Article Text

Abstract
Background A bidirectional relationship exists between the brain and the gastrointestinal tract. Foods containing bacteria that positively influence the gastrointestinal microbiome are termed, probiotics; compounds that promote the flourishing of these bacteria are termed, prebiotics. Whether microbiome influencing therapies could treat psychiatric conditions, including depression and anxiety, is an area of interest. Presently, no established consensus for such treatment exists.
Methods This systematic review analyses databases and grey literature sites to investigate pre and/or probiotics as treatments for depression and/or anxiety disorders. Articles included are from within 15 years. Pre-determined inclusion exclusion criteria were applied, and articles were appraised for their quality using a modified-CASP checklist. This review focuses specifically on quantitative measures from patients with clinical diagnoses of depression and/or anxiety disorders.
Results 7 studies were identified. All demonstrated significant improvements in one or more of the outcomes measuring the of effect taking pre/probiotics compared with no treatment/placebo, or when compared to baseline measurements.
Discussion Our review suggests utilising pre/probiotic may be a potentially useful adjunctive treatment. Furthermore, patients with certain co-morbidities, such as IBS, might experience greater benefits from such treatments, given that pre/probiotic are useful treatments for other conditions that were not the primary focus of this discourse. Our results are limited by several factors: sample sizes (adequate, though not robust); short study durations, long-term effects and propensity for remission undetermined.
Conclusion Our results affirm that pre/probiotic therapy warrants further investigation. Efforts should aim to elucidate whether the perceived efficacy of pre/probiotic therapy in depression and/or anxiety disorders can be replicated in larger test populations, and whether such effects are maintained through continued treatment, or post cessation. Interventions should also be investigated in isolation, not combination, to ascertain where the observed effects are attributable to. Efforts to produce mechanistic explanations for such effect should be a priority.
- microbiome
- mental health
- nutritional treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Humans are an amalgamation of both ‘self’ material and a plethora of ‘non-self’ microorganisms, termed microbiota. These two entities are interactive, and their symbiotic co-existence is crucial for maintaining health.
An ecosystem of microbiota is collectively known as a microbiome. One such example exists within the human gastrointestinal tract (GIT). A highly developed bidirectional relationship exists between the central nervous system (CNS) and the GIT (including the microbiota colonising the GIT), with each area seemingly capable of influencing the condition and functionality of the other. This relationship is termed the gut–brain axis (GBA).1–4 The potential effects of the GBA on physiology and pathophysiology are too vast to be covered in one review. Therefore, in light of the current mental health crisis, we have chosen to focus on the GBA’s relationship with ‘common mental disorder’ (CMD).
It is theorised that the behaviours, cognitive capacities and even the emotions of an individual may not be determined entirely by their nervous system, but also by the colonising GIT microbiota. The mechanistic details underpinning the GBA are complex and yet to be fully elucidated. However, it has already been identified that crucial to facilitating this interaction are: immunomodulatory mechanisms; afferent and efferent neuronal signalling afforded by the vagal nerve; and bidirectional enteroendocrine signalling.2 5
Many factors influence the GIT microbiome, from the mode of delivery at birth to genetic and epigenetic variables. One of the most significant influences is diet.4 Foods containing microbiota thought to exert a positive influence on an individual’s GIT microbiome are termed probiotics, and food types that promote the growth or flourishing of these bacteria are termed prebiotics.4 5 The growing appreciation of the interconnectedness between the GIT microbiome and the nervous system, combined with the knowledge that pre/probiotics can alter the condition and constitution of the GIT microbiome, has highlighted pre/probiotics as potentially therapeutically valuable agents in the treatment of certain psychiatric conditions.6 Among the conditions being investigated are anxiety disorders and depression. The extent to which pre/probiotics might be therapeutically useful (or even viable) in treating anxiety and/or depression is presently unknown, which provides a reasonable rationale for exploring their potential value. To better understand this, we will contemplate some of the mechanisms already identified as key for GBA interactions alongside existing experimental findings.
GBA mechanisms
The vagus nerve
The immune system is crucial in mediating the GBA interactions.1 2 7 At least two mechanisms for this have been described. Experimental findings suggest the vagus nerve is integral in mediating GBA interactions.8 Components of microbiota recognised as non-self provoke cells of the innate immune system to release pro-inflammatory cytokines. The presence of pro-inflammatory cytokines influences neuronal physiology via vagal nerve stimulation.5 9 Numerous animal studies support this and indicate that microbiota-induced effects on neuronal physiology can affect behaviour. For example, mice that were administered Bifidobactium longum to induce gut dysbiosis exhibited anxiolytic effects compared with control subjects; subsequent vagotomy blocked this effect.10
Signalling molecules
Neuronal biochemistry can also be affected by direct action of cytokines that cross the blood–brain barrier (BBB).9 Cytokines are produced when GIT microbiota or their metabolites gain access to the systemic circulation.11–13 This process is thought to be part of the pathophysiology of multiple medical conditions. For example, patients with depression show increased GIT permeability, which may enable luminal microbiota to enter systemic circulation and trigger pro-inflammatory states.12–14 Certain microorganisms are associated with such effects, while others appear to oppose these actions. Various lactobacilli and bifidobacteria strains—typically commensal within healthy human GIT microbiomes—have been shown to attenuate the presence of pro-inflammatory cytokines within he systematic circulation when administered as probiotic supplements.2 9 15 Contrastingly, other microbiota have been shown to exert the opposite effect. This may be significant, given that neuroinflammation has been identified as being key in the pathogenesis of multiple psychiatric conditions including both anxiety disorder and major depressive disorders (MDDs).9–14
Cross-talk
There is evidence indicating GIT microbiota affect the functioning of luminal GIT cells, which may affect host behaviour via endocrinal signalling. Microbial metabolites, such as short chain fatty acid (SCFA), are thought to have this effect.3 Certain commensals produce SCFAs by fermenting non-digestible dietary carbohydrates, like dietary fibre, as part of their natural physiology (fermentable compounds such as these are examples of prebiotics).2 5 SCFAs directly affect enteroendocrine cells within the GIT, triggering the release of various compounds including cholecystokinin and glucagon-like peptide 1. These compounds are endocrinologically active, and may induce changes in host physiology and behaviour—such as triggering satiety.3 Microbiota–host interactions of this nature are termed ‘cross-talk’.
Numerous compounds have been identified as potentially capable of influencing host behaviour by cross-talk. Tryptophan (TRP), a precursor of the neurotransmitter serotonin, is one such example.16 It is possible that cross-talk mechanisms may form part of the pathophysiology of anxiety disorders and/or depression, which highlights them as potentially utilisable therapeutic avenues for treating these conditions.11 16 Finally, it must be highlighted that the mechanisms by which GBA interactions are enacted suggest that the effects microbiota have on their host physiologically, or during pathophysiological states, may be detectable within the host’s biochemical profile. As such, it may prove useful to consider any effects that pre/probiotics have in humans through biochemical analysis, in addition to considering the global state of an individual subjectively and objectively.
Psychiatric disorders in society
The mechanisms and findings outlined provide a succinct tour of some of the information GBA studies have produced. Collectively, they indicate the necessity for further investigation; however, what they neglect to highlight is the importance that such research might hold within the context of clinical practice—particularly with regard to anxiety and depression. According to 2014 UK governmental statistics, 17% of people report experiencing the effects of a CMD weekly.17 CMD encompasses multiple conditions. Of these, anxiety disorders and depression are, respectively, the first and second largest contributors to this figure, comprising >9%. This review will focus on depression and anxiety as their symptoms are easier to quantify than other CMDs, yet still represent a significant proportion of CMDs as a whole. The prevalence of CMDs has consistently increased in adults, irrespective of age and gender, since 1993. In 2016/17, 1.4 million patients were referred with a clinical diagnosis of a CMD, 53% with a diagnosis of an anxiety or stress-related disorder and 33% with depression. The UK has a target for 50% of patients referred for anxiety disorder and depression—who complete treatment—to shift from a clinically recognised condition to a subclinical state. This target has not been met.17
These figures are included not to suggest that the treatment of anxiety and/or depression is failing, but to highlight the difficulty in treating such conditions. Our collective understanding of psychiatric disorders (and, broadly speaking, of mental health) is still developing, meaning it is vital to ensure our clinical approaches are multifaceted and evolving. The nascent field of ‘nutritional psychology’ could offer a way to enhance the efficacy of current treatments and/or provide novel treatments.
Recent reviews exploring pre/probiotic supplementation in other psychiatric disorders yielded null conclusions. However, this could be as a result of the heterogeneity of the studies included.18 19 Whether pre/probiotics are useful agents in the treatment of CMDs remains to be determined, though the pressing need for alternative treatment options, combined with the underlying scientific rationale supporting their potential efficacy, is reason enough to explore their worth further.
Objective
This review aims to ascertain whether individuals living with a clinically diagnosed anxiety disorder and/or depression can have a quantitatively measured reduction in the negative experience of their CMD by consuming a diet inclusive of prebiotics and/or probiotics, alongside any other treatment indicated in the National Institute for Health and Care Exellence (NICE) guidelines.
Population, intervention, comparison, outcome (PICO)
To inform the above objective, this review employs the population, intervention, comparison, outcome (PICO) framework detailed in table 1.
PICO information
Methods
A literature review was conducted using the PICO framework to structure the objective. Selected papers were appraised and scored using the Critical Appraisal Skills Programme (CASP) method. The bias of the selected papers was assessed using the Cochrane-risk-of-bias tool. The obtained data were then analysed against the objectives.
Eligibility criteria
While reviews exploring probiotics and anxiety and depression exist, there are no reviews that exclusively explore probiotics to supplement an existing treatment plan. In order to address this, specific criteria were outlined before conducting the literature search to identify suitable studies.
Inclusion criteria
Studies were identified for further consideration and potential inclusion if they met the following criteria: the study population must comprise human adults aged 18 and older; participants had a clinically recognised anxiety disorder and/or depression; participants received a dietary intervention of a prebiotic and/or probiotic; study findings must be expressed, at least in part, quantitatively; studies must have been published within the last 15 years (January 2003 to January 2019—the selected time period serves to differentiate between when information concerning microbiota was determined by bacterial culturing methods rather than the significantly more robust contemporary methods that utilise genomic sequencing to ascertain, with greater precision, which microbiota are present in an individual’s GIT); studies must present primary data—that is, they are not systematic reviews or review articles (however, articles of this nature were read to identify additional appropriate studies); studies must be available in the English language.
Exclusion criteria
Studies were excluded if any of the following conditions were applicable: participants were concurrently receiving any treatment that was in dispute of NICE guidelines (provided that a study participant had not been sectioned under the Mental Health Act (or equivalent), then there was no requirement that that individual should receive any form of treatment; as such, patients acting with informed consent who chose not to receive any aspect of the treatment protocol outlined in NICE guidelines, but chose to receive a dietary intervention in a study, were suitable for inclusion in this review—studies were only excluded when they appeared to be in dispute of NICE guidelines); the study investigated the effect of prebiotics and/or probiotics without regard for anxiety disorders and/or depression; the study’s findings were produced from animal models; the study’s findings were expressed only qualitatively; the study’s method or quality were deemed to be of a poor standard; the study was in disaccord with outlined inclusion criteria.
Sources in accord with the predetermined inclusion criteria and not exhibiting characteristics outlined in the exclusion criteria were deemed suitable for further investigation.
Information sources
With the eligibility criteria determined, a literature search was conducted.
Database searching
A systematic search was carried out of the following databases: MEDLINE, Embase, PsychINFO, AMED, Cochrane Library, PubMed and Web of Science. Limits applied were: publication date range 2003–2019, human studies, age >18 years, and English language.
Search strategy
A search strategy was devised and adapted to each database as required. The finalised search consisted of [Depress* OR “Low mood” OR Anxi* OR Stress* OR “Mental Health”] AND [prebiotic* OR probiotic* OR psychobiotic OR probiotic/tu OR “probiotic supplementation” OR symbiotic* OR bifidobac* OR bifidogenic OR “Gastrointestinal microbiome” OR “gut-brain axis” OR lactobac*].
Hand searching
To ensure relevant data were not missed, hand searching of ‘grey literature’ was also conducted. This consisted of advanced Google searching of specific domains likely to produce relevant findings. Specifically, the domains ‘nhs.net’ and ‘gov.uk’ were searched. Data were also yielded by searching relevant websites including the British Dietetic Association, NICE guidelines, NICE evidence search, MIND, and Web of Science conference archives.
Expert network consultations
Finally, to further minimise the possibility of missing any relevant findings, the scientific director of the American Gut Project and the lead of Dietary Intervention Studies at Cork University Ireland’s APC Microbiome project were contacted for their expert opinion regarding sources, unpublished conference findings or contemporary research relevant for this review. No previously unidentified sources were yielded.
Results
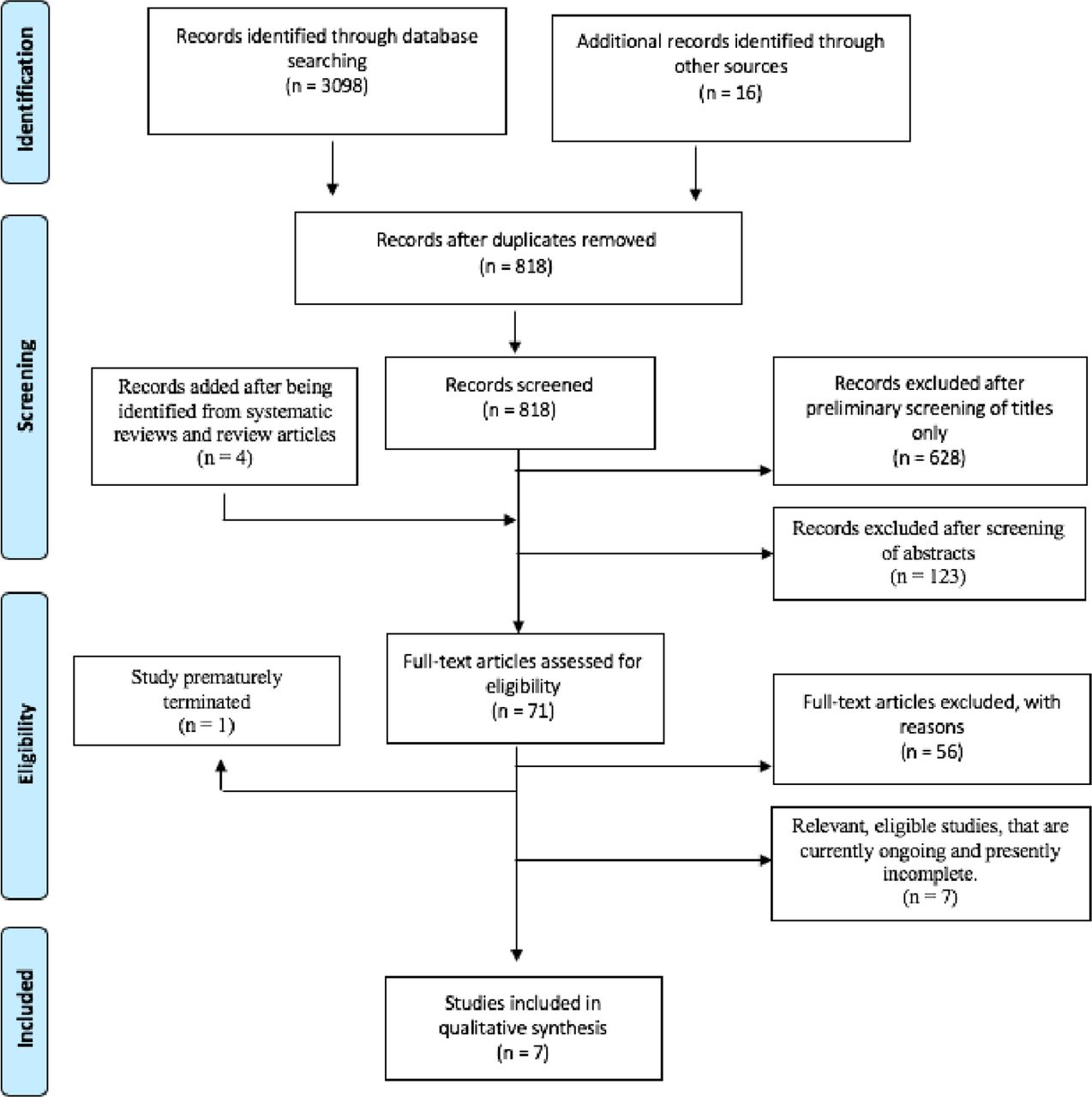
The outlined searching strategy was applied. The results of this are detailed below in Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart format. (figure 1)
{kind=link}
An adapted PRISMA flowchart detailing search results acquired by actioning the strategy detailed in the Methods section. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyses.
Study screening
Of the articles identified, 67 were deemed suitable for thorough evaluation. Non-primary sources were unsuitable for inclusion; however, they were included in a thorough evaluation to identify additional relevant articles, yielding a further four papers. Of this total of 71 articles, 56 were in breach of the pre-determined inclusion/exclusion criteria and were removed. Seven studies were ongoing, with results therefore unavailable—these were also excluded. One study was prematurely terminated.
Study selection
A total of seven articles were selected for inclusion. Key discriminators throughout this process included: studies conducted on non-human subjects; studies conducted on human subjects that lacked a clinical diagnosis; and studies that determined effect through non-quantitative measures. By adhering to the pre-determined conditions for this review, the studies identified investigated only populations with diagnosed depression (n=7); no suitable study investigated patients primarily for an anxiety disorder (n=0). However, given that certain included articles assess anxiety specifically within their test cohort, and that certain measured outcomes are highly relevant for assessing anxiety as well as depression (stress evaluators, or plasma cortisol, for example), both conditions will still be considered when evaluating the following results.
All seven studies investigated at least one probiotic strain; 3/7 studies investigated a single probiotic strain as an intervention, while 4/7 studies investigated the effect of administering multiple probiotic strains as a combined intervention. A total of 12 strains were investigated; most commonly tested were Lactobacillus acidophilus (tested in three articles), Lactobacillus casaei and Bifidobacterium bifidium (tested in two articles each). One study investigated combined prebiotic–probiotic therapy, and one article investigated isolated prebiotic therapy.
Article appraisal and data extraction
The salient details of the articles are presented in table 2, along with each study’s modified-CASP appraisal score.
Details of the articles, along with each study's modified CASP appraisal score
The risk of key biases present within each study
Bias
Risk of bias in studies
The Cochrane risk-of-bias tool was employed to assess bias within the studies. Studies were reviewed with respect to the outlined sub-categories within this tool and graded for risk of bias into the categories high, low, unclear or N/A. Table 3 details this.
Discussion
Results impression
There is significant clinical and methodological heterogeneity within this review which prevents meta-analysis. The nuances of the investigated populations, the variety of measured outcomes employed to evaluate interventions, and the variety of pre/probiotics that exist (and the multitude of experimental approaches/combinations of these) are examples of some of the factors contributing to this heterogeneity. Despite this, the results indicate a common finding—a link may exist between probiotic/prebiotic–probiotic supplementation and reductions in quantitative measures of depression.
Key findings
Three of seven studies showed insignificant changes for certain outcomes; however, these were generally biochemical measures. Prebiotics, when investigated as isolated therapies, incurred non-statistically significant results.20–22 However, in no study do the measured outcomes indicate pre/probiotic interventions increase, or negatively impact, measures of anxiety/depression. Furthermore, every study demonstrated a significant, quantitatively evident, decrease/improvement of symptoms and/or biochemically relevant measures of anxiety and/or depression for probiotic or combined prebiotic–probiotic use. This is observed regardless of the specific probiotic, method of administration or length of trial, across all test cohorts, irrespective of depression severity or additional comorbidities.20–26 The current evidence indicates: prebiotics are unlikely to be effective as an isolate therapy for depression within the timeframes investigated21 25; probiotics may be useful agents20–26; concomitant prebiotic–probiotic therapy may also be useful, though it is not obvious whether these agents function synergistically from this cohort of studies.21 25 The results offer some insights into pre/probiotic use for anxiety, though these are largely limited, with no test cohort being investigated primarily for an anxiety disorder (though some test populations have clinically significant comorbid anxiety disorders).26
Interpreting questionnaire results
The 17 item Hamilton Depression Rating Scale (HAM-D-17) and Beck Depression Inventory II (BDI-II) were the two most commonly employed methods for evaluating subjects’ psychiatric condition pre/during/post invention. Probiotic/combined prebiotic–probiotic therapy significantly reduced patient scores on these tests in 6/7 studies.21–26 The exception, Rudzki et al,20 found no link between probiotic use and changes in HAM-D-17 scores. There were no significant effects on depression and anxiety symptoms with the Symptom Checklist-90 and Perceived Stress Scale-10.20 The intervention in this study was Lactobacillus plantarum 299V; interestingly, no other study investigated this bacterial strain. Despite this, notable effects were seen following L. plantarum administration with respect to the cognitive functions of test subjects and for certain biochemical measures. Considering this, it is reasonable to suggest that L. plantarum may be functionally active via the GBA (hence its effect on cognition), but its influence pertains less to factors affecting depression and/or anxiety.
Furthermore, this finding indicates that, of the 12 different probiotics investigated, 11 were potentially useful agents. The effect measured by HAM-D-17 and BDI-II is perhaps best appreciated when considering Kazemi et al 21 and Ghorbani et al.25 These papers scored the joint highest and joint second highest during appraisal, respectively, and had the lowest risks of bias. Both articles demonstrated marked improvement in BDI-II or HAM-D-17 scores in patients supplemented with probiotics (Kazemi—mean BDI-II—probiotic group: 18.25 at baseline–>9.0 end of trial; placebo: 18.74–>15.55. Ghorbani—mean HAM-D-17—prebiotic-probiotic group: 22.90–>3.65 (1.71 SD); placebo: 22.55–>4.80 (2.05 SD). Interestingly, this effect is present in quite different cohorts. Ghorbani et al investigated subjects with moderate severity depression, while Kazemi et al studied patients with more severe MDD who were simultaneously using selective serotonin reuptake inhibitor (SSRIs). This may suggest that any positive effect derived from probiotic administration would be felt across a variety of depression severities, and that such an effect would be independent of—even additional to—the effects gained from conventional NICE guidelines treatment, such as SSRIs.21 25 This is further supported in Bambling et al,26 where improvements noted in participant’s mean quality of life (QoL) scores after 8 weeks of daily probiotic use (57.5 at week 1–>70.0 at week 8) were undone after 8 weeks post-treatment cessation (average scores returned to baseline levels: 70.0 at week 8–>56.7 at week 16). Participants of this study had highly treatment-resistant MDD, though still appeared to experience some benefit from probiotic use. It is also noteworthy that, within this cohort, the most common comorbidity to treatment-resistant MDD was an anxiety disorder, of which 60% of subjects also met the necessary criteria.26 Under these circumstances, QoL scoring can serve, at least in part, as a measure of the effect of probiotics on both anxiety and depression as comorbidities.
Potential mechanisms underlying the observed results
It should be noted that while disruption to the GBA is common across a wide range of disorders, our understanding of the GBA is limited. Much of the current research into its mechanisms has been conducted on animal models; with a limited number of human studies, we cannot say with certainty whether increased serotonin levels in the gut are responsible for a cascade of molecular events that influence neuronal activity. However, the findings of this review lead us to question what mechanisms might be driving such effects.
Pro-inflammatory cytokines and immune responses
As outlined above, immunomodulatory mechanisms are thought to be key in mediating GBA interactions.3 9 13 14 However, studies that assessed immune function through serum measurements of pro-inflammatory cytokines or by directly assessing immune cell functions all found insignificant changes between test and control groups (Rudzki—TNFα, IL-6 and IL-1b: 1.70, 2.05 and 0.16, respectively, at baseline; 1.78, 2.19 and 0.36, respectively, post-intervention. Akkasheh—assessment of B cell function: 29.8 at baseline–>22.7 end of trial, all changes statistically insignificant). However, it should be appreciated that sampling cerebrospinal fluid might have offered more useful information regarding CMDs than circulating blood samples.20 22 Nonetheless, this finding is surprising as it is suggested that in many conditions where probiotics are seen to be useful therapeutic agents, their usefulness is related to their capacity to reduce immune production of endogenous, pro-inflammatory compounds—such as cytokines—as is the case in ulcerative colitis.27 28 Given the strength of evidence supporting the claim that there may be an underlying inflammatory basis in the pathogenesis of certain CMDs—including depression—such a mechanism would have been fitting.2 13 14 The absence of such a finding certainly does not indicate such mechanisms are insubstantial in GBA actions or in the pathogenesis of psychiatric conditions. However, it does suggest that other mechanisms may be mediating the observed effects. Another mechanism that may potentially be significant in explaining the aforementioned findings relates to the compound TRP and its metabolic pathways.
Tryptophan
TRP has been identified as potentially important in GBA interactions in psychiatric disorders as its metabolic pathways hypothetically could enable microbiota to have cross-talk interactions with their host.2 3 12 TRP is a metabolic precursor for serotonin and is present in the systemic circulation; it can cross the BBB, with the potential to raise serotonin levels in the CNS.29 However, TRP may instead progress down the kynurenine (KYN) pathway, from which serotonin cannot be synthesised.29 30 Microbiota have a modulatory effect over which metabolic pathway TRP progresses down.30–32 Considering the role that serotonin levels within the CNS have on the pathogenesis of CMDs, the effect probiotics have on TRP and KYN levels is of interest and might partially explain the global effects observed in test subjects.
Both Rudzki et al and Kazemi et al considered TRP, KYN and KYN:TRP ratios. Kazemi et al also considered KYN levels adjusted for isoleucine concentration, as isoleucine can reduce KYN concentration.33 Kazemi et al found a significant decrease in KYN and adjusted-KYN:TRP ratio in placebo versus probiotic (KYN (nmol/L)—placebo: 772.89–>798.49; probiotic: 757.59–>722.47. KYN:TRP (nmol/μg)—placebo: 11.0–>12.4; probiotic: 11.23–>9.58). Rudzki et al found decreased KYN (placebo: 2.17–>2.32; probiotic: 2.05–>1.82), but insignificant differences in KYN:TRP ratio between placebo and probiotic groups (KYN:TRP (both measured in μmol/L)—placebo: 0.04–>0.04; probiotic 0.04–>0.03). Rudzki et al’s KYN:TRP ratio, however, was non-adjusted for amino acids and may therefore be less insightful. Decreased KYN may in fact be a more significant finding, given that available TRP may have been converted into serotonin in the probiotic group, which could offer an explanation for the improvements observed in their performance in tasks assessing cognitive function.31 Furthermore, probiotics, including Lactobacillus plantarum 299 v specifically, have been shown to increase serotonin biosynthesis, which further strengthens this point.34 In either case, probiotic supplementation seemingly initiated biochemical changes in depressed patients for compounds considered to be significant in the pathogenesis of CMDs. This indicates further investigation is required into the effects of probiotics on TRP, KYN and other metabolic compounds, as they may offer insights into why the articles in this review resoundingly indicate that probiotics can improve symptoms of anxiety and depression in a quantitative sense.
Implications of findings
It is crucial that these findings are appreciated with regard to the clinical contexts in which they would be applied. For practical purposes, we try to observe the effect of an intervention on a condition in an isolated manner; however, this can overemphasise the clinical significance of the data. The reality is that anxiety disorders and depression affect individuals in a multitude of ways, manifest in multiple bodily systems, and arise in patients who may have other comorbidities. While one person might experience gastrointestinal symptoms as a result of their primary illness, another may find their cardiovascular health more affected. In essence, the effects of psychiatric morbidity are diffuse, variable and require treatment approaches that adequately appreciate their complexity—at the risk of cliché, they require a holistic approach. In this way, with a better understanding of its mechanisms, probiotics may prove to be a useful tool across a wide range of conditions.
Evidence exists supporting the benefits of probiotics in the treatment of numerous morbidities—from infectious/antibiotic-induced diarrhoea and irritable bowel syndrome (IBS) to autoimmune conditions such as ulcerative colitis.32 34 35 Microbiome studies are novel, and it is likely more information will surface as research continues—for example, preliminary data already suggest probiotics may be useful for the prevention of obesity and type 1 and type 2 diabetes. In fact, in this review, Akkasheh et al 22 demonstrate that probiotics significantly lower serum insulin concentration and resistance, while Majeed et al 23 showed significance decreases in intervention group scores for the Gastrointestinal Discomfort Questionnaire (GI-DQ), Modified Epworth Sleepiness Scale (mESS) and the Irritable Bowel Syndrome Quality of Life questionnaire (IBS-QoL).36 This information is of particular significance as patients with anxiety disorders and depression are predisposed to numerous comorbidities, including impaired insulin functioning and IBS.37 As such, the effect that probiotics have on patients with CMDs may be twofold: they may directly improve depression in line with the observed findings of this review, and/or they might beneficially impact a patient’s experience of their CMD by alleviating additional comorbidities. The overlap of conditions more commonly arising in patients with CMDs and conditions that probiotics may be useful for treating highlights the exciting potential that the clinical application of probiotic agents may hold for certain patient groups.
Limitations
There are some limitations affecting this review. First, it is acknowledged that while the review shows no negative effects of pre/probiotics, this could be a reflection of a positive reporting bias; this is supported by evidence that highlights a lack of systematic reporting of adverse events in connection with probiotic interventions.38 Further to this, a number of the interventions administered contained a combination of compounds—be this multiple probiotics, or other ingredients. Therefore, it cannot be ascertained with certainty which product is responsible for the observed results or whether a specific combination is required for such an effect. There is also anecdotal evidence that prebiotics may worsen outcomes under specific treatment conditions.39 The findings thus point more towards products that warrant further investigation in isolation or in combinations whereby effects can be better understood, rather than indicating the value of a specific product. An existing study highlights that a more appropriate study methodology would be to assess disease-specific and strain-specific efficacy.40 In the selected papers, study durations were short and populations small, meaning they were unable to provide full clarity on the effect the interventions might have. There was also a notable difference in sample sizes between studies with significantly fewer data for probiotic interventions. Without balanced data, a larger scale or longer trials, one cannot gain accurate information regarding: the overall effect of an intervention; whether the effects seen are lasting, long-acting or temporary; or whether there are any long-term dangers or complications associated with the prolonged use of the intervention. Thirdly, it should be noted that, while the studies are generally uniform in indicating the usefulness of probiotic-containing products for patients with clinically diagnosed depression, there is little scope to posit their use for patients affected by an anxiety disorder in the absence of depression. No studies were identified investigating this population without having additional confounding factors that made their results less relevant/useful; additional work is required to clarify whether such products might benefit this patient group. It should also be noted that even though the studies are widely in accordance in their findings, the included studies are of variable quality and subject to different degrees of bias. Finally, this review does not include papers published within the last year and therefore the conclusions may not necessarily reflect the most recently published data.
Conclusion
Our results affirm that pre/probiotic therapy warrants further investigation. Efforts should aim to elucidate whether the perceived potential efficacy of pre/probiotic therapy in depression and/or anxiety disorders can be replicated in larger test populations, and whether any effects are maintained through continued treatment, or post-cessation. Specific interventions should be investigated in isolation, not combination, to ascertain from where the observed effects arise. Detailing mechanistic explanations for any effects should be a priority. Consideration and research effort should also be directed towards identifying patient groups that may experience greater benefits of pre/probiotic therapy due to their own individual idiosyncrasies; as previously discussed, patients with comorbid depression and IBS may be such a group. Finally, it is imperative that biochemical analysis is included in our interpretation of the effects of microbiome studies. A biochemical focus may highlight processes that precede or follow notable changes in an individual, which could offer new insights or affirm present theories regarding why particular outcomes occur. This would provide a useful contribution to the growing literature for microbiome studies and may even inform our understanding of physiology and pathophysiology generally.
These preliminary findings suggest continued investigation, on a larger scale and over a longer time period, would be appropriate. However, purely from the information gathered in this review, it is valid to suggest that, for patients with clinically recognised depression: isolate, or adjuvant, prebiotic therapy is unlikely to affect an individual’s experience of their condition in a quantitatively evident way; and that isolate, or adjuvant, probiotic/combined prebiotic–probiotic therapy may offer a quantitatively measurable improvement in parameters relating to depression. However, there are inadequate data to suggest anything meaningful to support or refute the use of either pre/probiotic agents (or a combination of both) in patients with clinically recognised anxiety disorders; this would be a useful area to investigate further.
Acknowledgments
Special thanks to Librarian, Lisa McLaren, for her patience and advice during the review process. We are grateful to the NNEdPro Global Centre for Nutrition and Health for assistance towards APC costs.
References
Supplementary materials
Footnotes
Twitter @macaninch
Contributors SN acted as the main author of this project. MZ provided review, editing and amendments. EM assisted with methods, editing and supervision. KM offered senior supervision and final editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing is not applicable as no datasets were generated and/or analysed for this study.