Article Text

Abstract
Background Currently, there is an unmet clinical need in identifying and screening women at high risk of breast cancer, where tumours are often aggressive and treatment intervention is too late to prevent metastasis, recurrence and mortality. This has been brought into sharp focus by the SARS-CoV-2 global pandemic, constantly changing hospital policies and surgical guidelines in reducing access to established screening and treatment regimens. Nipple aspirate fluid (NAF), is thought to provide a unique window into the biological processes occurring within the breast, particularly in the context of a developing neoplasm. Evaluation of NAF in asymptomatic women, for novel chemical biomarkers of either early disease and/or cancer risk offers tremendous promise as a tool to facilitate early detection and to supplement screening. However, it is acceptability as a method of collection and screening by women is critical and yet unknown. A breast health questionnaire was disseminated to women through breast cancer charities, patient support groups and social media platforms, with the aim of collecting opinions on the acceptability of use of NAF as a potential screening tool.
Method Following ethical approval a questionnaire was prepared using online surveys consisting of four parts: (a) introduction on breast health screening in the UK, (b) core demographic data, (c) questions regarding screening and the acceptability of using NAF and (d) opinions about the process of collecting and using nipple fluid for screening. The voluntary and anonymous questionnaire was disseminated through social media, professional networks, charity websites and by individuals between October 2019 and December 2020. Survey responses were collected electronically, and the data analysed using online surveys statistical tools.
Results A total of 3178 women completed the questionnaire (65.9% Caucasian, 27.7% Asian/British Asian, 0.6% black and 5.0% other). Of these, 2650 women (83.4%) had no prior knowledge of NAF and 89.4% were unaware that NAF can be expressed in up to 90% of all women. Concerning their risk of breast cancer, 89.8% of women were keen to know their future risk of breast cancer, 8.5% were unsure whether they wanted to know their risk and a further, 1.6% did not want to know. Regarding screening, 944 women (29.8%) were unaware of the lack of routine National Health Service Breast Screening for those under the age of 47 years. Furthermore, 53.0% of women were unaware that mammographic screening is affected by breast density. In terms of the acceptability of home testing for breast health, 92.0% were keen to undergo a home test. Both 79.7% and 70.9% stated they would consider hand massage and a breast pump to acquire nipple fluid samples, respectively. A further 48.6% of women would consider the use of a hormonal nasal spray for the same purpose. However, with regards to acquiring results from NAF testing, 42.6% of women would prefer to receive results at home and 34.2% in a medical facility. Finally, 91.6% of women believed that breast health should be incorporated as part of school education curriculum.
Conclusion Public awareness regarding breast screening protocols and limitations of mammography could be improved. Many women were unaware that NAF might be a useful biofluid for future risk prediction, and yet the concept of self-testing of nipple fluid, with either hand massage or a breast pump was well received. Efforts should be made to increase awareness of the benefits of alternative and supplementary tests, especially in the context of high-risk individuals and younger patients.
- biomarker
- COVID-19
- mental health
- microbiome
Data availability statement
Data are available upon reasonable request. The authors are happy to share all data of individual participants with the BMJ if required.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
The concept of self-testing of nipple fluid, with either hand massage or a breast pump was well received by the majority of women.
Public awareness regarding breast screening protocols and limitations of mammography could be improved.
Efforts should be made to increase awareness of the benefits of alternative and supplementary tests, especially in the context of high-risk individuals and younger patients.
Introduction
The majority of the 55 000 new breast cancer cases in the UK each year derive from women deemed to be at low or average risk. However, women at high risk constitute ~6% of the female population between 40 and 75 years of age.1 A relative risk of 3–8, or higher, is defined as high risk and is associated with a plethora of features including significant family history of breast or ovarian cancers,2 very high breast density and those previously treated for breast and cancer with ≥1% risk of recurrence.3 While certain high-risk individuals may be identified from attending family genetic clinics, for the vast majority there is no mechanism to quantify breast cancer risk. This is critical, since identification of risk status facilitates adaptation of screening schedule intensity on the basis that early detection improves survival.4
In terms of current screening pathways, in addition to mammograms from the age of 47 years, those at higher risk are offered 12–18 monthly mammograms from the age of 40 years, and MRI screening, which has high sensitivity for breast cancer detection,5 but which is expensive, time consuming and has its contraindications.6 Similarly, the diagnostic accuracy of mammography is inferior in premenopausal women (eg, only 30%–48% sensitive).7 8 This is, in part due to high breast density.9 10 In addition, although able to detect breast cancer at an early stage, some lobular invasive cancers are notoriously occult on mammography, while other screen-detected cancers may have already metastasised at the time of diagnosis due to their aggressive nature.11 Moreover, ductal carcinoma in situ (DCIS) constitutes 20%–25% of all cases and if detected results in surgical excision often combined with radiotherapy. However, with such a small percentage of low-grade and intermediate-grade DCIS developing into an invasive carcinoma, overtreatment is a significant concern.7 12 Radiation exposure may also contribute to an increased incidence in breast cancer, particularly in high-risk populations, rendering mammography unsuitable for more frequent screening.7 12
Consequently, there is an unmet clinical need to provide high risk women with a safe, convenient breast health diagnostic and screening tools.13 Furthermore, in the midst of a SARS-CoV-2 global pandemic, with ever changing hospital policies and surgical guidelines,14 restrictions being placed on the number of diagnostic modalities offered to patients and the need to avoid unnecessary hospital admissions and surgical intervention—a single non-invasive, screening test to exclude breast carcinoma has become increasingly important and would pave the way towards proactive rather than reactive breast health management.
When considering novel screening tests, there has been a shift towards organ-specific biofluids.15–17 Exclusive to the breast, nipple aspirate fluid (NAF), is thought to provide a unique window into the biological processes occurring within the mammary ducts, particularly in the context of a developing neoplasm. Evaluation of NAF in asymptomatic women, for novel chemical biomarkers of disease offers tremendous promise as a tool to supplement screening and facilitate early detection, as well as the potential to offer a more tailored personalised risk profile.17 18 Early work has identified proteins,17 18 lipids,19 DNA promotor hypermethylation,20 hormones and tumour markers,21 as well as microbiome features22 that carry diagnostic potential. However, it is acceptability to women as a method of screening is unknown. In terms of the acquisition of NAF, over the years, a variety of methods have been used including: manual breast suction pumps, automated aspiration devices (similar to breast pumps for lactating women),23 nipple ductoscopy, ductal lavage24 and manual compression.25 These techniques carry success rates from 38% to 76%,26 27 increasing to up to 94% with oxytocin-assisted NAF collection.28 29
Aim
A breast health questionnaire was disseminated to women through breast cancer charities, patient support groups and social media platforms, with the aim of evaluating opinions on the acceptability of use of NAF as a potential screening tool.
Methods
The survey was prepared using online surveys (https://www.onlinesurveys.ac.uk/) and comprised four parts: (a) introduction on breast health screening in the UK; (b) core demographic data; (c) questions regarding screening and the acceptability of use of NAF and (d) opinions about the process of collecting and using nipple fluid for screening. Having read the background information, respondents were required to consent to participate in the survey. The inclusion criteria encompassed: being 18 years old or over, female, no known diagnosis of dementia and able to understand English. After consenting, respondents created a confidentiality code to protect their anonymity, before proceeding to complete the survey. No personal identifiable information was included to ensure privacy of patients.
The survey was launched in October 2019 and responses collected until December 2020 (https://bradford.onlinesurveys.ac.uk/breast-health-screening-uk). It was disseminated through social media (Facebook, Instagram, HealthUnlocked, Mumsnet), charity websites (CRUK, Breast Cancer Now), medical, cancer and professional networks (Bosom Friends, Soroptimists, British Society of Proteomics Research), institution newsletters (University of Bradford) and through correspondence of individuals. The social media platforms of doctors, professional groups and women were used to distribute the survey through all untargeted channels that encouraged participation of healthy women, along with patients with cancer in the past through the CRUK distribution mailing list and website.
Survey responses were electronically collated, processed and analysed using online survey statistical tools. Free text answers were subcategorised into themes and then grouped using Microsoft Excel (Excel 2019, V.16.30). Those respondents who did not consent were excluded from analysis.
Results
A total of 3178 completed the questionnaire with consent, providing a response rate of 74.0% (4305 respondents interacted with the survey to the point of creating a confidentiality code prior to commencing the survey). Of these, 65.9% were white, 27.7% Asian or British Asian and 5.0% other (undefined). Only 0.6% (19 respondents) were of black African, black American, black British or black Caribbean ethnicity while 0.8% preferred not to say (table 1). In terms of educational background, 2647 women (83.3%), had a higher degree, either in the form of a bachelor’s degree (41.6%), a master’s degree (16.6%), a professional degree (19.2%) or a doctorate degree (6.1%).
Demographics of patients, including: age, ethnicity, professional qualifications and relationship status
Regarding breast cancer risk, the vast majority of women (89.8%) were keen to know their risk, although a small proportion (8.5%) were unsure whether they wanted to know their risk and very few (1.6%) did not want to know (table 2). Free text responses revealed that most women wanted to know their risk because of a family history of breast cancer (29.2%), a personal history of breast cancer/previous breast disease (11.5%), or they were undecided between wanting to know their risk and concern that it would cause undue anxiety especially if there no acceptable treatment (4.3%) (table 3). Respondents who wanted to know did so in order to proactively managing their health, especially since they have known family members or friends who had breast cancer or died from it at a relatively early age (less than 60 years old). For those unsure, it was important for health services to have a support strategy in place should they find out they are at high risk. Those who said no, generally had no family history of breast cancer and therefore saw no reason for unnecessary alarm.
Summary of questionnaire answers, detailing overall response to non-free text questions
Summary of free text answers about whether women would want to know their risk of breast cancer, detailing common themes expressed
In terms of screening, 1954 women (61.7%) were aware of the lack of routine National Health Service Breast Screening for those under the age of 47 years, with 29.8% stating they were completely unaware. Furthermore, 53.0% of women were unaware that mammographic screening is affected by breast density, with further comments focusing on wanting to reduce the age of screening, drawing on personal experiences of their breast cancer diagnoses and comparisons to breast screening pathways in other countries (both good and bad). Many respondents who were aware of their breast density, were particularly enthusiastic for an alternative screening approach.
The majority of respondents (83.4%) were unaware of nipple fluid production in the breast other than for milk production, and consequently most were also oblivious to the fact that up to 90% of women can express NAF. Free text responses ranged from alarm to curiosity, with many requesting more information. A few commented on having expressed an infrequent discharge but as it did not persist, they ignored it. Many thought that expression of NAF might be restricted to those women who were pregnant (producing colostrum) or had breast fed and some comments reflected a concern that NAF expression might be uncomfortable or even painful.
In terms of the acceptability of home testing for breast health, 92.0% were keen to undergo a home test. Free text comments were subcategorised between the empowerment of a home-based test (citing convenience, flexibility, privacy, safety and timesaving when managing work and family commitments) versus trust in health professionals to do a better job (in clinic or general practitioner surgery). Some concerns were expressed regarding performing the test correctly, that it needs to be simple, provide an accurate diagnosis and be able to reflect the importance of the result in terms of next steps that is, further investigations, whether surgery was required, or whether the patient could indeed, be discharged. Many observed the benefits of a home test during the SARS-CoV-2 global pandemic rather than screening in a hospital.
79.7% and 70.9%, respectively stated they would consider hand massage and a breast pump to acquire nipple fluid samples, respectively, particularly if the respondent had successfully breast fed in the past. A further 48.6% of women would consider the use of a hormonal nasal spray for the same purpose. A negative response to the hormonal nasal spray approach from some respondents was based on the assumption that it was a steroid administration (whereas it is in fact a peptide, oxytocin, used to assist milk production in mothers with preterm babies) and that further steroid treatments (in addition to the pill and hormone replace therapy) would not be acceptable. However, with regards to acquiring results from home testing, 42.6% of women would prefer to receive results at home, 34.2% in a medical facility and 23.3% were undecided.
Finally, 91.6% of women believed that breast health should be incorporated as part of school education curriculum. Some of those respondents who felt it should not be included based their view on an already full curriculum.
Discussion
The results of this questionnaire illustrate that overall, a large majority of women (92%) would be keen to try an ‘at-home’ test, with 80% and 71% willing to trial either manual compression or a breast pump, respectively, to acquire a nipple fluid sample. From this, we demonstrate what appears to be a large shift in mindset following years of mammographic screening within the hospital setting. It can also be concluded that public awareness of at-home test has been raised by the SARS-CoV-2 crisis, whereby home-testing kits have been publicised and implemented successfully, with a turnaround time for 48 hours in some cases.30 Moreover, fear of attending a hospital for a non-urgent test during this time has been substantial.31 Other home-testing kits such as faecal occult blood testing32 for colorectal cancer and postal kits for sexually transmitted diseases (STDs) have helped this become the new norm for diagnostic as well as cancer screening tests.33 Although groups such as Suijkerbuijk et al,29 de Groot et al 34 and Proctor et al,27 have conducted questionnaires on patients enrolled in their studies evaluating NAF collection, to the author’s knowledge, this is the first questionnaire of its kind, seeking opinion on the acceptability of acquisition of NAF within the general untested population, focusing on the implementation of home-testing for breast health. Unsurprisingly, knowledge of NAF was limited, with 83% and 89% not having heard of NAF before or unaware that nipple fluid can be expressed in women. This was regardless of age, education or relationship status. Despite this, their willingness to try new methods of testing was significantly higher than those who were not interested, with 92% of women keen to both try this means of testing for breast health and improve baseline knowledge through the introduction of breast education into curriculums. From this, the conclusions drawn are threefold. First, women are concerned about their risk of developing breast cancer and are willing to go above and beyond current means to reassure themselves. Second, women are aware of the gaps in their own knowledge and understanding and third, there is a desire to change this for future generations.
While exploring the demographic of those who responded to the questionnaire, it was interesting to note that 85.8% of respondents were aged between 21 and 40 years. This reflects the currently ‘unscreened’ population of women. Targeting this cohort of women was considered a strength as it reflects the opinions of future service users, rather than only those who are considering their experience of screening retrospectively, which can carry bias for a number of reasons including personal history of breast disease, family history of breast cancer and of course, their past experience of screening. In addition, 28% of women who completed the questionnaire were of either an Asian or British Asian background. This is disproportionately high compared with the 8% represented within the UK population, and contradicts the engagement barriers often encountered with breast screening services within these communities.35 Reasons for high engagement may include: a higher distribution by word-of-mouth through these communities; marketing within doctors’ groups on social media, with a larger percentage of Asian followers/subscribers, an ability to express their views anonymously through the survey and an increasing desire to self-educate as the incidence of more aggressive subtypes of breast cancer perpetuate within ethnic minority groups in the western world.36 Moreover, engagement from these communities in this way demonstrates that the use of social media may enable clinical researchers to connect with populations that have been historically difficult to study.35 Another important point to note is that only 8% of respondents were aged 41–50 years. This age group includes current screening users, particularly in high-risk groups and it would have been interesting to equally compare differences in opinions between this group and the younger cohort. Screening guidelines for this group differ internationally and therefore future questionnaires would seek to target this group of women to explore their ideas about screening for breast health.
In terms of the response rate, we documented that the number of people who progressed to the point of creating a confidentiality page on the questionnaire, compared with those who went on to complete it, was 74%. An important consideration is that there is no agreed methodology for calculating response rates in questionnaires which have been distributed on social media platforms. This is because, for example, a link to the study posted on a person’s account, may then be shared by another person, leading to an exponential and incalculable rise in the number of viewers, making the denominator impossible to calculate. However, validity can be assumed from the large absolute number of responses from the survey. It is rare for surveys of this nature to attract so many responses, with a recent meta-analysis demonstrating that the average response rate in web-based patient-studies is 59.3%.37 This potential limitation is therefore also one of the greatest strengths of the questionnaire and signifies a change in the way we look at public engagement.
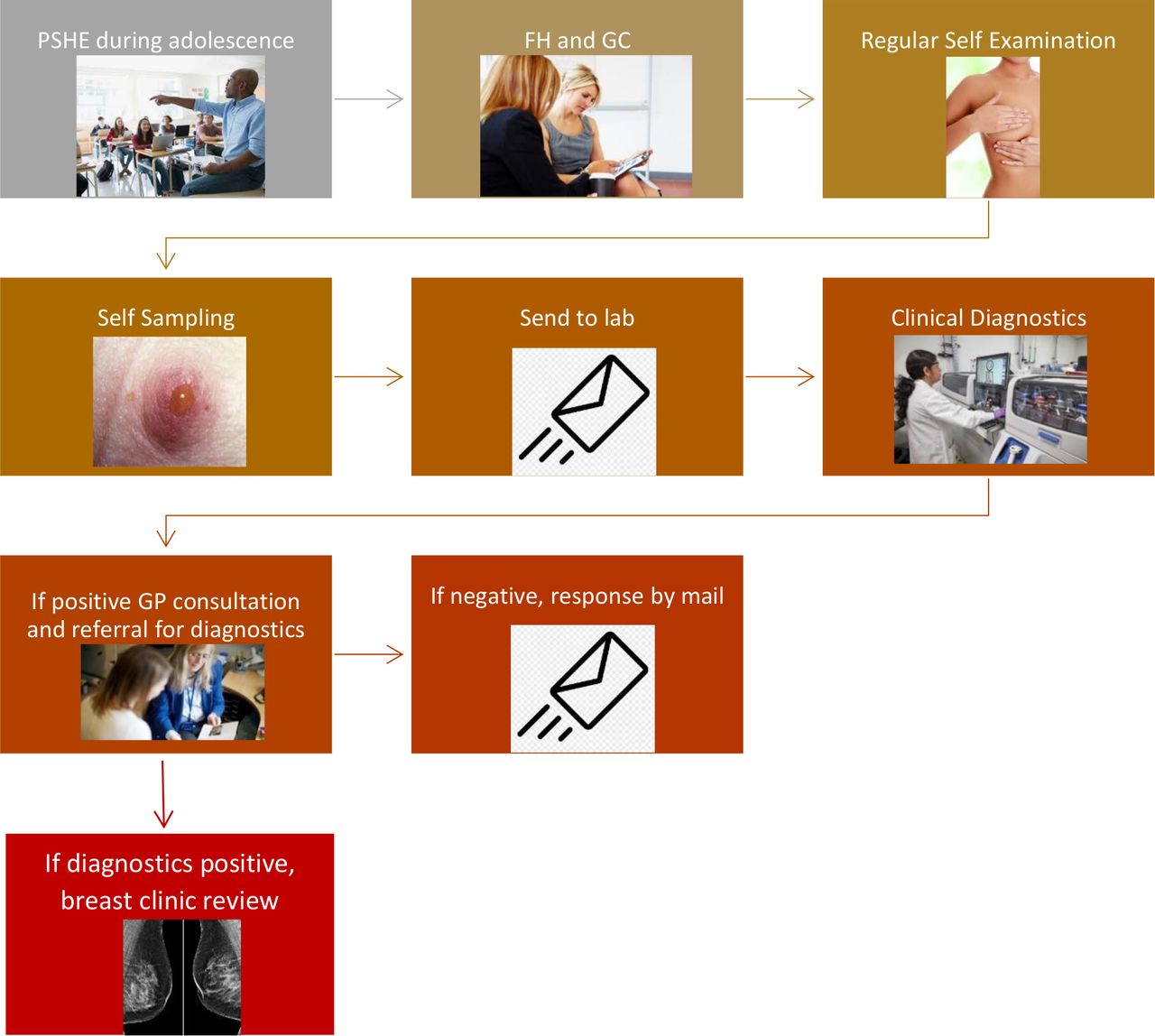
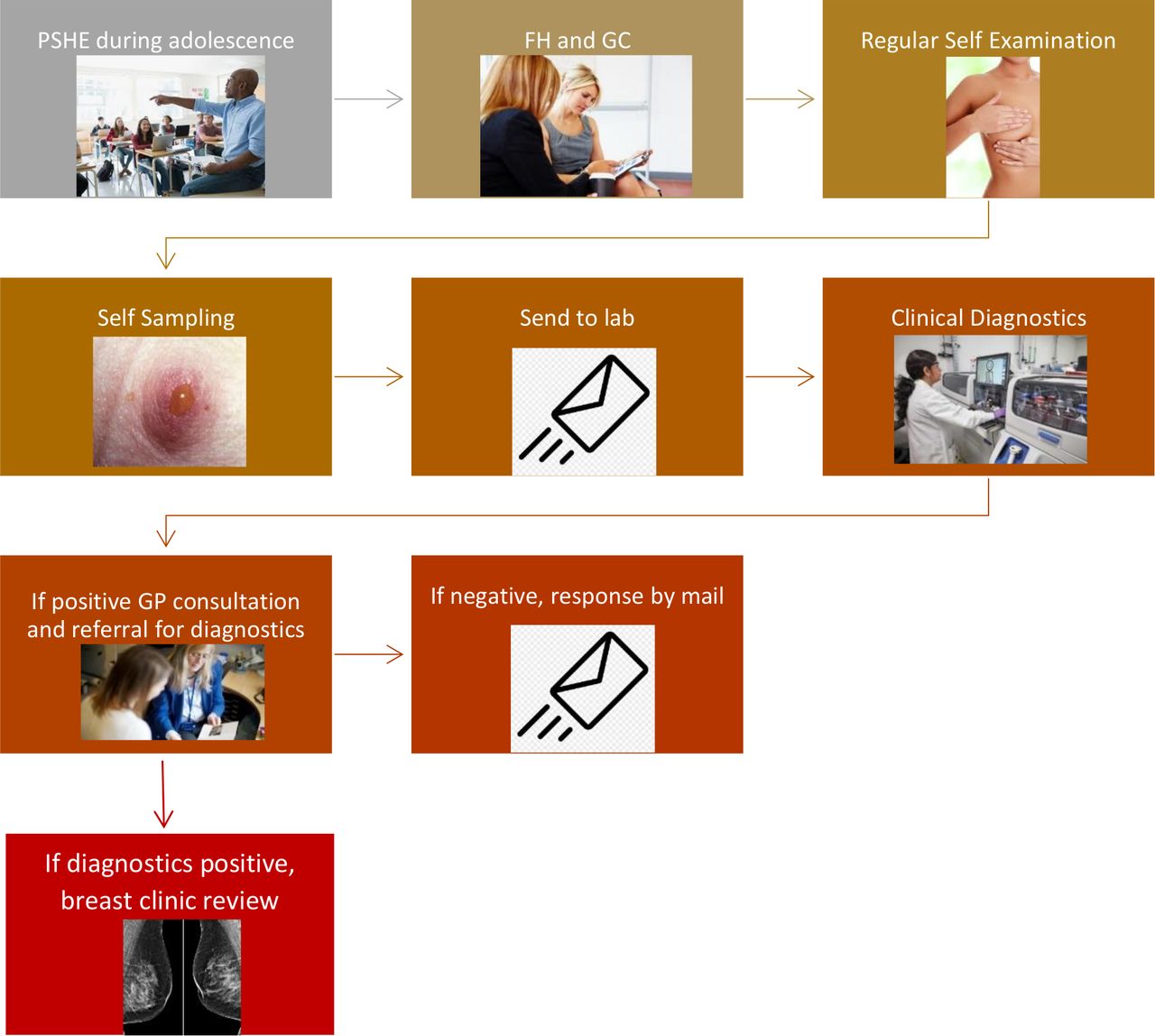
Another key finding was the willingness of participants to improve public knowledge of breast cancer and self-examination through school education (91.6%). Free text answers echoed this, with 12.4% reiterating that education should be for both sexes. This finding reflects the increasing interest in breast health awareness in general, especially when compared with similar diseases such as cervical cancer, vaccinations, STDs and so on. With this in mind, we have suggested a potential pathway for breast education, self-examination and NAF screening, based on responses from the questionnaire (figure 1).
{kind=link}
Summary of pathway for management of breast screening with nipple aspirate fluid. FH, family history; GC, genetic counselling; GP, general practitioner; PSHE, physical and sexual health education.
Conclusion
This questionnaire highlights that the concept of self-testing of nipple fluid, with either hand massage or a breast pump, is well received. Public awareness regarding breast screening protocols and limitations of mammography could be improved, with many women understandably unaware that analysis of nipple fluid might be useful for future risk prediction. The use of social media for public engagement creates endless possibilities for similar research in the future. Efforts should be made to increase awareness of the benefits of alternative and supplementary tests, especially in the context of high-risk individuals and younger patients. Consequently, there is a case to initiate a programme of research to determine the diagnostic value of NAF for the early detection of breast cancer in women at highest risk. Future work would need to further explore the themes identified within this questionnaire in the form of patient interviews. Opinions on methods of collection of nipple fluid, as well as how best to disseminate patient education and improve public awareness across all demographics is the key to improving pathways for breast cancer screening in the years to come.
Supplemental material
Data availability statement
Data are available upon reasonable request. The authors are happy to share all data of individual participants with the BMJ if required.
Ethics statements
Ethics approval
The questionnaire protocol was subject to ethical and institutional review at the University of Bradford (Ethical Approval ID: E744). The questions were also reviewed by the Patient and Public Involvement (PPI) Team at Imperial College London, who gave feedback on the nature of the questions, use of language and appropriateness.
Acknowledgments
The authors would like to thank Dr Valerie Lesk, University of Bradford for her expertise in survey design. A special appreciation to CRUK, Breast Cancer Now, Bosom Friends and many individuals who circulated the survey link including Dr Stephanie Patel, Dr Zena Willsmore and Dr Amalina Che Bakhri. Most importantly we are grateful to all the respondents for their participation in the survey, the very useful feedback and personal stories that provide the motivation to find a new way to support women at risk of breast cancer.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @natasha_jiwa
Contributors NJ: disseminated the questionnaire, cleaned and analysed the data and prepared the draft and revised manuscript. As the guarantor, NJ accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. ZT: prepared the manuscript and provided a supervisory role. DRL: Prepared the draft and revised iterations of the manuscript. He also provided a supervisory role. CS: responsible for overall design, acquired ethical approval, designed and disseminated the questionnaire. He cleaned and analysed the data and prepared the draft and revised iterations of the manuscript. He was overall lead supervisor of project.
Funding The research was funded by the NIHR Imperial Biomedical Research Centre (BRC). Health Technology Assessment Programme.
Disclaimer The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Competing interests All authors have completed the Unified Competing Interest form and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed by Cathy B Moelans, UMC Utrecht, the Netherlands and Dr Emmanuel Baah, University of North Carolina System.