Article Text

Abstract
Background Adherence to nutritional guidelines for chronic disease prevention and management remains a challenge in clinical practice. Innovative strategies are needed to help optimise dietary behaviour change.
Objective The objective of this study was to determine if a nutrigenomics-guided lifestyle intervention programme could be used to motivate greater dietary adherence and change in dietary intake short-term, moderate-term and long-term compared to the gold-standard population-based weight management intervention (Group Lifestyle Balance (GLB)/Diabetes Prevention Programme (DPP)).
Design The Nutrigenomics, Overweight/Obesity, and Weight Management (NOW) randomised controlled trial is a pragmatic, parallel-group, superiority clinical trial (n=140), which was conducted at the East Elgin Family Health Team (EEFHT). GLB weight management groups were prerandomised 1:1 to receive either the standard GLB programme or a modified GLB+nutrigenomics (GLB+NGx) programme. Three 24-hour recalls were collected at baseline, 3, 6 and 12 months using the validated multiple pass method. Research assistants collecting the three 24-hour recalls were blinded to the participants’ group assignments. Statistical analyses included split plot analyses of variance (ANOVAs), two-way ANOVAs, binary logistic regression, χ2 and Fisher’s exact tests. Using the Theory of Planned Behaviour as guidance, key confounding factors of behaviour change were considered in the analyses. This study was registered with clinicaltrials.gov (NCT03015012).
Results Only the GLB+NGx group significantly reduced their total fat intake from baseline to 12-month follow-up (from 36.0%±4.8% kcal to 30.2%±8.7% kcal, p=0.02). Long-term dietary adherence to total fat and saturated fat guidelines was also significantly (p<0.05) greater in the GLB+NGx group compared to the standard GLB group.
Conclusions Weight management interventions guided by nutrigenomics can motivate long-term improvements in dietary fat intake above and beyond gold-standard population-based interventions.
- precision nutrition
- nutrition assessment
- weight management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about the subject?
It is challenging to achieve long-term dietary change and adherence to dietary guidelines; typically, nutrition interventions result in short-term dietary change, but these changes are not sustained long-term.
What are the new findings?
The addition of an actionable nutrigenomics intervention to the Group Lifestyle Balance programme enhanced dietary change and adherence to dietary guidelines long-term (12 months).
How might these results change the focus of research or clinical practice?
The provision of genetically-tailored nutrition advice can be used in research and clinical practice to motivate greater long-term dietary change and adherence to dietary guidelines.
Introduction
The science of nutrigenomics, which explores interactions between individual genetic variation, dietary intake and changes in gene expression, structure and function,1 has garnered significant attention in recent years with consumers and healthcare professionals alike expressing overall positive attitudes towards genetic testing for personalised nutrition.2–4 As such, a number of companies are offering nutrigenetic testing for weight management.5 6
A recent review reported that personalised nutrition recommendations are of great potential for optimising outcomes of weight management interventions, while also noting that research in this area is lacking and human intervention studies are needed.6 The potential value of personalised nutrition for weight management stems from studies indicating positive consumer attitudes towards genetic-based dietary advice,3 7 several indications that a one-size-fits all approach to weight management is not optimal,6 and the potential for genetically guided, actionable nutrition recommendations to help motivate changes in dietary intake.8
According to the most recent systematic review on genetic testing behaviour change research, nutrition was found to be the most promising lifestyle component that could be motivated as a result of undergoing genetic testing, especially when the genetic intervention provided actionable recommendations.8 Furthermore, this review found that genetic testing behaviour change research has yet to incorporate the Theory of Planned Behaviour (TPB), and incorporation of behaviour change theory in general is fundamentally lacking.8 This is concerning given that the TPB is one of the most widely accepted behaviour change theories. It suggests that attitudes, subjective norms and behavioural control are the three key factors affecting human behaviour.9 Furthermore, researchers in the field of genetic testing behaviour change research have called to action academia to incorporate this theory into genetic testing behaviour change studies in order to account for potential confounding factors; this has been further detailed elsewhere.10 Behaviour change theories provide important guidance for the development of interventions that are more likely to facilitate changes in lifestyle habits. Thus, failing to consider established behaviour change theories can lead to findings that do not demonstrate changes in dietary behaviours. As such, it is not surprising that the current limited knowledge related to change in dietary intake and eating habits in genetic-based weight management interventions does not appear to be promising.11 12 Overall, the field of nutrigenomics and behaviour change is highly complex and warrants further investigation.
This study aimed to address the limitations of previous work by considering the TPB in the dietary interventions and statistical analyses, and providing a high-quality, personalised, genetic-based lifestyle intervention. Ultimately, the purpose of this study was to determine if the provision of a nutrigenetic-based weight management intervention motivates greater dietary change and adherence compared to a population-based weight management intervention.
Subjects and methods
The Nutrigenomics, Overweight/Obesity and Weight Management (NOW) trial is a pragmatic, parallel-group, superiority, randomised controlled trial (RCT) (n=140) incorporated into the Group Lifestyle Balance (GLB) programme (formerly referred to as the Diabetes Prevention Programme). The GLB programme is one of the most effective public health weight management programmes13–16; this group-based health programme is offered to patients in numerous clinics in the USA and Canada and has been extensively researched for long-term weight management and diabetes prevention.13–16 Detailed study methods for the NOW trial have been published elsewhere.17 One author (JH) conducted 1:1 computer-generated cohort randomisation18 of GLB groups. A cohort randomisation model was used rather than subject randomisation to ensure that all participants in each GLB group received the same intervention (standard GLB or GLB+nutrigenomics (GLB+NGx)).
Participants
Patients were recruited into the GLB programme at the East Elgin Family Health Team (EEFHT) in Aylmer, Ontario, Canada, through healthcare professional referrals and word-of-mouth referrals from members of the community from April 2017 to September 2018. Patients expressing interest in the GLB programme were then invited to participate in the study if they met the following inclusion criteria: body mass index (BMI) ≥25.0 kg/m2, ≥18 years of age, English-speaking, willing to undergo genetic testing, having access to the internet and not seeing another healthcare provider for weight loss advice outside of the study. Pregnancy and lactation were exclusion criteria. Four of the five researchers (JG, JS, CO and JM) and all research assistants collecting 24-hour recalls were blinded to participant group allocation. It was not possible to blind the researcher responsible for organising and facilitating all intervention sessions (JH), and given the nature of the intervention, it was inappropriate to blind participants to their allocated intervention. The participants, setting and healthcare provider facilitating the interventions (JH) were all highly representative of typical/standard care, which speaks to the pragmatic nature of this trial. All interventions were delivered by one healthcare provider (JH) in order to standardise their delivery and enhance reliability, and no additional resources were required to implement the interventions; the healthcare provider was a registered dietitian (RD) with previous training in nutritional genomics.
Interventions
Staggered cohorts participated in the 12-month intervention (standard GLB or GLB+NGx) and data collection occurred from May 2017 to September 2019. Participants received specific targets for eight nutrients: calories, protein, saturated fatty acids (SFAs), monounsaturated fatty acids, polyunsaturated fatty acids, total unsaturated fat, total fat and sodium. These nutrients were selected based on weight-related information and advice available through current consumer nutrigenetic testing. The nutrient targets were derived from genetics for half of the participants and were derived from population-based guidelines19 for the other half of participants; the nutrition reports provided to participants have been previously published.17 For the standard GLB intervention, participants were advised primarily to follow a calorie-controlled, moderately low fat (25% kcal) nutrition plan.20 Both intervention groups followed the standard GLB programme’s overall calorie intake targets.20 For the personalised GLB+NGx group, individuals received information related to resting metabolism and subsequent personalised calorie deficits recommended for weight loss. Participants in the GLB+NGx group were advised to focus on the macronutrient recommendation(s) that was/were highlighted in their genetic report to enhance weight loss response. For example, an individual with the AA variant of FTO (rs9939609) was advised to focus on following a higher-protein nutrition plan to optimise weight loss, whereas an individual with the CC variant of APOA2 (rs5082) was advised to focus on following a low saturated fat (<10% kcal) nutrition plan to optimise weight loss (rather than all participants following the standard moderately low total fat GLB nutrition intervention). Participants randomised to the GLB+NGx group were also informed of their genetic predisposition to eat more frequently during the day based on MC4R (rs17782313) genetic variation. If an individual had multiple genetic variants and genetic-based nutrition recommendations highlighted in their genetic report, they were advised to focus on achieving one of the nutrition targets (of their choosing), and then work on another when they perceived that they were ready to engage in further dietary changes. A sample NOW trial genetic report has been previously published elsewhere17; this report was selected for the present study based on commercially available nutrigenetic testing accessible by the general public globally through healthcare professionals.
All participants were advised to track their food and beverage intake closely (by completing food records/journals) for the first 2–3 months of the intervention while working towards their nutrition targets. Participants were further advised to measure their food and beverage intake for at least the first week of the intervention in order to increase awareness and accuracy of the portion sizes indicated in their dietary tracking. In the second week of the intervention, participants were educated on counting and tracking calories and nutrients (total fat for the standard GLB group; individualised nutrients for the GLB+NGx group). This tracking was included in the intervention for educational purposes for the participants in order to help participants understand food/beverage sources of different nutrients and whether they were meeting their target(s). These food records/journals were not used for data collection or analyses; they were for educational purposes only. With weekly meetings for the first 3 months and meetings approximately once per month for the remainder of the 12-month intervention, participants had several opportunities to ask questions about their nutrition recommendations to ensure comprehension. These recommendations were also reviewed at a 3-month, 6-month and 12-month one-on-one follow-up appointment with an RD.
Incorporation of the TPB
This is the first study to intentionally incorporate the TPB into a genetic testing behaviour change study. Both interventions aimed to positively impact key components of the TPB (attitudes, subjective norms and behavioural control). The interventions aimed to impact attitudes by informing individuals of the health benefits associated with engaging in a healthy lifestyle and providing education on positive mindsets and mindfulness.20 The group-based nature of the intervention aimed to affect subjective norms. A stepwise, goal-setting approach was used to help positively impact behavioural control. In the GLB+NGx group, the intervention aimed to further impact attitudes through the provision of more personalised dietary guidance. All participants completed a baseline TPB questionnaire. The TPB was used to guide the analyses of possible attrition bias and subsequently control for possible confounding factors of behaviour change as further indicated below.
Genotyping
Oragene ON-500 saliva collection kits (DNA Genotek, Ottawa, Ontario, Canada) were used to collect DNA saliva samples of participants at the EEFHT. The saliva samples were shipped and stored at −80°C at the University of Toronto until they were analysed. The iPLEX Gold assay with mass spectrometry-based detection on the Sequenom MassARRAY platform was used for all genotyping. This genotyping method has been used in previous research.21–23 The following single nucleotide polymorphisms of interest to the current dietary change and adherence study were analysed: UCP1 (rs1800592), FTO (rs9939609), TCF7L2 (rs7903146), APOA2 (rs5082), PPARγ2 (rs1801282), and MC4R (rs17782313).
Dietary intake and adherence: data collection
Change in dietary intake was a predetermined secondary outcome of the NOW trial24 and was measured using the validated multiple pass method25 to collect three 24-hour recalls consisting of 1 weekend day and 2 weekdays. Data collection occurred at baseline (during a 14-day run-in period), 3-month, 6-month and 12-month follow-up in order to assess short-term, moderate-term and long-term changes. Trained research assistants who were blinded to participants’ group allocations collected three 24-hour recalls over the phone. In some rare cases where a participant could not be reached over the phone, the three 24-hour recalls were collected in-person at the EEFHT. Dietary adherence was measured by analysing the quantity of participants adhering to the calorie, saturated fat, total fat and protein recommendations. ESHA Food Processor V.11.3.285 (ESHA Research, Salem, Oregon, USA) was used for nutritional analyses.
Statistical analyses
The mean and SD were used to report continuous variables and percentages were used for categorical variables. Estimates of the different sources of attrition bias were conducted using two-way analysis of variance (ANOVA) models. The TPB9 was used to guide this analysis with data collected from a baseline TPB survey. The following possible confounding factors were analysed to determine if there were significant differences between dropouts in each group: attitudes towards changing their intake of calories, fat and protein (attitudes); friends eating a healthy diet, family eating a healthy diet (subjective norms); stage of change/transtheoretical model; perceived difficulty altering calorie, fat and protein intake (perceived behavioural control); income and education (actual behavioural control/social determinants of health).
χ2 tests were used to analyse categorical variables (dietary adherence). In cases where there were fewer than five expected counts, Fisher’s exact tests were used. To assess dietary adherence at 3 months while controlling for income, binary logistic regression was conducted. Split-plot ANOVAs were used to compare differences between groups (GLB vs GLB+NGx) for change in dietary intake from baseline to 3-month, 6-month and 12-month follow-up (prespecified outcome). Repeated-measures ANOVAs were used to assess within-group changes in dietary intake from baseline to 3-month, 6-month and 12-month follow-up (prespecified outcome). SPSS V.26.0 (IBM Corporation) was used for all statistical analyses, which took place in October–November 2019. The analyses were by originally assigned groups.
Hypotheses
It was hypothesised that the GLB+NGx group would engage in greater dietary changes and better adhere to the dietary advice compared to the standard GLB group.
Results
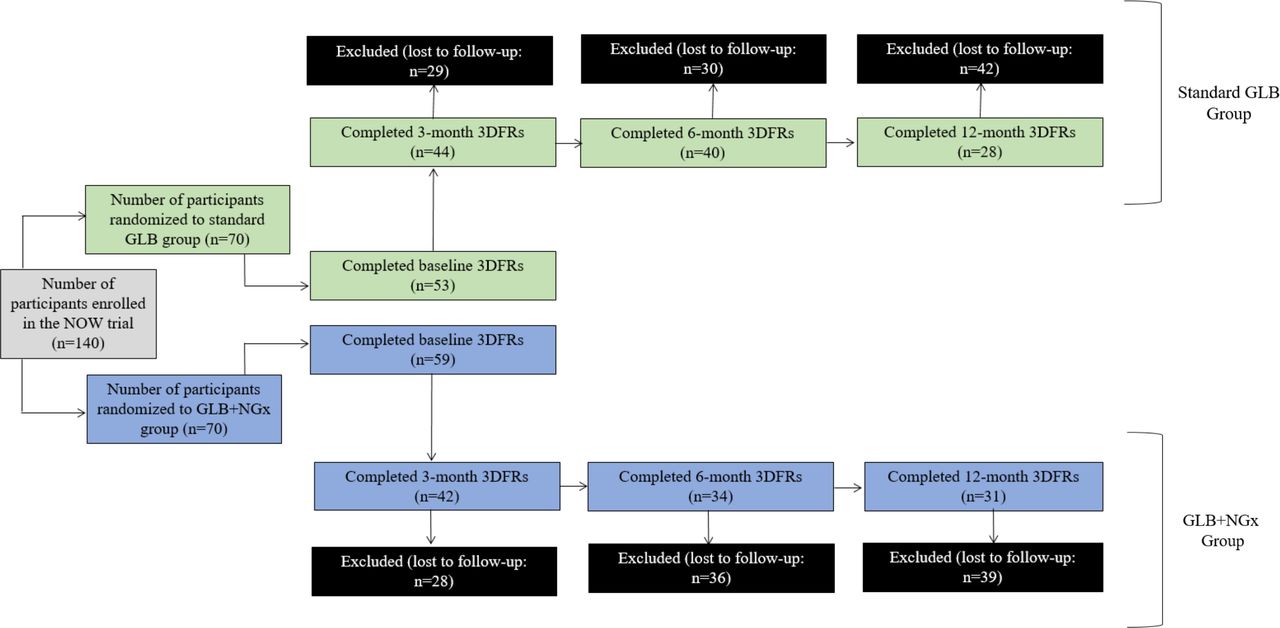
Overall, mean values from demographic and TPB characteristics (tables 1 and 2) indicated that the study population consisted of highly motivated, college-educated, middle-aged female subjects with obesity, who had positive attitudes towards changing their dietary intake, with neutral subjective norms related to friends/family consuming a healthy diet and neutral perceived behavioural control for changing their dietary intake. The genetic results of participants in the GLB+NGx group are summarised in table 3. There was significant attrition bias for one TPB component, income (p=0.02), at the 3-month follow-up only (table 2), and therefore, this was controlled for as a confounding factor in the 3-month analyses. There were no differential attrition rates between groups. As outlined in figure 1, at baseline, 112 participants completed the three 24-hour recalls, with 86 completing the 3-month follow-up data collection (77% retention), 74 completing 6-month recalls (66% retention) and 59 completing the 12-month recalls (53% retention). No adverse events were reported.
Baseline demographic and clinical characteristics of participants
Baseline scores and values for components of the Theory of Planned Behaviour for dropouts and stayers
Nutrition-related genetic variation among participants in the GLB+NGx group

Flow diagram of participants from baseline to 3-month, 6-month and 12 month follow-up. GLB, Group Lifestyle Balance; NGx, nutrigenomics.
Change in dietary intake
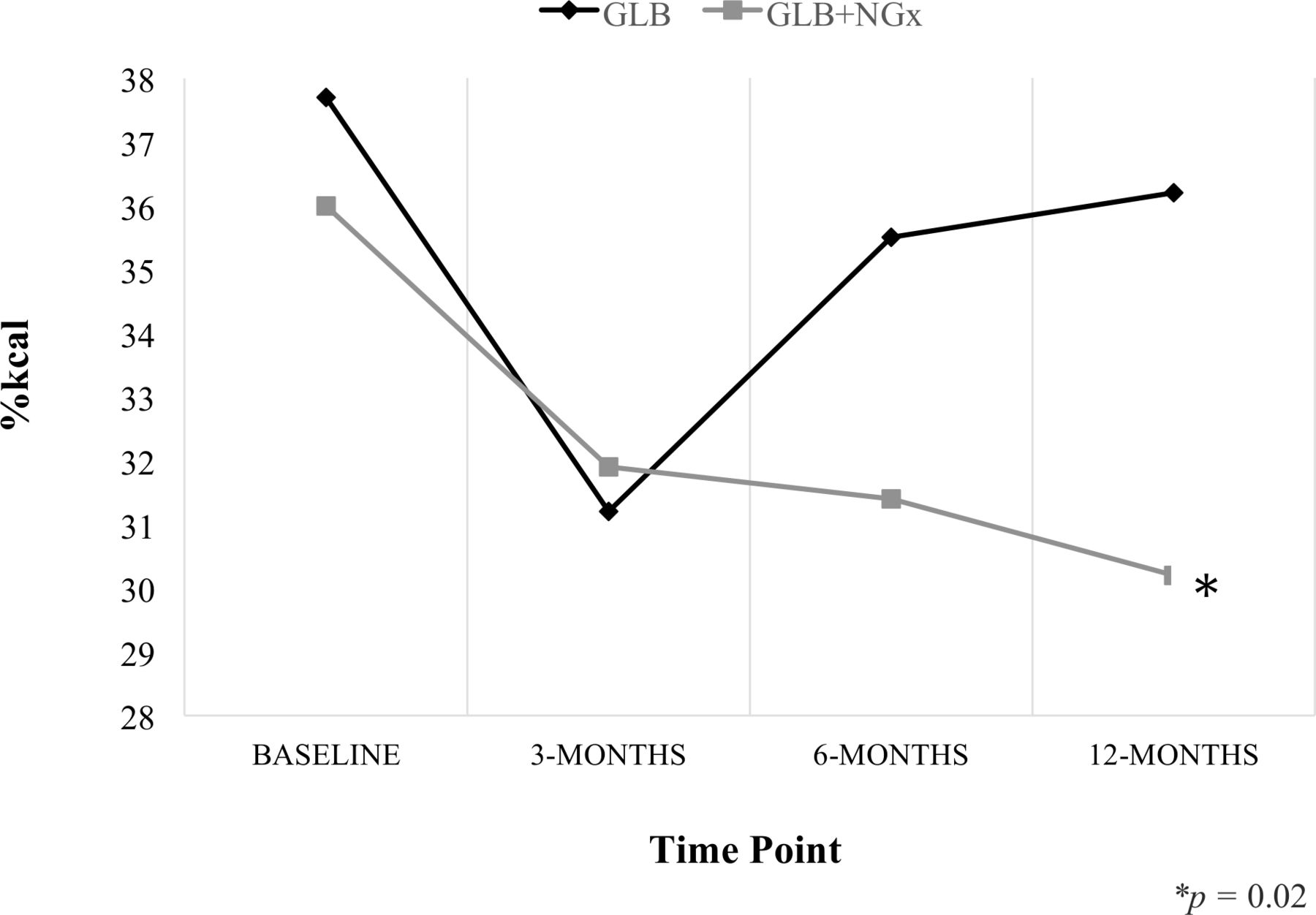
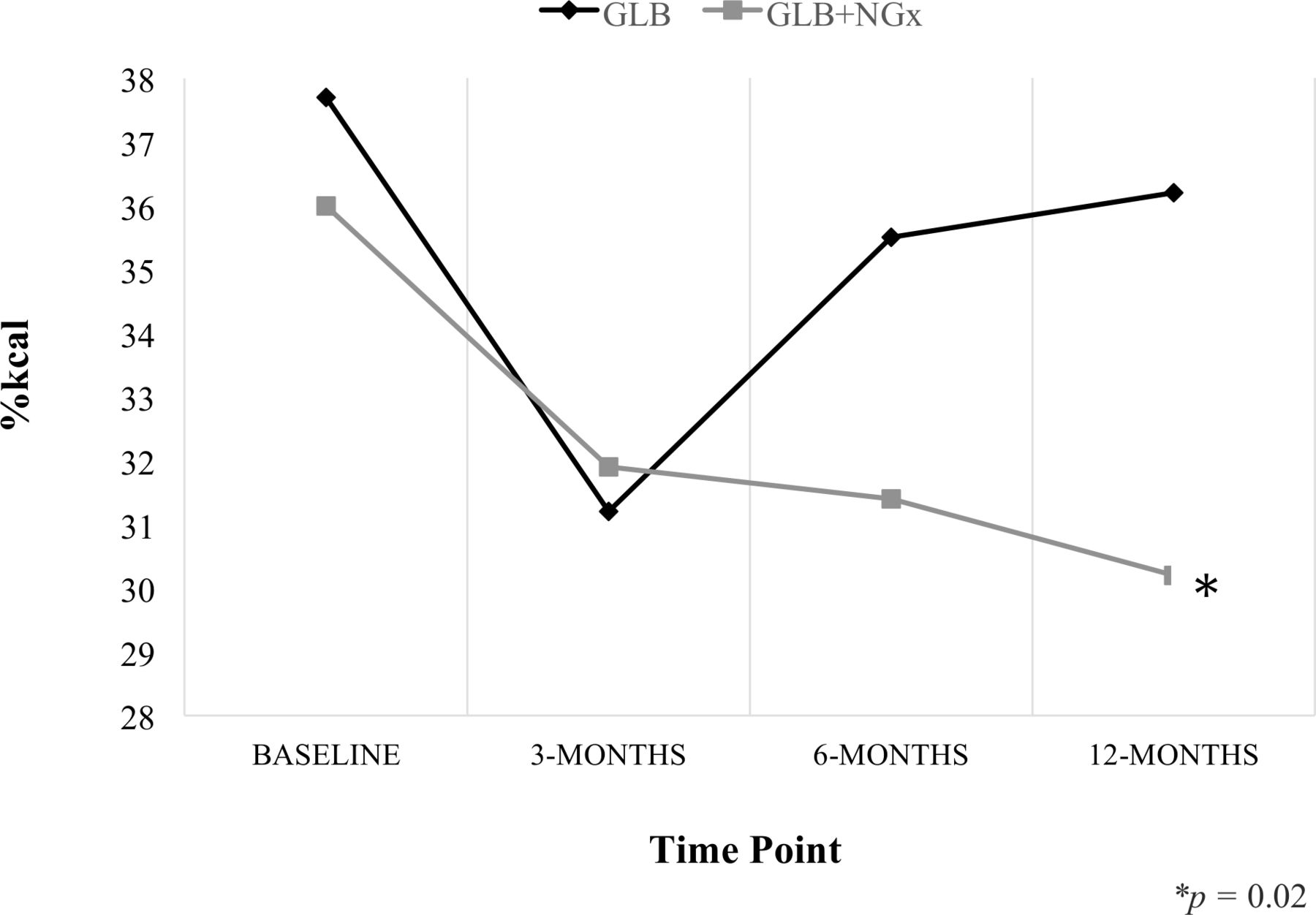
Change in dietary intake from baseline to 3-month, 6-month and 12-month follow-up is detailed in table 4. For the analysis of overall change in dietary intake throughout the entire duration of the study, a total of 32 participants completed the dietary recalls at all four time points. As further depicted in figure 2, only the GLB+NGx group significantly reduced total dietary fat intake from baseline to 12-month follow-up (from 36.0%±4.8% kcal to 30.2%±8.7% kcal, p=0.02). Furthermore, the GLB+NGx group experienced a clinically meaningful reduction in SFA intake (11.9%±3.3% kcal to 9.3%±3.3% kcal, p=0.13) and statistically significant reduction in grams, but not percent of calories (%kcal), of unsaturated fat. Overall, there were long-term (12 month) changes in dietary fat intake when participants in the GLB programme received the addition of nutrigenetic information and advice, while those receiving only population-based dietary information and advice did not significantly change their dietary fat intake long term.
{kind=link}
{kind=link}
Change in percent of calories from total fat. Significant reduction in total fat intake in the GLB+NGx group only (repeated-measures analysis of variance: p=0.02). GLB, Group Lifestyle Balance; NGx, nutrigenomics.
Overall change in dietary intake from baseline to 3-month, 6-month and 12-month follow-up
Dietary adherence
As further detailed in table 5, with more broad %kcal ranges, participants in the standard GLB group had significantly (p<0.01) greater adherence to the group-specific target for protein intake at all four time points (baseline, 3, 6 and 12 months) indicating that the group-specific targets in the GLB+NGx group were more difficult to achieve from the beginning. Similarly, with more broad %kcal ranges for total fat intake in the GLB+NGx ‘typical response’ group, participants in the GLB+NGx group had significantly (p<0.01) greater adherence to the group-based targets for total fat at all four time points, indicating that the target for total fat intake in the standard GLB group was more difficult to achieve. Interestingly, the GLB+NGx group had significantly greater long-term (12 months) adherence to the targets of <25% kcal from total fat (p<0.01) and <10% kcal from saturated fat (p=0.02), compared to the standard GLB group.
Differences between groups for dietary adherence at baseline, 3, 6 and 12 months
Discussion
This study demonstrates that a nutrigenomics weight management intervention can motivate greater long-term dietary change compared to population-based recommendations in one of the most effective public health weight management and diabetes prevention programmes. Notably, this is the first genetic testing behaviour change study to incorporate the TPB and thus control for important confounding factors of behaviour change and is the first study to assess changes in calorie and macronutrient intake resulting from a genetic-based weight management intervention. It is also the first study to assess change in dietary intake when the GLB/DPP programme is extended to patients with overweight/obesity, regardless of having a pre-diabetes diagnosis—a recommended programme expansion by public health officials.26
Previous research has assessed change in dietary intake in participants diagnosed with pre-diabetes enrolled in the GLB/DPP programme. Over the course of 12 months, it appears that the participants with pre-diabetes made greater overall dietary changes (−452 calories and −6.6% total fat) compared with the population of adults with overweight/obesity in the NOW trial who received the standard GLB programme (−236 calories and −1.5% total fat), although different tools were used to measure dietary intake, therefore the results cannot be compared with complete accuracy.27 Theoretical concepts of behaviour change support this finding; the extended parallel process model suggests that if individuals’ perceptions about susceptibility to a threat (eg, developing type 2 diabetes) and the magnitude of the threat are high, they are more likely to take action to control the threat (eg, improve their nutrition).28 Interestingly, the NOW trial GLB+NGx group (with overweight/obesity but not necessarily a pre-diabetes diagnosis) changed their dietary intake to a similar extent as those in the original GLB/DPP cohort, all of whom had a diagnosis of pre-diabetes, whereas the NOW trial standard GLB group made fewer changes to their diet.27 In comparing these findings to the extended parallel process model, it is possible that the addition of genetic-based nutrition information and advice positively impacted response efficacy (beliefs about the effectiveness of the advice to improve weight management), and elicited greater danger control responses (beliefs, attitudes, intentions and behaviours to manage weight).28 Future research should explore this concept further. Future research should also assess change in dietary intake in the GLB programme (with and without the addition of nutrigenomics information/advice) in various locations across North America, and with a more ethnically diverse study sample in order to improve generalisability. The current study is primarily generalisable to Caucasian females with overweight and obesity enrolled in a weight management programme. Notably, given the highly pragmatic nature of the NOW trial (table 6), overall, this study has strong external validity.
PRECIS-2 scoring tool
In terms of the dietary analyses, while both grams and %kcal are reported in the present study, %kcal is a more accurate comparison between groups given that calorie intakes between groups were not identical. As such, differences in %kcal from macronutrients should be weighted more highly in the interpretation of the overall results compared with grams of nutrients. Given that the %kcal from protein recommendations for the GLB+NGx ‘enhanced response’ group proved to be challenging to achieve, and that a large proportion of the GLB+NGx group were advised to limit their SFA intake to <10% kcal to enhance weight loss (table 3), it is not surprising that there was significantly greater dietary adherence to the SFA recommendations in the GLB+NGx group as many participants were focusing on reducing their SFA intake. This would also contribute to the significant reduction in total fat intake in the GLB+NGx group only (in addition to a reduction in unsaturated fat). It was, however, surprising to see minimal change in total fat intake and poor dietary adherence to the total fat recommendations in the standard GLB group at 12-month follow-up since this was the main focus of the standard programme. While clinically meaningful (although not statistically significant) reductions in total fat intake occurred from baseline to 3-month follow-up, these were not sustained after 12 months. As further explained above, it appears individuals with overweight/obesity, but not necessarily having a pre-diabetes diagnosis, have a more difficult time maintaining long-term dietary changes in the standard GLB programme compared with those diagnosed with pre-diabetes.27 According to the NOW trial findings, the addition of genetic-based dietary advice could help to mitigate this. Indeed, previous research has indicated that weight control is a motivator for the intention to adopt personalised nutrition strategies.29
Our finding that GLB+NGx group participants who dropped out at 3 months had a significantly lower income, on average, compared with 3-month dropouts from the standard GLB group was interesting. It is possible that purchasing food in order to adhere to the nutrigenomics intervention was perceived as, or in reality was, more expensive (eg, 30% of participants were advised to follow a higher protein nutrition plan) and cost may have been prohibitive to following the dietary advice. Studies have reported cost is a barrier to consumption of higher protein foods.30 31 However, the finding that dropouts from the GLB+NGx group tended to have lower incomes was not consistent after 6 and 12 months, and therefore, future research should explore this phenomenon further.
Strengths and limitations
There are several specific strengths and limitations of the present work that should be noted. This research was novel to the field, as it is one of only four completed RCTs assessing change in dietary intake resulting from a nutrigenetic intervention over a 12-month period. Previously, Hietaranta-Luoma et al similarly found that a nutrigenetic cardiovascular disease intervention motivated greater long-term changes in dietary intake, and further motivated greater short-term and moderate-term changes compared to a control group.32 Nielsen and El-Sohemy’s and Chao et al’s 12-month RCTs also found that nutrigenomics interventions motivated greater long-term (12 months) changes in nutritional intake.33 34 There have been no RCTs demonstrating that nutrigenomics is ineffective at motivating changes in dietary intake after 12-month follow-up.8 Thus, taken together, the body of evidence highly suggests that nutrigenomics is a useful tool for motivating positive nutritional intake over the long term.
Consistent with the vast majority of nutrition research, there were limitations related to the methods used to collect dietary intake data such as possible recall bias and under-reporting of intake.35 However, three 24-hour recalls were collected using the multiple-pass method, which has been validated against direct observation in a similar population.25 Additionally, these 3 days of dietary recalls provided highly detailed nutritional intake data, which is a strength of this dietary collection method.35 Nonetheless, collecting three 24-hour recalls is a time-consuming process, leading to respondent burden,35 which helps to explain why a smaller subset of the NOW trial sample participated in three 24-hour recall data collection throughout the entire duration of the study. In addition, three 24-hour recalls were collected over the phone, whereas other NOW trial outcome data (eg, weight and body composition) were collected in-person,17 24 leading to slightly different samples as some participants completed only the three 24-hour recalls, while others completed only the in-person data collection, and others completed both.
Since the dietary analysis was a secondary outcome of the NOW trial (and sample size calculations are based on the primary outcome), the sample size may not have been large enough to detect statistical significance in some cases. For example, while adherence to SFA was significantly greater (p=0.02) in the GLB+NGx group compared with the standard GLB group, a 12-month clinically meaningful reduction in SFA was observed in the GLB+NGx group only (11.9%±3.3% kcal to 9.3%±3.3% kcal), but this change was not statistically significant (p=0.13). Nonetheless, this was a notable observation given that in addition to possible weight-related outcomes resulting from a decrease in SFA to <10% kcal from saturated fat,36 achieving <10% kcal from SFA can have further beneficial effects on LDL-cholesterol and other cardiovascular disease risk factors.37 Future research should seek to replicate this study in an RCT adequately powered to detect significant differences in %kcal from SFA. Nonetheless, this long-term 22% reduction in SFA observed in the GLB+NGx group is notable and relates to the statistically significant greater adherence to the SFA guidelines after 12 months in the GLB+NGx group compared to the standard GLB group.
Lastly, baseline portion sizes were likely under-reported given that baseline data collection occurred during the run-in period and participants were taught how to measure their food and beverage intake in the first week of the intervention. This may have affected the results for calories and grams of nutrients (but not percent of intake from macronutrients). However, since participants were advised to measure all food and beverages for 1 week and track their intake for 2 to 3 months, this likely improved the accuracy of the follow-up 24-hour recalls. Thus, the actual change in dietary intake may in fact have been greater than the data suggest.
Conclusion
Overall, the NOW trial has provided important, novel insights into genetic testing behaviour change research, grounded in fundamental theoretical concepts. The results of this study provide convincing evidence that the addition of nutrigenomics to one of the most effective public health weight management and diabetes prevention programmes can help motivate and optimise long-term, clinically meaningful differences in nutritional intake and adherence to dietary guidelines.
Acknowledgments
The authors would like to acknowledge the NOW Experiential Learning Group at Brescia University College for their contribution to data collection.
References
Footnotes
Twitter @justinehorneRD, @westernprof, @bresciaprof, @Jamie_Seabrook1
Contributors All authors (JH, JG, JS, CO and JM) were involved in designing the study. JH conducted the study at the East Elgin Family Health Team, wrote the first manuscript draft and revised subsequent drafts. JH and JS completed the statistical analyses. All authors (JH, JG, JS, CO and JM) revised manuscript drafts and approved the final manuscript.
Funding This project was supported by a grant from Brescia University College. Nutrigenomix provided complimentary genetic test kits and laboratory analysis. JH was supported through an Ontario Graduate Scholarship, Ontario Respiratory Care Society Fellowship, and Canadian Institutes of Health Research Frederick Banting and Charles Best Doctoral Award.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Western University Research Ethics Board and registered with clinicaltrials.gov (NCT03015012).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Please contact the corresponding author with any requests.