supplements using MedPass almost doubled over the time periods (7%–13% of all patients, p<0.007).29
Phase 2 qualitative data collection
To further understand the role of the champion in sustaining and spreading the nutrition care improvements, 10 telephone interviews were conducted with all phase 2 champions between July and December 2019. All M2E champions were invited as they each provided their own valuable insight, both positive and negative. No champion refused to participate. Those involved since phase 1 were able to provide a long-term perspective. CL conducted all interviews, and since she had also conducted the previous three rounds of interviews in 2015, 2016 and 2018, she could go into depth about each site, and understood the context and challenges faced over the years. As CL had been working with the phase 1 champions for several years, she had a relationship with these champions which facilitated the depth of the conversation. CL had been on the monthly calls with new phase 2 champions but did not have a relationship with these champions. CL is a female, postdoctoral, implementation scientist and health services researcher. She is not a healthcare professional and not associated with any of the hospitals.
An active interviewing approach was used based on a semistructured interview guide (online supplemental file 1) adapted by CL for each hospital based on how long they had been involved with M2E.44 Focus of the interviews, particularly for champions involved for several years, was on sustainability of improvements and efforts to spread to other units and hospitals. Context notes were made immediately after each interview. Verbatim transcription of audio recordings was completed by a professional service. A draft publication was sent to all champions to review the results.
Supplemental material
Analysis
Two rounds of deductive analysis were conducted by CL using NVivo V.12 on transcript from the interviews with the champions. The first round of deductive coding focused on the role of the champions using the 3C model.26 Themes related to the role of champions not covered by the 3C’s were inductively coded. Results of this analysis were reviewed against the transcripts by RV, JB and HK (n=2 transcripts each), who also confirmed the similarity with phase 1 findings. This acknowledgement led to the second round of analysis which included deductive coding to the phase 1 baseline and post implementation themes (described above and elsewhere31 32). Ideas that did not align were coded inductively then reviewed by RV, JB and HK. Since this was the fourth round of interviews, saturation was thought to have occurred by interview 7; however, interviews were continued so perspectives of champions from all sites could be included. All hospitals had the opportunity to review results. To interpret the participant codes in the results, P1 represents a site involved since phase 1, and P2 for a site new in phase 2.
Results
Fourteen M2E champions were involved (10 interviews) from 10 hospitals in six provinces across Canada (table 1). Three hospitals, all new in phase 2, had more than one champion. All champions felt sustainability was the most challenging aspect of INPAC implementation, recognising that ‘you just can’t set it up and walk away. It needs regular attention by a leader’ (03-P1). The use of trained champions, typically dietitians in manager/leadership positions, was a crucial INPAC implementation and sustainability strategy. To fill this role, champions needed to understand the Concepts of change management, implementation, adaptation, sustainability and spread in order to embed the changes into routine practice. Champions also needed the Competence, including the skills to identify, support and empower new champions, thus decreasing the burden on individual champions. Even when the champion knew the concepts and had the competence, they still needed the Capacity, including time, resources and leadership support in order to stay engaged after initial implementation. Capacity appeared to be the most important and limiting facilitator for champions to stay engaged, thus the most challenging. The 3C’s in relation to trained M2E champions are summarised in figure 2.

{kind=link}
{kind=link}
Relationships among concept, capacity and competence regarding implementation of sustained nutrition care improvements (adapted from Laur et al [26]).
Results also suggest that the themes identified in phase 1 baseline and post implementation interviews31 32 were still relevant at least 4 years later, and thus help explain the quantitative phase 2 data, which showed sustained nutrition screening and assessment.29 Phase 2 champion interviews mapped to all phase 1 themes. Emphasis across some themes shifted over time and whether the effort was directed to spread or sustainability. Phase 2 champions emphasised the importance of audit and feedback, and the need for standardisation to support embedding the nutrition care improvements into current practice.
The 3C’s of champions
Concept
Champions did not need to be experts in change management, implementation, adaptation, sustainability or spread; however, they did need to be aware and understand the importance of these concepts to apply them, with mentors to guide them through the process. Understanding that implementation is more than education and reminders, and that sustainability and spread will not happen on their own, were central concepts for champions. ‘You can only remind and educate and do all those things so many times with the nursing, and then if there’s other barriers in place, then we need to try and find out why aren’t they being done’ (010-P2). Champions learnt about change management through trial and error and the need to always be flexible. ‘You’ve got to really work at being flexible, moulding it, changing as time goes on, and finding what the needs are from the unit level’ (03-P2). Champions also needed to truly listen to and involve those impacted by the change. ‘You definitely have to involve the staff, or you’d never get down to the right solutions’ (03-P2).
Champions also reported needing to understand that they could not keep adding new processes and had to recognise the importance of balance. This balance included refining an existing process or removing what was not having a beneficial impact to make room for another or different process that would allow that benefit, without increasing the time required for those involved.
When we look at something, as opposed to adding additional work or looking at increased workload, we try to achieve the same thing by doing things a bit differently, right? So, where can we save time? Then if you can highlight that with the staff and you’re saying that we’ve actually reduced your workload if we follow this process or if we can achieve this, then you’re going to have sort of less work in the long run or reduced length of stays, or you’ll have better outcomes. (002-P2)
MedPass was used as an example of this balance in one site, presenting the new process of MedPass as another form of administering medications, a process which the staff were doing anyways. The champion highlighted how the process would save time because they would no longer need to ‘chase after’ dietitians for approval nor complete a large assessment, which had been the previous process for administering oral nutritional supplements. Understanding the need for these concepts was directly connected to the competence to apply these concepts in practice.
Competence
Champions discussed needing the competence, or skills, to apply the implementation concepts or strategies, including supporting new champions, collecting relevant data, listening to and learning from others, and finding ways to make it easier for changes to be embedded. When encouraging sustainability and spread, a key competence was the ability to identify, support and empower others to become unit or topic-specific champions, thus decreasing the burden of implementation and spreading out ownership.
Pick a [unit] champion that has informal leadership qualities, so they’re respected by their peers, they’re engaged in the project, they want to see successes, and they’re passionate about something. … You have to really be choosy about who you pick – that they’re respected by their peers, and they’ll listen to them, and, again, they, themselves, are engaged. (02-P2)
Although champions discussed needing to be selective when picking other champions, this did not need to be discipline specific. For example, dietitians did not always need to be nutrition champions, and nurses or other professionals could champion this role and emphasise that nutrition care is everyone’s responsibility.
The competence to build and maintain relationships with staff and management was needed. One champion discussed overcoming the challenges of engaging hospital leadership. ‘I think that it [talking to leadership] can be intimidating, but it’s not really. They’re happy to hear what people are working on, and especially initiatives like this that are for patient-centred care’ (010-P2).
Some champions mentioned needing the competence to rapidly understand the context of new units, to know what is going on in the system and to know who to consult to determine the right time to make nutrition care improvements. These competencies could be learnt, with phase 1 champions refining their skills over time and providing guidance to the phase 2 champions. One phase 2 champion who was not in a leadership position discussed the competence she developed during INPAC implementation.
It made me see things a lot differently just in the way that the hospital works and how change works and big organizations. I’ve never been involved with a big project like that that’s kind of higher level than just dietitian work. … Sometimes, I wanted to quit because I was like, ‘How can I do this? I’m just a dietitian. No one cares what I’m doing,’ and those kind of things. But just knowing that anyone can do it… you don’t have to be a manager. You don’t have to be on the senior leadership. You don’t have to do anything crazy. You can make changes from all different levels, and it just sometimes might take you longer. You learn a lot along the way, but it can happen. (010-P2)
Capacity
Even when a champion understood the concepts and had the competence to make change, if they reported a lack of capacity to stay engaged after the initial implementation, it was more difficult to sustain and spread. Capacity was reported as an issue for all champions. Several of those involved in phase 1 found phase 2 to be more challenging as they had fewer resources, and less dedicated time for implementation, especially as they were spreading to at least two other units. However, this change also forced champions to increase their competence and find ways to be more efficient with time and resources. ‘To keep things going, I think I’m going to have to be more creative in trying to realize efficiencies. … We might have to be a little bit more selective with what we choose and how much time we actually have to dedicate to it’ (09-P1).
One champion discussed the capacity challenges of being an M2E champion in a hospital leadership position in a healthcare system that was undergoing significant restructuring. ‘It’s been challenging from a resourcing perspective. I feel like I’m being torn at all sides, and so it’s been a bit of a struggle to coordinate more time with the teams to try and keep this work going’ (06-P1).
Concepts, competence and capacity were key for champions to sustain and spread nutrition care improvements.
It wasn’t a ‘stick it in place and let it thrive.’ You’ve got to really work at being flexible, moulding it, changing as time goes on, and finding what the needs are from the unit level. … Each unit wants something a little bit different. It takes time and, really, consultation with those involved to figure out what’s going to work at those sites and revisiting. (03-P1)
Comparison to phase 1 themes
Baseline
Phase 2 participants mentioned the five themes identified at baseline that were focused on how to effect meaningful improvements and implement INPAC. These themes were: building a reason to change; involving relevant people in the change process; embedding change into current practice; accounting for climate; and building strong relationships within the hospital team.31 At the core, new phase 2 sites still needed a reason to change nutrition care practices and a reason to keep those practices going, thus impacting both spread and sustainability. ‘It goes a long way with nursing to get them to do anything if you give them a reason why – a good reason why’ (02-P2). The relevant people needed to be involved and be supported to stay involved. Leadership support was important, as was having continued support from a unit champion who could increase visibility and demonstrate that reason to change. Champions recognised the long-term impact of this interdisciplinary involvement and demonstrated ways they planned to support unit champions to stay engaged.
Involve as much of the folks on the unit as much as possible and engage and to see where they have opportunities to kind of take some leadership on some of these issues because they will still be there … we know that those will be great champions going forward, but just kind of helping support and grow that a little bit more before the study ends so that hopefully they will have a supportive team that they can be able to move forward with and keep some of those changes and continue on to make the changes well beyond the end of the study is our hope. (07-P2)
Embedding change was mentioned at baseline and key for sustainability of nutrition care practices and change processes, yet ways to action this differed between implementation and sustainability phases. For example, in phase 1, M2E-specific teams were set up to support the ‘project’, while in phase 2, discussions and planning for INPAC implementation and sustainment were incorporated into existing quality improvement teams. This switch encouraged sustainability and meant the changes were considered within the context of other changes underway, and the work was seen as part of regular practice rather than a time-bound ‘project’. The sites new to phase 2 (spread) started with these embedded, rather than project-specific teams. ‘The dietitians really use opportunities like the huddles and their quality council to kind of integrate the information versus having special meetings on the side for this particular project. It’s too hard’ (06-P1). In phase 1, champions focused on understanding and adapting to a specific unit, and by phase 2, the champions were more focused on supporting spread, for example, through standardising local procedures, understanding what could be adapted to the local context and what needed to be maintained to be consistent across the hospital. ‘When you set a standard on a unit, you can’t go and have a different standard on another unit. … I think the key thing is the communication piece – setting the standard, having it written down, making sure all of the key players know about it’ (01-P1). Phase 2 interviews also mentioned national standards as facilitators for embedding change, which were not mentioned in phase 1. ‘It’s so much easier to work with when you’re able to say, “This is best practice. This is the standard. This is what we’re trying to achieve”’ (10-P2).
Accounting for climate, or hospital values, was not mentioned as frequently in phase 2 as baseline; however, this may be because the phase 2 champions were mostly hospital managers/leaders and their involvement demonstrated that the values of the hospital aligned with the study aims. Champions did acknowledge the need to recognise the climate or values of specific units, which aligns with the theme of accounting for local context and readiness in both spread and sustainability. The importance of strong relationships was evident in baseline and post implementation themes and was still important in phase 2. In phase 1, the emphasis was on raising awareness about the need and the plans, while by phase 2, the emphasis was on maintaining relationships with other leaders and making the effort to introduce themselves and INPAC to new staff and building lasting relationships out of this common purpose. Overall, few differences were found between baseline phase 1 and phase 2 interviews; however, when separated into spread and sustainability, themes from phase 1 were particularly relevant for spread since champions were starting again from the beginning with building the reason to change and involving relevant people on the new units. For sustainability, the similarities were on building relationships, and continuing to adapt to changing context.
Post implementation comparison
Post implementation themes from the end of phase 1 suggested two key strategies to sustain and spread effective nutrition care practices: being and staying visible; and maintaining roles and supporting new champions.32 In phase 2, being visible, such as by being present on the unit, sending reminders and developing relationships with relevant people were all key factors to sustain and spread changes in all sites. ‘It was just trying to be more visible and talking with individual nurses about the aspects of INPAC that they were involved in. … putting up some more posters and kind of keeping the momentum going’ (03-P1). Maintaining the roles of current champions was key; however, this was limited by capacity as discussed with the 3C’s. Supporting new champions was facilitated by champion competence to identify, support and empower new champions, particularly when spreading to a new unit or hospital.
Sustainability
To sustain changes, themes from phase 1 included: maintaining the new routine; building intrinsic motivation; continuing to collect and report data; and engaging new staff and management.32 Although these themes were mainly relevant for sustainability, they also played a role in spread. Continuing to collect and report data, also called audit and feedback, was mentioned by all champions, and was more strongly represented in spread and sustainability in phase 2 interviews. Sites that were starting a new change (spread) used data to determine baseline rates and understand if there was a problem. When champions did not have the same capacity as in phase 1, they relied more heavily on the audits to know how each unit was progressing and to encourage sustainability. Audits of previously implemented activities were used for accountability, motivation and to encourage sustainability as action could be taken if rates had decreased. ‘Sharing results with them [unit staff] I think is important, and then circling back if we notice that there’s been a decline or we’re not getting the results that we need – you know, circling back with the staff to look at why, what is happening’ (02-P2). As collecting INPAC audit data was an M2E study requirement, some champions were concerned with their capacity to collect regular audit data long term, but planned to conduct an occasional audit to show progress (sustainability). Champions saw the benefits of frequent audits when starting at a new unit or hospital (spread). Other champions had found ways to integrate INPAC processes into existing data collection systems, decreasing the burden for data collection and increasing access to information, thus facilitating both spread and sustainability.
We’ve gotten IT to build us what’s called a status board … it probably takes less than a minute to just quickly scroll through and see everyone on your unit and quickly flag anyone who requires a screen or anyone who’s scored an SGA B or C that needs further intervention. (10-P2)
Results for maintaining the new routine suggested similar strategies to embedding into routine practice, with examples such as reinforcement through reminders and education updates. Intrinsic motivation connected to building a reason to change (spread) and maintain change (sustainability), and although capacity was always a barrier, as said by one champion, ‘If you care about it, you can make it work’ (10-P2). In one site, use of MedPass was not sustained and the champion felt there may have been a lack of intrinsic motivation to continue.
I don’t know if it’s the lack of trust or she [unit champion; dietitian] truly believes that people don’t need it, which is kind of interesting. … I don’t get the sense it’s a barrier to getting it done. It’s really her decisions around who gets it and who doesn’t. (06-P1)
Staff and management turnover was high in most hospitals, impacting spread and sustainability. Ways to engage new staff and management mainly included integrating into existing education and orientation sessions and involving the nurse educator. Engaging new management was more challenging in phase 2 than phase 1, with champions having less capacity, mainly time, to quickly engage new management when turnover was high. ‘[A] great new manager came onboard… they knew nothing about – or very little about – what we were doing and were in theory supportive, but it just took a long time to really get them up to speed and helping to facilitate keeping things going’ (03-P1).
Spread
Themes for spread identified in phase 1 included: being responsive to opportunities; considering local context and readiness; and making it easy to spread.32 Each of these factors was mentioned in phase 2 interviews and has some overlap with sustainability. In phase 2, champions became more specific about how to respond to opportunities and the importance of starting back with initial implementation, adapting to the new unit/hospital, based on their inner and outer contexts, including readiness to make change. Champions involved from phase 1 typically felt they were starting from a better place with new units based on their previous experience. ‘We’re not starting from scratch. We had already rolled out those initiatives in the other departments and on the other units, but then as problems arise, we’re working with those established, unit-based teams to talk about how we could do things differently or make them better’ (03-P1). Champions new in phase 2 also felt they were starting from a good place since they had access to existing resources and could connect with phase 1 champions to ask questions and learn from their experience. Further, they had the example of hospitals in phase 1 that were able to successfully implement INPAC activities.
Even with this strong foundation, some champions, particularly those involved since phase 1, were surprised by how different new units were, emphasising the importance of considering local context and readiness.
Every unit is extremely different. Even though they’re using the same forms and following similar processes, it’s been challenging just to learn how things are done differently on those units, but it’s been nice to work with three different hospitals. Although it takes a lot more energy and time to travel and be more involved at those sites, it’s been good to go a little bit abroad and involve more staff that way. (03-P1)
With fewer resources and many hospitals undergoing extensive changes, such as a new Electronic Medical Record (EMR) or provincial restructuring, sites had to be more responsive to ‘windows of opportunity’ in phase 2 and decrease their expectations of how much could be achieved in 1 year.
[We had to] pick the windows of time that were given to us, and kind of run with it. … [As long as] there was an opportunity to change, then there was an opportunity to make improvement. And the outcome may not look like we had hoped for or planned, but that we were more prepared to accept that if we had a small success, that was okay, and then we were just going to keep building on that. (09-P1)
Discussion
The quantitative M2E results29 demonstrated that changes made in the phase 1 hospitals were sustained 4 years later (end of phase 2) and were spread to other hospitals. This substudy helps explain the role of the M2E champions in supporting sustainability and spread of nutrition care improvements in hospital. This understanding of the role of champions in supporting implementation, spread and sustainability of nutrition care improvements can support other hospitals to use a similar approach.
Strategies for implementation, sustainability and spread were relatively similar from phase 1 to phase 2, with increased emphasis on audit and feedback and the need for standardisation to support embedding the nutrition care improvements into current practice. Strategies focused on spread related strongly to the baseline themes, as the emphasis was on starting again from initial implementation, yet the champions felt more prepared as they adapted to the new context. Interestingly, both phase 1 and 2 champions felt more prepared for initial implementation/spread, as those from phase 1 now had more experience, and those new in phase 2 knew change was possible and felt supported by the phase 1 champions. As mentioned in other studies, the champion’s role for sustainability was more focused on continuing to monitor and adapt based on changes in the unit and hospital.20
To facilitate the improvements, trained champions understood the Concepts of change management, implementation, adaptation, sustainability and spread, to embed the changes into routine practice. Champions also had Competence, including the skills to identify, support and empower new champions, collect relevant data, listen to and learn from others, and find ways to make it easier for changes to be embedded. Capacity, including time, resources and leadership support, appeared to be the most important facilitator for champions to stay engaged, yet also was the most challenging. Although the 3C model has not been applied in other studies, it appears to be a useful way to consider the champion role and where gaps may be if intervention implementation is lagging. The 3C model follows a similar approach to the Promoting Action on Research Implementation in Health Services framework which provides a way to implement research into practice focused on evidence, context and facilitation.45
M2E champions were typically dietitians with leadership or managerial responsibility, and worked closely with interdisciplinary site implementation teams, which included front-line staff. This interdisciplinary approach aligns with the CFIR, which emphasises the importance of champions at different levels of the organisation, including front-line and supervisor or manager champions.16 Literature highlights that champion roles in the past were typically emergent, such that a clear champion ‘emerged’ based on their strong support for a cause.46 More recently, champions are being assigned to this role and it is unclear if this emergent versus assigned method of champion allocation makes a difference.46 As M2E champions were named as part of the initial proposal, it is unclear if they were appointed or emergent; however, based on experience working with these champions, it appears to be a mix with the proposal leads working together to choose an appropriate champion.
A 2018 review found champions to be an important positive influence on implementation effectiveness.18 This review identified characteristics of champions which also aligned with the competencies discussed by M2E champions, specifically: to fully understand the initiative and local context; collaborating well with others; leading teams and recruiting new team members; and collecting data, tracking progress and providing feedback.18 Characteristics identified in this review, which were not highlighted as frequently by M2E champions, were around negotiation and having political acumen.
The importance of champions is also recognised with respect to their role in having sustained commitment to implementation activities, requiring engagement, influence, credibility and capacity to champion the initiative.47 Some studies have allocated a ‘sustainability champion’, who, among other roles, ‘made a commitment to sustain best practices education with future employees’ after the funding ended.48 Within M2E phase 1 and phase 2, sustainability of champions was encouraged by providing training and mentorship from researchers to develop their competence, while also encouraging them to empower others to become champions in their hospitals. This empowerment helped the trained champions to bring others on board and share the responsibility. It is unknown if champions continued to bring new people on board after M2E phase 2 funding ended. During phase 2, phase 1 champions became mentors for new sites; however, it is unclear if their mentorship continued after the regular mentoring calls stopped at the end of phase 2.
Changing the emphasis
It is not surprising that champions felt more strongly about the use of audit and feedback in phase 2 for sustainability and spread. With less capacity, champions relied on occasional audits to keep them informed of their progress and to direct where to focus next. Audit and feedback is a common implementation strategy with proven effectiveness,43 although few studies have focused on sustainability.
The increased focus on standardisation in phase 2 was also expected as champions aimed to build on their previous work and, ideally, make it easier to implement in the next unit or hospital by having more standardised processes. However, champions experienced the common tension between needing to adapt to the new context, while also maintaining fidelity to the effective strategies.49 M2E champions’ experience appears to align with the view that fidelity and adaptation should be complementary, all aiming for the ‘end product’ of value for patients, providers, organisations and systems.49 Knowing when and how to adapt an intervention is not straightforward.50 M2E champions applied and understood the concept of adaptation and had the competence to navigate complex unit and hospital systems. While champions adapted their ways of working with new units or hospitals, their focus on implementing and sustaining nutrition screening and assessment remained consistent.
Scaling nutrition care improvements
While M2E focused on how to implement nutrition care improvements at the unit and hospital levels, efforts were also underway to ‘scale’ nutrition care improvements at a national level. While spread is focused on going from one site to another with potential for significant adaptation to the local context, scale is more focused on addressing the wider infrastructure.15 51 Efforts to scale nutrition care improvements were led by the CMTF within the Canadian Nutrition Society (CNS) by working with Health Standards Organization to develop a national standard of Canada, entitled: ‘CAN/HSO 5066:2021 Malnutrition Prevention, Detection and Treatment ’ (in press).52 Hospitals can strive to meet this Standard using a multimodal and multidisciplinary approach that involves organisation-wide leadership to support, facilitate and implement changes in nutrition care processes to prevent, detect and treat malnutrition in adult and paediatric patients and after discharge into the community. The Standard aims is to help hospitals identify and treat malnutrition sooner and thus improve patient outcomes.
The momentum generated by the M2E studies, the CMTF and the CNS over several years has raised the profile of hospital malnutrition in Canada. This impact was demonstrated when recruiting for phase 2 hospitals, as it was difficult to find hospitals that had not started nutrition screening or other recommendations which sites directly connected to INPAC. Having a national Standard will, ideally, help maintain the focus on the importance of nutrition care in hospitals at the local, national and, potentially, international levels.
Strengths and limitations
As M2E has been running for several years, a key strength of this work is the ability to look qualitatively and quantitatively at the changes in nutrition care practice over time in 10 hospitals across Canada. As several implementation strategies were used simultaneously, the full impact of the champions cannot be confirmed; however, many of the other strategies, such as audit and feedback, and training, were implemented or received by the champions, indicating these strategies likely would not be in place without the champion. As the same researcher conducted all interviews in phase 1 and phase 2, she had developed a relationship with the champions, particularly from phase 1, thus was able to increase the depth of understanding within each interview by building off specific examples and experiences. Using the same interviewer may have limited the generation of new ideas; however, several checks with other authors and M2E champions were in place to ensure results were confirmed from a variety of perspectives. Triangulation of results was also conducted with the quantitative data, which demonstrated that the changes were sustained, and successful implementation was not based on champion interpretation. There are also limitations with the quantitative audit data as there may have been inconsistencies in reporting. Within the Concept domain, it should be noted that champions did not necessarily use the same words to demonstrate their understanding of the concepts. For example, the term ‘adaptation’ was not necessarily used by champions, yet champions understood the need to change their approach to meet the needs of the changing contexts.
Conclusion
The M2E study has demonstrated that nutrition care improvements can be implemented in a way that can be sustained for a minimum of 4 years and be spread to other hospitals. By focusing on core elements of INPAC, trained champions at 10 hospitals across Canada were able to advocate for and implement changes that improved nutrition care for patients. These changes were achieved because champions understood the concepts of change management, implementation, adaption, sustainability and spread, as well as had the competence and capacity to bring this work forward. Champions are an important implementation strategy and understanding how to identify and support them can increase impact and improve patient care.
Data availability statement
Data sharing not applicable as no data sets generated and/or analysed for this study. As transcripts may be identifiable, interviews are not available.
Ethics statements
Patient consent for publication
Ethics approval
Research ethics boards at each hospital (and hospital-affiliated university, if needed) and hospital administration approved the study, as did the research centre, the University of Waterloo (ORE 31791). M2E phase 1 was retrospectively registered to ClinicalTrials.gov on 7 June 2016 and prospectively for phase 2 on 1 January 2018. All data remained anonymous to all researchers, excluding CL. As HK, RV and JB had in-depth knowledge of the sites, participants were informed that transcripts may have been identifiable to these three authors. Written consent was taken before each interview, complemented with a verbal reminder before recording began. Participants were aware that some quotations would be used and that these would be deidentified by person and hospital before use.
Acknowledgments
The 10 hospital sites, their management and staff were essential to the conduct of the study. Auditors at each site are thanked for the dedication to a quality data collection. Champions are specifically acknowledged as partners in this research, which would not have been possible without their dedication: Susan Taylor, Tina Strickland, Sonya Boudreau, Nancy Tawil of Victoria General Hospital, Halifax, Nova Scotia; Dianne Gaffney, Amanda Degen McLarty, Rebecca Donnelly, London Health Sciences Centre, London, Ontario; Kirsten Bernosky, Erin Woodbeck, Thunder Bay Regional Health Sciences Centre, Thunder Bay, Ontario; Amy Noto, Melanie Hart, Brandon Regional Health Centre, Prairie Mountain Health, Brandon, Manitoba; Lisa Koski, Michelle Smith, Kelowna General Hospital, Kelowna, British Columbia; Meghan Reddy, Jennifer Masson, Jennifer Beverly, Jenna Shepherd, Lennox and Addington County General Hospital, Napanee, Ontario; Marilee Stickles-White, Lina Vescio, Andrea Digweed, Tawnya Crawford, Liz Kukan, Niagara Health System, Niagara Falls, Ontario; Donna Butterworth, Chelsa Marcell and Stephanie Barnes, Concordia Hospital, Winnipeg, Manitoba; Roseann Nasser, Pasqua Hospital, Saskatchewan Health Authority, Regina, Saskatchewan; Mei Tom, Michelle Booth, Francesca Richard, Nicole Tanner, Chelsea Greschner, Shannon Rendall, Alberta Health Services, Edmonton, Alberta.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Celia_Laur, @ProfSumantraRay @nnedpro, @nutriagelab
Contributors All authors (HK, CL, RV, JB, SR) reviewed and verified the final manuscript for submission. All authors were involved in conception and design. CL conducted the interviews, analysis and interpretation, which were verified by HK, RV and JB. The final version was verified and approved by each hospital.
Funding This research was funded by the Canadian Frailty Network (CFN) (Phase 1 SIG 2014F-08; Phase 2 KT2017-01), which is supported by the Government of Canada through the Networks for Excellence (NCE) programme. As required by CFN, funding from sponsors was also solicited for this knowledge translation grant. This included in-kind hospital investment of staff time for implementation efforts as well as monetary sponsorship from Abbott Laboratories. For Phase 1, CL was funded by a Canadian Institutes for Health Research (CIHR) doctoral award (201510GSD). While conducting the Phase 2 interviews, CL was funded by the CIHR Health System Impact Fellowship (Postdoctoral; IHSPR-FE).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.