Article Text

Abstract
Introduction The majority of Indian women have a poor dietary folate and vitamin B12 intake resulting in their chronically low vitamin status, which contributes to anaemia and the high incidence of folate-responsive neural-tube defects (NTDs) in India. Although many countries have successfully deployed centrally-processed folate-fortified flour for prevention of NTDs, inherent logistical problems preclude widespread implementation of this strategy in India. Because tea—the second most common beverage worldwide (after water)—is consumed by most Indians every day, and appeared an ideal vehicle for fortification with folate and vitamin B12, we determined if daily consumption of vitamin-fortified tea for 2 months could benefit young women of childbearing-age in Sangli, India.
Methods Women (average age=20±2 SD) used teabags spiked with therapeutic doses of 1 mg folate plus either 0.1 mg vitamin B12 (Group-1, n=19) or 0.5 mg vitamin B12 (Group-2, n=19), or mock-fortified teabags (Group-0, n=5) to prepare a cup of tea every day for 2 months, following which their pre-intervention and post-intervention serum vitamin and haemoglobin concentrations were compared.
Results Most women had baseline anaemia with low-normal serum folate and below-normal serum vitamin B12 levels. After 2 months, women in both Group-1 and Group-2 exhibited significant increases in mean differences in pre-intervention versus post-intervention serum folate levels of 8.37 ng/mL (95% CIs 5.69 to 11.04, p<0.05) and 6.69 ng/mL (95% CI 3.93 to 9.44, p<0.05), respectively; however, Group-0 experienced an insignificant rise of 1.26 ng/mL (95% CI –4.08 to 0.16). In addition, over one-half and two-thirds of women in Group-1 and Group-2, respectively, exhibited increases in serum vitamin B12 levels over 300 pg/mL. There was also a significant post-interventional increase in the mean haemoglobin concentration in Group-1 of 1.45 g/dL (95% CI 0.64 to 2.26, p=0.002) and Group-2 of 0.79 g/dL (95% CI 0.11 to 1.42, p=0.027), which reflected a bona fide clinical response.
Conclusion Tea is an outstanding scalable vehicle for fortification with folate and vitamin B12 in India, and has potential to help eliminate haematological and neurological complications arising from inadequate dietary consumption or absorption of folate and vitamin B12.
- birth defects
- malnutrition
- mental health
- nutrient deficiencies
- nutritional treatment
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
Although many countries have successfully deployed centrally-processed folate-fortified flour for prevention of neural-tube defects, several inherent logistical problems preclude widespread implementation of this strategy in India. This is an important issue to resolve because Indian women of childbearing age, who have a poor dietary intake of both folate and vitamin B12 and low-vitamin status, uniformly prefer food-based vitamin supplements.
We posited that a single daily cup of tea, which is consumed by most Indians, has outstanding characteristics as an actionable and scalable vehicle for fortification with these water-soluble vitamins.
Accordingly, under the aegis of a therapeutic care protocol for women of childbearing age in Sangli, India, we exploited folate-spiked and vitamin B12-spiked teabags as Trojan Horses to deliver therapeutic doses of these vitamins into their daily cup of tea over 2 months. This led to significant rises in their serum folate, serum vitamin B12 and haemoglobin concentration.
Although additional research is needed, these preliminary data suggest that eventual adoption of large-scale fortification of tea with folate-and-vitamin B12 in India has real potential to eliminate haematological and neurological complications arising from inadequate dietary consumption or absorption of folate and/or vitamin B12 in all stages of life.
Introduction
Most women of childbearing-age in India consume a poorly balanced diet that leads to a chronically low folate-and-vitamin B12 status.1–8 An equally disturbing finding is that (for a variety of reasons) up to 90% of the world’s women (who reside primarily in resource-limited countries) do not receive sufficient dietary folate.4 9 This is a particularly serious issue, given the compelling evidence of a causal relationship between periconceptional low-folate status and an increased risk in the incidence of folate-responsive (folate-preventable) neural-tube defects (NTDs).1 Conversely, periconceptional folate supplementation has consistently reduced the risk of both first occurrence and recurrence of NTDs by over 70%.10–14 These studies have informed recommendations for dietary guidelines and fortification of flour with folic acid,15 led to markedly improved serum folate concentrations in populations receiving folate-fortified flour,16 and substantially reduced first-occurrence of NTDs.17–21 Globally over 80 countries mandate folate-fortification of industrially-milled cereal grain.22
Despite the documented success of folate-fortification of flour for two decades,1 17 this rosy picture masks three significant inter-related issues which have remained perpetually vexing problems in India that warrants highlighting and begs an urgent solution:
(1) There are inherent limitations related to the equitable distribution of folate-fortified flour throughout India. In general, successful implementation of such a programme necessitates the process of folate-fortification of flour be carried out centrally in large roller-mills for milling cereal, from where it can be widely distributed to reach populations living in the smallest towns, villages and hamlets throughout India. This poses significant logistical challenges within the Indian context where approximately 70% of the population live in over 650 000 villages, cereal grain is more often grown and purchased locally, and flour is prepared by small-scale millers in these villages; this effectively bypasses any need for centrally-processed fortified flour. This fact predicts that India is unlikely to achieve a robust folate-food fortification programme solely using flour, and opens the door to identification of alternate food vehicles that are contextually-appropriate for fortification.
(2) There is a high incidence of nutritional vitamin B12deficiency (estimated in three-quarters of the population)6 among vegetarians and non-vegetarians in India who usually subsist on a ‘near-vegetarian’ diet.1 2 4 5 23 In the city of Pune, in Maharashtra (the second largest state of India: population 114 million), vitamin B12 deficiency is documented in two-thirds of non-pregnant women,24 as well as pregnant rural women,8 but in Haryana it was found in 74%.25 Therefore, without also replenishing deficient vitamin B12, consumption of supplemental folate alone through folate-fortified flour will not be adequately used by tissues because the key intracellular enzyme, methionine synthase, depends on the presence of vitamin B12 as a co-factor to sustain intracellular one-carbon metabolism.1
(3) The consequence of these nutritional deficiencies have an extremely serious impact on the incidence of severe but preventable birth defects. Our population-based study on NTDs carried out in the least-developed area of India (Balrampur District, Uttar Pradesh) in 2005, identified up to 8.2-affected babies with NTD per 1000 live births,26 which is among the highest in the world. A decade later, another population-based study modelled after ours in the same State (Uttar Pradesh), confirmed a persistently high incidence of NTD (up to 7.48-cases per 1000 live births).27 Thus, there has been no progress in NTD-prevention in this most populous state of India of ~200 million. A systematic review of all studies in India primarily from tertiary referral centres (which do not capture as many NTDs as population-based studies) revealed a more conservative prevalence of 4.1-cases of NTDs per 1000 live births.28 Given the approximately 26 million births annually in India, this is still an unacceptably large burden of folate-preventable NTDs in India,26–31 particularly since it is estimated that up to 90% of these birth defects can be prevented by improvement in the folate (and vitamin B12) status of women in India.32 It is estimated that a robust programme in India that optimises the periconceptional (folate and vitamin B12) nutrition of Indian women can avoid the tragedy of 115 000 babies being born with NTD every year.32
We have also determined that despite knowledge of their low dietary intake of folate and vitamin B12 and potential adverse risks to the well-being of their future progeny, most young Indian women attending undergraduate college expressed staunch resistance to taking daily supplements of vitamins in tablet form; however, they were open to consumption of a fortified staple food that is a part of their daily diet (see online supplemental material).
Supplemental material
Based on these considerations, we posited that tea meets criteria33 as an ideal, contextually-appropriate, food vehicle for full therapeutic replenishment with folate and vitamin B12 (and by implication, for fortification) in India for several reasons: Besides water, tea is the most common beverage in India (and worldwide),34 and is largely grown and processed in the highlands of only 4 (out of 28) states of India—Assam, West Bengal, Tamil Nadu and Kerala. Moreover the vast majority of adult Indians from every geographical area within India—from megacities to the smallest towns, villages and hamlets—consume at least one cup of tea from one of these regions every day; thus, tea retains a unique role by being a common ‘food’ that rises above the otherwise extremely diverse food preferences of Indians.5
There has been no previous documentation of the feasibility of using tea as a vehicle for delivery of therapeutic doses of folate and vitamin B12 in humans. Accordingly, we embarked on a preliminary study to assess the feasibility of using vitamin-fortified teabags as a means to deliver full therapeutic replacement doses of pure folate and vitamin B12 in a daily cup of tea over 2 months to Indian women of childbearing age in a region of the state of Maharashtra where most young women have a low folate and vitamin B12 status. The efficacy of using tea prepared from vitamin-fortified teabags in this population was assessed primarily by focusing on whether there were significant changes in each individual woman’s pre-intervention versus post-intervention serum folate and vitamin B12 levels and haemoglobin.
Methods
Strategy and study design
As the first study to use tea as a vehicle for the delivery of folate and vitamin B12 into humans, some issues that justify this strategy warrant consideration. Earlier studies from Pune, India, suggested that a significant majority of the population of women of childbearing age had low folate and vitamin B12 status that was likely due to inadequate dietary intake3–6; because they could efficiently absorb physiological oral doses of vitamin B12,24 35 this ruled out any defects in absorption. Although it was reasonable to infer that women in Sangli (120 miles away) would have similarly low vitamin status, this was formally assessed in a population of 60 women (nursing students) in Sangli (see online supplemental figure S1). These data revealed that the overwhelming majority of women in this region (who usually consume a daily cup of tea) had evidence of a combined low folate and vitamin B12 status.
Preliminary studies (see online supplemental material) revealed that therapeutic doses of both United States Pharmacopeia (USP)-grade oral preparations of vitamin B12 and folate, which are usually swallowed using water, are easily water-soluble, and do not impart any taste when dissolved in water. So, we reasoned there would be equivalence in delivery of daily therapeutic doses of both USP-grade vitamins to women by either directly dissolving therapeutic doses of these vitamins in water during the brewing of tea, or spiking teabags with full daily therapeutic doses of these vitamins prior to the brewing of hot tea.
Therefore, the aim of this preliminary study in a cohort of young women with low-vitamin status was to assess the acceptability, feasibility and efficacy of exploiting folate-spiked and vitamin B12-spiked teabags as a vehicle to deliver therapeutic doses of these vitamins into a daily cup of tea over 2 months to improve their serum vitamin levels. The acquisition of encouraging preliminary data on the efficacy of this strategy would lay the groundwork for subsequent confirmation of the effectiveness of vitamin-fortified tea in women with low-vitamin status through formal randomised controlled trials.36 Such an approach had the potential to scale up and establish tea as an ideal contextually-appropriate vehicle for fortification with folate and vitamin B12 in India.
With regard to the dose of folate and vitamin B12 to be added to each teabag, clinical trials have demonstrated that oral vitamin B12 consumption of 0.1 mg37 and 0.5 mg24 are apparently equally efficacious24 37 and can improve serum vitamin B12 levels among those with vitamin B12 deficiency within 6 weeks, whereas 0.5 mg and 1 mg vitamin B12 can reverse food-vitamin B12 malabsorption within 4 months.24 38 39 In addition, subjects with folate deficiency rapidly respond to daily oral doses of 1 mg folic acid.1 Therefore, we assumed most subjects would respond to the consumption of a daily cup of tea using teabags—(fortified with 1 mg folate plus either 0.1 mg37 or 0.5 mg24 vitamin B12 for 2 months)—by normalisation of their vitamin status.1 4 5 40
Because this was the very first exploration on therapeutic repletion of low vitamin status in humans using this strategy, we did not have any guidelines on the sample size to be used. We limited the number of control subjects based on the following reasoning: The finding of a high prevalence of low folate and vitamin B12 status among young women in Sangli (online supplemental figure S1) allowed for the inference that any available folate and vitamin B12 in their daily cups of (unfortified) tea could not meaningfully increase the serum folate and vitamin B12 over 2 months in a control group of women consuming (unfortified) tea. Hence, we could not justify inclusion of an equivalent number of control subjects as those in the experimental arm of the study (who would be administered full therapeutic replacement doses of folate and vitamin B12 daily through vitamin-fortified tea). Accordingly, we primarily focused on comparison of each subject’s pre-intervention serum levels with her post-intervention serum levels as the initial measure of efficacy, whereas group-wise comparisons between the experimental and control subjects would necessarily be limited by the smaller number of women assigned to the control group.
Recruitment of subjects
Women recruited for the teabag intervention study were from the RR Patil College of Nursing Education and College of Homeopathy, Sangli. Inclusion criteria for entry into the trial were women between 18–25 years with no medical history of illness in the past 6 months. Each participant would necessarily agree to consume a daily cup of tea using their uniquely assigned teabags for 2 months everyday (from Monday to Saturday in the college cafeteria, and on Sunday in their homes). Exclusion criteria included existing pregnancy or planning pregnancy, use of iron, folate or vitamin B12 or other multivitamins in the previous 6 months or during the 2 months of the trial, and any other chronic medical illness, or fever, or diarrhoea in the prior 3 months. These studies were initiated and completed in 2019 before the COVID-19 outbreak reached India.
Informed consent
Two authors (RMV and ACA) delivered a lecture for women who were potential candidates for entry into the teabag intervention study: This lecture highlighted the problem of dietary folate deficiency and vitamin B12 deficiency in India; the consequences for adverse pregnancy outcomes of women who were folate-deficient and/or vitamin B12-deficient; and the general plan of the study. Ample time was allotted for answering questions. Those women expressing an interest in this study were provided with informed consent forms, which highlighted details of the study. These informed consent forms contained specific assurance that we would administer full doses of vitamin replacement (1 mg tablets of vitamin B12 and folate daily for 2 months) to the group assigned mock-fortified teabags, as well as for any other women using vitamin-spiked teabags who had suboptimal serum vitamin responses. All women were requested to carefully read and discuss the study with their family for at least 1 week before agreeing to sign consent to enter the study. The college leaders were separately encouraged to emphasise to students that entry into the study was entirely voluntary, and there was to be no coercion, as was emphasised in the informed consent form.
Fortification of teabags containing Indian tea (Camellia sinensis) with folate and vitamin B12
Preliminary observations on the dissolution of the vitamins, appearance and organoleptic assessment of vitamins dissolved in brewed tea are described in online supplemental material. The exposure of vitamins to heat following brewing of tea involved teabags being steeped in approximately 95°C hot water (75–100 mL) for 2–5 min before addition of room temperature milk and sugar; this extent of heat exposure is far less than that involved in baking vitamin-fortified bread, where the majority of both vitamins were stable and functionally capable of raising blood vitamin levels among healthy adults.41 Fortification of teabags was carried out in a darkened room, with windows covered by dark coloured cloth to avoid ultraviolet light induced photodegradation of folic acid42 and vitamin B12.43
Each teabag was spiked with pharmacological doses of folate (1 mg folate) plus either of two equally efficacious24 37 doses of vitamin B12 (0.1 mg or 0.5 mg, respectively) that were precisely applied onto each teabag for two equal cohorts of women of childbearing-age in Sangli (n=19). As reasoned above (Strategy and Study Design), we also planned to randomly assign a much smaller cohort of women (n=5) to simultaneously receive mock-fortified teabags for 2 months to assess for any changes in serum vitamin levels to unfortified tea; after the 2-month trial, this group would then be given an additional 2 months of full vitamin replacement tablets (ie, with a 2-month delay compared with the other groups).
We used commercially available teabags, each composed of a filter paper bag containing 2 g Brooke Bond Taj Mahal tea—an orange pekoe blend of black tea with characteristic dark-red brew, a strong malty flavour and full body. Both folic acid and vitamin B12 used to fortify tea were of USP-grade and obtained from Sigma-Aldrich (USA); this was in keeping with Food Safety and Standards Authority of India (FSSAI) regulations44 on the use of USP-grade vitamins for medical use in humans.
Applying precise amounts of dissolved solutions of vitamin B12 (red colour) and folate (yellow colour) using an Eppendorf pipette left a small coloured stain on each teabag in Group-1 and Group-2. For mock-fortified teabags for controls (Group-0), we used two US Food and Drug Administration-approved food colouring agents, Chefmaster Liqua-Gel Food Golden-Yellow and Super-Red colours (Byrnes & Kiefer Company, Fullerton, California). Diluting 5 mL of stock Golden-Yellow and Super-Red into 50 mL water perfectly matched the colour of stock solutions of folate and vitamin B12, respectively. Thus, women in Group-0 used teabags spiked with 25 µL each of Super-Red plus Golden-Yellow food colouring; women in Group-1 used teabags spiked with 0.1 mg (5 µL) vitamin B12 plus 1 mg (50 µL) folate; and women in Group-2 used teabags spiked with 0.5 mg (25 µL) vitamin B12 plus 1 mg (50 µL) folate. After addition of vitamin B12 and folate (or food colouring) to teabags, they were gently dried using a hair dryer and repacked in original boxes, now specifically coded for Group-0, Group-1 and Group-2.
Logistics of tea delivery and consumption
After informed consent was obtained, women were randomly assigned using a lottery format to either receive mock-fortified tea in Group-0 (n=5), or to fixed doses of folate in Group-1 and Group-2, with increasing doses of vitamin B12-fortified tea in Group-1 (n=19) and Group-2 (n=19), respectively. Confirmation that the teabags were correctly distributed to each of the participants in the three Groups was verified by the investigators. Women were blinded as to which Group they were assigned. A blood sample was obtained for measurement of baseline pre-intervention serum folate, serum vitamin B12, and haemoglobin. Women kept their Group-assigned teabags in lockers at the college. During each mid-morning ‘tea-break’ (Monday through Saturday), they were provided with a near-boiling cup of hot water (75–100 mL) into which they dunked their assigned teabags for 2–3 min after which milk and sugar was added to taste. Women took one of their assigned teabags home for their Sunday mid-morning tea. Compliance was maintained by two class monitors who observed the subjects drinking tea every day in college and kept a daily ‘tea attendance record’. At the end of 2 months of daily use of trial teabags, a repeat post-intervention blood sample was taken for serum folate, serum vitamin B12 and haemoglobin for comparison with the pre-intervention values.
Following the study, all women with persistently low serum folate and/or serum vitamin B12 levels in post-intervention blood samples were provided tablets containing 1 mg folic acid and 1 mg vitamin B12 and advised to take them daily for 2 months.
Blood tests
Venous blood for haemoglobin and vitamin determination was drawn from each woman between 1–2 days before the intervention with vitamin-fortified or mock-fortified teabags from the Ghatage Hospital Laboratory; these were the pre-intervention blood samples. Of 5 mL blood drawn from each woman, 1 mL was for sent for a complete blood count at the Ghodawat Diagnostic Center, Sangli, and the remainder processed for measurement of serum folate and vitamin B12. Briefly, following separation of serum within 1 hour of blood collection, samples were transported chilled in ice-packs to Mumbai by courier where serum folate and vitamin B12 levels were measured at Metropolis Laboratory, Mumbai, within 1 day of receipt, using a chemiluminescence immunoassay. A second blood sample was drawn within 2 days after completion of the intervention with teabags from all women. A portion of this post-intervention sample was again sent for a complete blood count, and the remainder was similarly processed, transported and analysed for serum folate and vitamin B12 by Metropolis Laboratory, Mumbai, as described above. Normal values for serum folate from this laboratory was 3–17 ng/mL; the reference range for normal serum vitamin B12 was between 187–883 pg/mL. The coefficient of variation for folate assays was 8.7% and for vitamin B12 was 7.7%.
Statistics
Analyses of variance were used to evaluate between-group mean differences in levels of pre-intervention versus post-intervention serum folate, serum vitamin B12 and haemoglobin. Paired t-tests were used to evaluate within-group differences. Non-normally distributed data were evaluated using the non-parametric Kruskal-Wallis and Wilcoxon signed-rank tests. To account for multiple comparisons (eg, involving all three Groups), we used a conservative alpha of 0.02 (0.05/3). For within-group comparisons and comparisons between two groups, we used an alpha of 0.05. All statistics were conducted using IBM SPSS Statistics V.25.
Role of funding source
Neither the Manavrahat Charitable Trust nor any other institution or individual had any role in the study design, data collection, data analysis, data interpretation, in writing of the report or in decision to submit the paper for publication.
Results
Low folate and vitamin B12 status is common among young women in Sangli
Studies on a group of 60 women (average age=22±3 SD) who were nursing students at the Kulloli Institute of Nursing Sciences in Sangli (see online supplemental figure S1) revealed that 95% had evidence for low-folate status (with 80% having below-normal serum folate values, consistent with frank folate deficiency). In addition, 63% of these women also had low-vitamin B12 status (with 23% having frank vitamin B12 deficiency, based on below-normal serum levels). Therefore, women of childbearing-age in Sangli also exhibited a low-folate and low-vitamin B12 status, similar to that reported in Pune,8 24 which reflected their uniformly inadequate dietary intake of these vitamins. This justified preliminary studies to develop a therapeutic care protocol designed to reverse low-vitamin stores among a comparable cohort of women in Sangli, with an ultimate goal to scale up studies to benefit millions of women with low-folate and low-vitamin B12 status throughout India.
Organoleptic features of brewed tea using vitamin-fortified teabags
Preliminary data on the dissolution of vitamins in water, camouflage of vitamins in tea and organoleptic assessment of vitamins dissolved in brewed tea are described in the o nline supplemental material. The consumption of tea prepared from teabags fortified with folate and vitamin B12 (Group-1 and Group-2) compared with mock-fortified teabags (Group-0) precluded subjects from discerning which Group they belonged to; this extended to their inability to discern differences between vitamin-fortified and unfortified tea, since neither the inclusion of pure vitamin B12, nor folate, nor the infusion of colouring in the amber-reddish brewed tea imparted any changes to the original high quality, unique flavour, and aroma of this brand of tea—so its unique ‘terroir’ was retained. Over 90% of women adhered to the protocol and none modified their regular diet during the trial.
Basal values and responses to folate-fortified tea
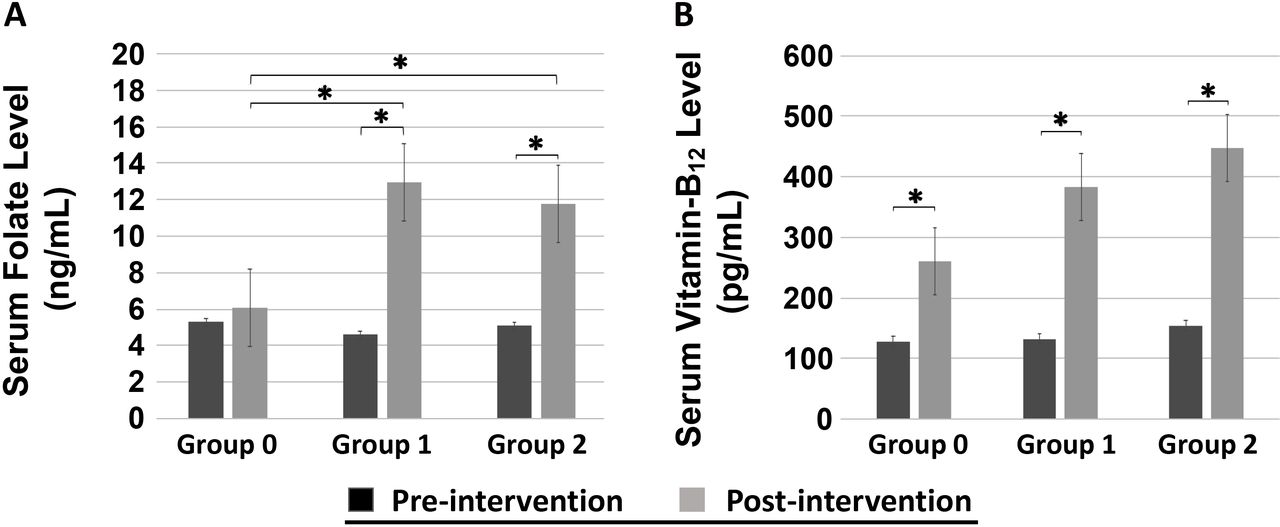
When baseline values for serum folate were examined (figure 1A), women in Group-0 (n=5, average age=20±1 SD), Group-1 (n=19, average age=20±2 SD) and Group-2 (n=19, average age=20±1 SD), had mean serum folate levels of 5.3, 4.6 and 5.5 ng/mL, respectively; (normal serum folate is 3–17 ng/mL (Metropolis Laboratory)). Thus, there were no differences in pre-intervention mean serum folate levels for subjects in any of the three Groups. A small minority of women had serum folate levels that were frankly below normal—0 among 5 in Group-0, 4 of 17 in Group-1 (2 blood samples were lost), and 2 of 19 in Group-2.
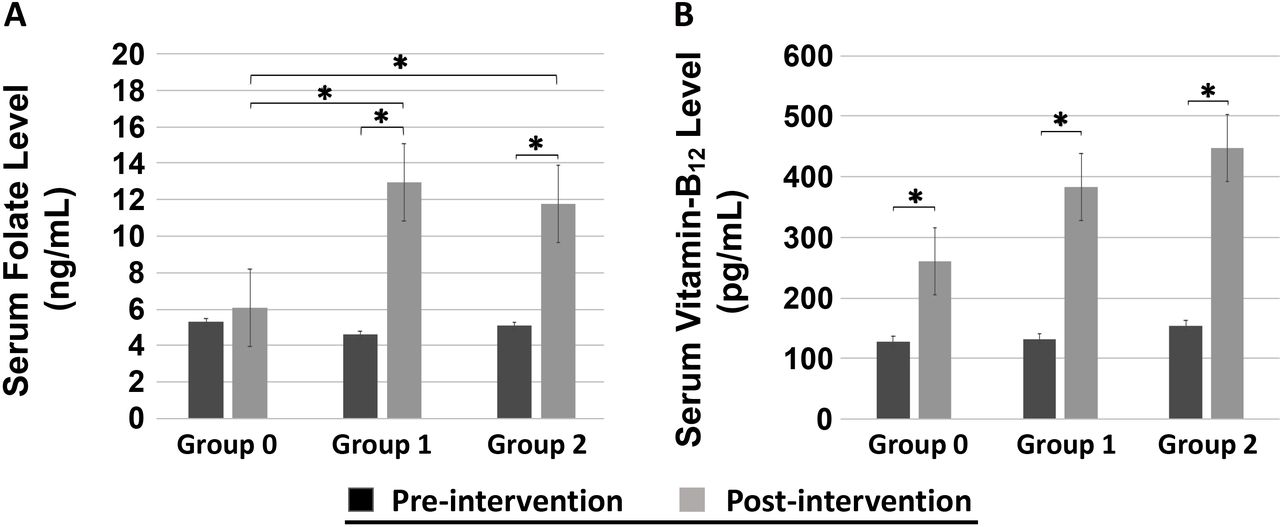
Comparison of mean serum folate levels (A) and serum vitamin B12 levels (B) in various groups of women at baseline (pre-intervention) (dark shaded bars) and after 2 months (post-intervention) (light shaded bars) consumption of a daily cup of tea using either mock-fortified teabags (Group-0, n=5, (average age=20±1 SD)), or folate-fortified and vitamin B12-fortified teabags (Group-1, n=19, (average age=20±2 SD) containing 0.1 mg vitamin B12 plus 1 mg folate per cup) or (Group-2, n=19, (average age=20±1 SD) containing 0.5 mg vitamin B12 plus 1 mg folate per cup). Data is shown as mean±SE. The asterisks signify a statistically significant difference (p<0.05) in the pre-intervention versus post-intervention serum folate or serum vitamin B12 levels between-Groups and within-Groups indicated.
However, in response to intervention with daily mock-fortified tea (Group-0) or daily 1 mg of folate-fortified tea (Group-1 and Group-2) for 2 months, there were important results in serum folate levels both within-Groups and between-Groups (figure 1A). Thus, for Group-0, the mean difference in pre-intervention versus post-intervention serum folate level was only 1.26 ng/mL (95% CIs –4.08 to 0.16), indicating no statistical differences. By contrast, the mean difference in pre-intervention versus post-intervention serum folate level for Group-1 was 8.37 ng/mL (95% CI 5.69 to 11.04), and Group-2 was 6.69 ng/mL (95% CI 3.93 to 9.44), indicating a statistically significant difference (p<0.001) within both Group-1 and Group-2. In addition, between-Group comparisons of Group-0 and Group-1 also indicated a statistically significant mean difference in post-intervention serum folate level in response to daily folate-fortified tea consumption (p=0.02). Not surprisingly, there were no differences between post-intervention serum folate levels in Group-1 and Group-2.
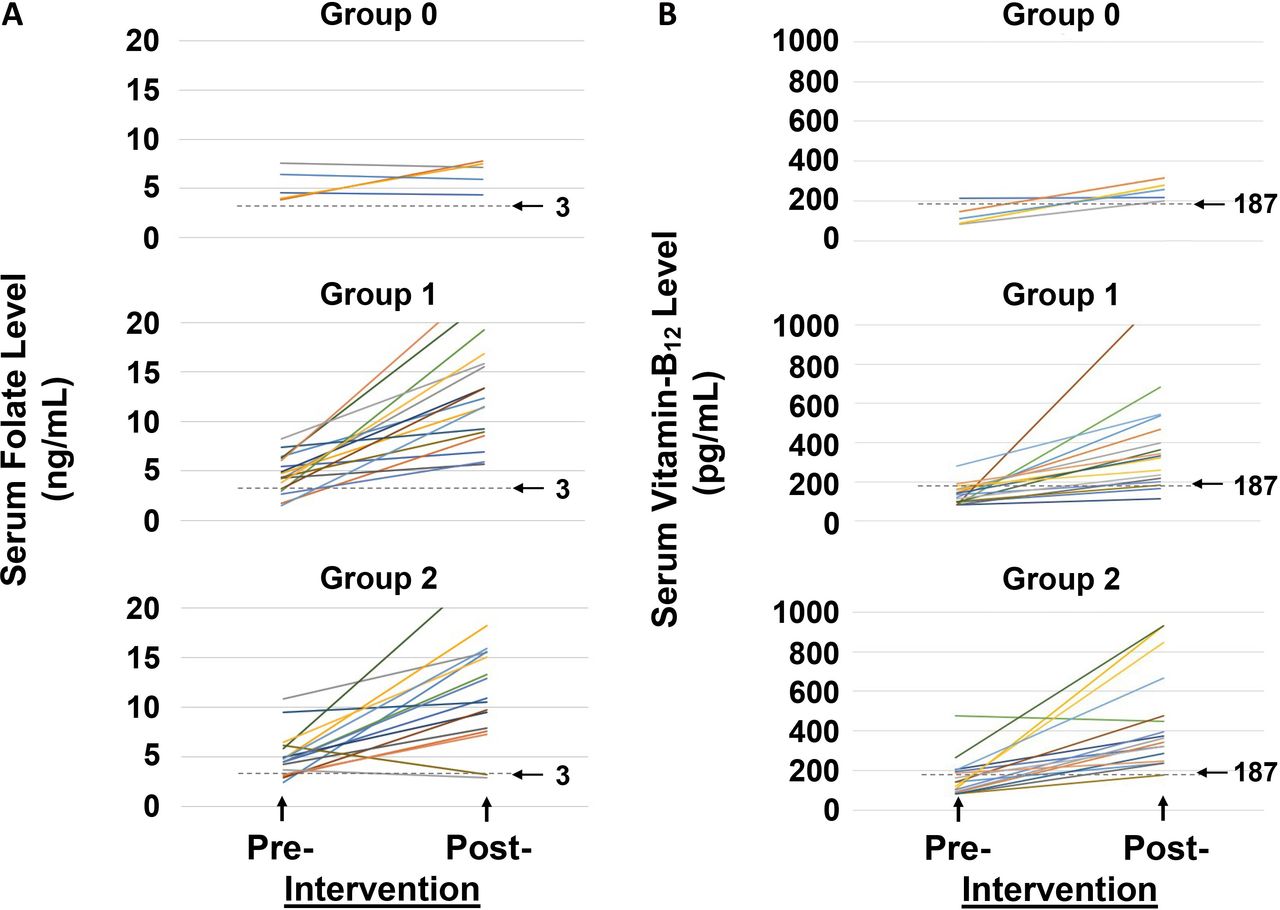
The individual responses of women to mock-fortified tea or folate-fortified tea are shown in figure 2A. Of significance, in Group-0 (figure 2A, upper panel), three of five women showed no change in pre-intervention and post-intervention serum folate results, but two of five women exhibited a small rise from 4 to 8 ng/mL. By contrast, all 17 women in Group-1 (including four with very low folate levels) exhibited a rise in serum folate levels after 2 months consumption of folate-fortified tea (figure 2A, middle panel); within this group, 11 had a rise in serum folate above 10 ng/mL whereas six remained below this value. Likewise, in Group-2 (figure 2A, lower panel) 17 of 19 women had a post-intervention rise in serum folate (including 12 with serum folate levels over 10 ng/mL). Among two women in whom post-intervention serum folate levels dropped, one into a low-normal level and another to below-normal values, their vitamin B12 levels were observed to double—to just below-normal in one, and to just above normal in the other, respectively. These findings reflect the well-known reciprocal effect of vitamin B12 deficiency in artificially raising serum folate levels, and reversal of this phenomenon on relief of vitamin B12 deficiency (discussed in Reference4). Similar results have been observed among Indian children with combined vitamin B12 and folate deficiency; after their vitamin B12 deficiency was treated, serum folate levels of children with severe, persistent folate deficiency also dropped (Reference4 and references therein).

Comparison of the individual responses of serum folate levels (A, left panels) and serum vitamin B12 levels (B, right panels) among various Groups of women at baseline (pre-intervention) and after 2 months (post-Intervention) consumption of a daily cup of tea using either mock-fortified teabags (Group-0, n=5, (average age=20±1 SD), upper panel), or folate-fortified and vitamin B12-fortified teabags (Group-1, n=19, (average age=20±2 SD) containing 0.1 mg vitamin B12 plus 1 mg folate per cup, middle panel) or (Group-2, n=19, (average age=20±1 SD) containing 0.5 mg vitamin B12 plus 1 mg folate per cup, lower panel). Each coloured line denotes a single woman’s pre-intervention to post-intervention response. The lower limit of normal for the serum folate concentration corresponding to a value of 3 ng/mL is shown as a horizontal dotted line in each of the three panels on the left. The lower limit of normal for serum vitamin B12 concentration corresponding to a value of 187 pg/mL is shown as a horizontal dotted line through each of the three panels on the right.
Taken together, these studies demonstrated that the majority (34 of 36) women in Group-1 and Group-2 who received a daily cup of tea fortified with 1 mg of folate over 2 months had a statistically significant elevation in serum folate levels when compared with controls in Group-0 who received mock-fortified tea.
Basal values and responses to vitamin B12-fortified tea
When baseline values for serum vitamin B12 (figure 1B) among women in Group-0 was examined, four of five had below-normal levels (normal serum vitamin B12 is 187–883 pg/mL (Metropolis Laboratory)); the remaining woman had a serum vitamin B12 level of 215 pg/mL, which is at the lower range of normal for this assay. (A serum vitamin B12 value of 300 pg/mL was used as a upper limit cut-off for ‘low-normal’ vitamin B12 values because ~15% of subjects with values between 200–300 pg/mL can have metabolic evidence for vitamin B12deficiency when more sensitive metabolite studies are employed).45 In Group-1, 15 of 17 women had below-normal serum vitamin B12 levels at baseline, with 2 women in the low-normal range (190 and 282 pg/mL). And in Group-2, 13 of 19 women had below-normal serum vitamin B12 levels, whereas 4 of 6 women had values in the low-normal range (194, 206, 264 and 202 pg/mL); only 2 women had more abundant serum vitamin B12 levels (at 313 and 476 pg/mL).
There was no significant difference in pre-intervention mean serum vitamin B12 levels among Group-0, Group-1 and Group-2 (figure 1B). Although there was a statistically significant post-intervention increase in serum vitamin B12 levels within each Group, the between-Group comparisons were not significant. This was because of an unexplained upward-drift in Group-0 where three of five women exhibited a small rise in the post-intervention serum vitamin B12 levels into the low-normal range (less than 300 pg/mL); one woman had essentially unchanged values from 215 to 217 pg/mL, whereas another rose from 148 to 324 pg/mL. This was similar to earlier observations by Solomon46 who noted variation in results (up to 23%) when individual subjects with borderline low-normal serum vitamin B12 values were followed longitudinally over 2–6 weeks, with documented differences in serum vitamin B12 values above 100 pg/mL in one-fifth of patients.46 This likely reflects the relatively imprecise nature of the serum vitamin B12 assay, especially at the lower range of normal values. In addition, the mean difference in post-intervention versus pre-intervention serum vitamin B12 in Group-0, Group-1 and Group-2, were 132, 250 and 294 pg/mL, respectively (figure 1B); this continued rise in serum vitamin B12 levels among women in Group-1 and Group-2 who received progressively more vitamin B12-fortified tea (when compared with Group-0) suggested a dose-response relationship.
The individual responses of women before and after the trial using vitamin B12-fortified tea is shown in figure 2B, where the depth of response reflected by post-intervention serum vitamin B12 levels are better contrasted between Group-0 (figure 2B, upper panel) versus Group-1 (figure 2B, middle panel) and Group-2 (figure 2B, lower panel). Thus, for women in Group-0 who received mock-fortified tea, there was only a small rise in serum vitamin B12 into the low-normal range. By contrast, in Group-1, 10 of 17 women who received tea fortified with 0.1 mg vitamin B12 raised their serum vitamin B12 levels over 300 pg/mL; the remaining women exhibited a smaller rise into the low-normal range (less than 300 pg/mL). Likewise, in Group-2, 13 of 19 women receiving 0.5 mg vitamin B12-fortified tea exhibited a rise in serum vitamin B12 above 300 pg/mL; among the remainder, 5 women who normalised their serum vitamin B12 values into the low-normal range had smaller rises (less than 300 pg/mL); only 1 subject with a baseline serum vitamin B12 level of 476 pg/mL failed to exhibit a rise in post-trial levels.
Taken together, these data following the use of different strengths of vitamin B12-fortified tea suggested a dose-response relationship, and the majority of women using vitamin B12-fortified teabags every day for 2 months raised their serum vitamin B12 levels well into the normal range. The inability of many women to exhibit a brisk rise in vitamin B12 level post-intervention likely reflects the severity of their baseline low-vitamin B12 status, and the need to clarify the optimum dose and duration of daily replenishment with vitamin B12-fortified tea.
Basal haemoglobin values and responses to folate-fortified and vitamin B12-fortified tea
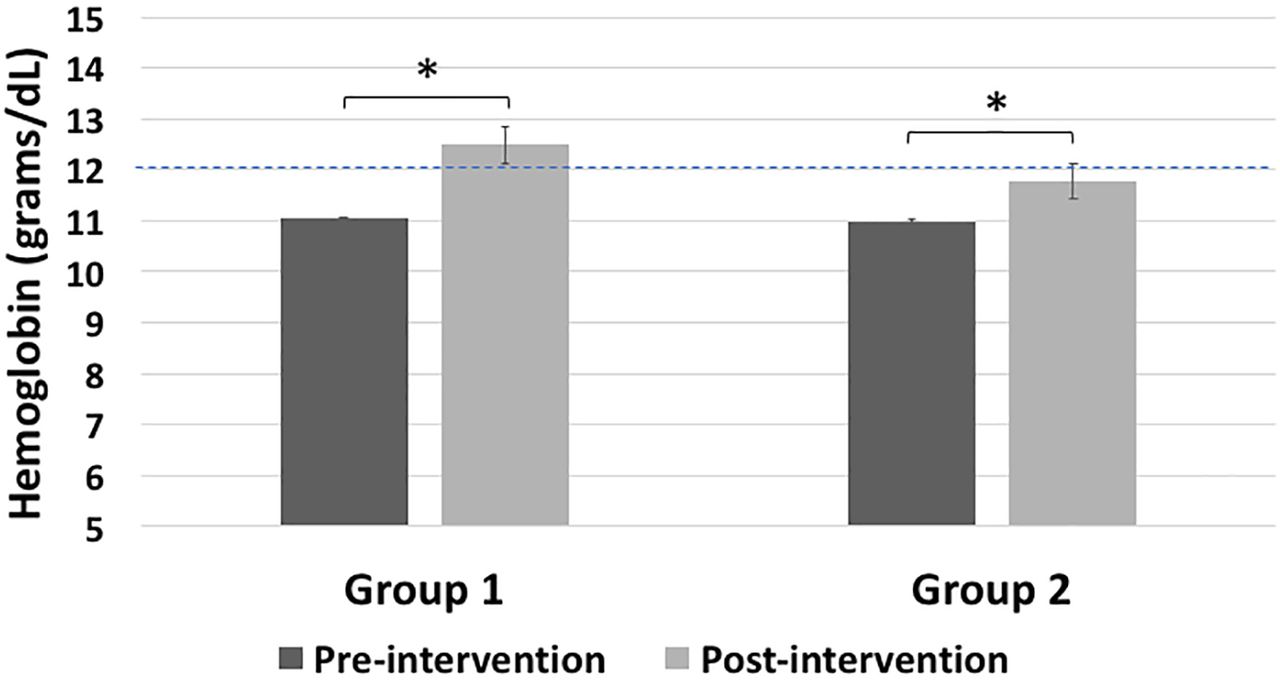
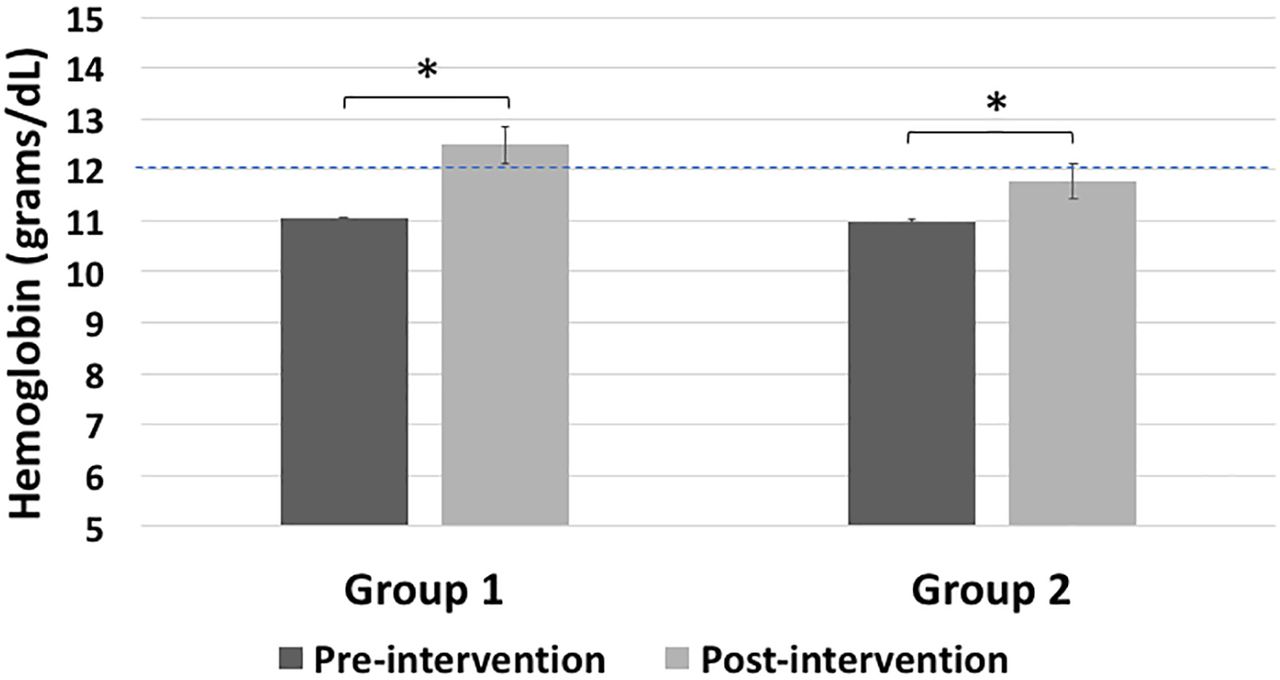
A majority of Indian women of childbearing-age have iron deficiency in addition to low-vitamin B12 and low-folate nutrition.1 Indeed, most study subjects had anaemia (haemoglobin less than 12 g/dL) in pre-intervention blood samples: Thus, in Group-0, 4 of 5 had anaemia (1 blood sample was lost); in Group-1, 14 of 16 had anaemia (1 blood sample was lost); and in Group-2, 15 of 19 had anaemia. Figure 3 shows a comparison of mean haemoglobin values in women from both Group 1 and Group 2 at baseline and after 2 months consumption of a daily cup of tea using folate-fortified and vitamin B12-fortified teabags. (Due to an inadvertent communication error, post-intervention haemoglobin levels were not uniformly obtained in all three Groups). There was a significant post-interventional mean rise in haemoglobin among women in Group-1 of 1.45 g/dL (95% CI 0.64 to 2.26, p=0.002) and in Group-2 of 0.79 g/dL (95% CI 0.11 to 1.42, p=0.027), which indicated a clinical response. Thus, among 12 women in Group-1 who had post-intervention haemoglobin tests, 7 normalised their haemoglobin with a rise of between 1–2 g/dL; and both women with normal haemoglobin values pre-intervention further increased their post-intervention haemoglobin by over 1 g/dL. Likewise, 4 out of 11 women in Group-2 with baseline anaemia had a post-intervention normalisation of haemoglobin of 1–1.5 g/dL, whereas 3 women with continued anaemia nevertheless improved their haemoglobin values by ~0.5 g/dL.
{kind=link}
{kind=link}
{kind=link}
Comparison of mean haemoglobin concentration in women from Group-1 and Group-2 at baseline (pre-intervention) (dark shaded bars) and after 2 months (post-intervention) (light shaded bars) consumption of a daily cup of tea using folate-fortified and vitamin B12-fortified teabags (Group-1, n=12, containing 0.1 mg vitamin B12 plus 1 mg folate per cup) and (Group-2, n=11, containing 0.5 mg vitamin B12 plus 1 mg folate per cup). The horizontal dashed line (set at 12 g/dL) signifies the cut-off between normal haemoglobin concentration and anaemia at sea level. Data is shown as mean±SE. The asterisk signifies a statistically significant difference (p<0·05) in the pre-intervention versus post-intervention haemoglobin concentration within each Group.
Thus, when taken together, there was a significant reversal of low-vitamin B12 and low-folate status that coincided with a significant mean increase of haemoglobin among those women from both Group-1 and Group-2 who were tested after consumption of a daily cup of folate- and vitamin B12-fortified tea for 2 months.
Discussion
To our knowledge, there has been no previous report on the therapeutic use of vitamin-fortified tea to raise the serum folate or vitamin B12 levels of women in India, or elsewhere. Although flour and rice fortification are under study, there are significant regional dietary variations throughout the vast Indian subcontinent (arising from cultural, religious, ethnic differences and beliefs3 5) that will necessarily limit the use of these fortified products to the regions they are consumed. However, tea is a universal beverage consumed by most adults in every city, town, village and hamlet throughout India. This fact highlighted tea as a potentially ideal vehicle for fortification with both folate and vitamin B12, which could result in its widespread distribution and use, and thereby decisively ensure long-lasting benefits for Indians.
Parenthetically, testing of tea as a vehicle for fortification with folate and vitamin B12 to reverse poor-folate and poor-vitamin B12 status among women of childbearing-age in India (ie, where tea is used as a ‘nutraceutical’) is entirely consistent with existing Food Safety and Standards Authority of India (FSSAI) regulations.44 FSSAI has also declared an intention to pursue ways to improve the vitamin status of vulnerable subjects in India47—that is, ‘Food fortification is a realistic and sustainable complementary strategy to food supplementation and dietary diversification to eliminate micronutrient deficiencies’; and, ‘It is, therefore, important to identify commodities that are ‘Fortifiable’, that is those staple foods that go through processing by organised industry’.
Vitamin-fortified tea efficaciously reverses low folate and vitamin B12 status in Indian women
We found a high prevalence of low-vitamin B12 and low-folate status as well as anaemia among women of childbearing-age in Sangli, India, irrespective of whether they were vegetarian or near-vegetarians—the latter are defined as non-vegetarians who consume small portions of animal-source foods often only once or twice a week.1 2 5 As a result, there is often little difference in dietary intake of folate and vitamin B12 content between those consuming vegetarian or non-vegetarian diets, as best illustrated among affluent urban-dwelling individuals and neighbouring slum-dwelling individuals in North India.4 48 Because of a strongly expressed preference for food-based vitamin supplements to reverse their extant low vitamin intake and status by scores of women of childbearing-age from several states of India (see online supplemental material), our focus was on identifying a commonly-consumed, scalable, fortifiable food for rapid replenishment of folate and vitamin B12.
Fortification with folate and vitamin B12 did not modify the terroir of the tea, thereby retaining its acceptability to women. In addition, heat exposure of these vitamins during the brewing of tea was far less intense when compared that during breadmaking using flour fortified with both vitamins, as reported by Winkels et al.41 For example, despite exposure to ~500°C for ~45 min (during breadmaking) followed by autoclaving—(at 119°C for 15 min to extract vitamins from bread prior to analysis)—which led to only a 25% net loss of both vitamins,41 consumption of three slices of bread daily led to a significant improvement in the status of both vitamins among healthy older people. In a similar vein, both vitamins were stable during the brewing of tea using vitamin-fortified teabags because daily consumption of tea fortified with 1 mg of folate per cup over 2 months significantly improved serum folate levels in 34 of 36 women; by contrast, there was an insufficiently meaningful change in the serum folate of women consuming mock-fortified tea. Moreover, among women using teabags spiked with 0.1 mg and 0.5 mg of vitamin B12 per cup, over one-half and two-thirds of women, respectively, increased their serum vitamin B12 levels well into the normal range.
Of clinical significance, the post-interventional improvement of serum folate and serum vitamin B12 levels in these women coincided with a statistically significant mean increase of their haemoglobin concentration when compared with pre-interventional levels. Therefore, it is reasonable to conclude that despite the likelihood of iron deficiency being present in this cohort, (i) many of these women had an element of folate deficiency and/or vitamin B12 deficiency related anaemia before intervention with folate-fortified and vitamin B12-fortified tea, and (ii) the post-intervention improvement in haemoglobin with reversal of anaemia in these women reflected a clinical response to tea-fortified with folate and vitamin B12.1 Thus, vitamin-fortified tea appears to be an efficacious vehicle for rapid replenishment of folate and vitamin B12 among young Indian women of childbearing-age.
Limitations of the study
This first-of-its-kind preliminary study,36 had several inherent and significant limitations that precluded it from rising to the level of a formal randomised controlled pilot trial.49 These limitations stem primarily from a lack of prior data on the use of fortified tea in raising the serum folate and vitamin B12 in humans, which led to insufficient preliminary data to calculate sample size; there was also a paucity in the number of control subjects; and a failure in assessment of the haemoglobin concentration in all control and experimental subjects.
A deliberate reduction in the number of control subjects recruited (when compared with experimental subjects) was strengthened by our finding of a high prevalence of low serum folate and serum vitamin B12 level among 60 young nursing students in Sangli (online supplemental figure S1), most of whom consumed a cup of tea every day. This suggested that there was an insufficient amount of folate and vitamin B12 in a daily cup of unfortified (or mock-fortified) tea to meaningfully raise the serum folate and vitamin B12 levels (in a control cohort) within 2 months. Therefore, because this was the very first preliminary study that was primarily aimed at testing the feasibility, efficacy and acceptability of vitamin-fortified tea, we opted to reduce the number of control subjects, and primarily focused on pre-intervention versus post-intervention values of both serum vitamins and the haemoglobin concentration. Parenthetically, post hoc analysis of the results and estimates of the group differences in serum folate levels indicated that the sample size required to detect difference in folate levels would be a minimum of 13 per group; this estimate is not too dissimilar from the number of subjects used in the present study.
Although we used an accurate Eppendorf pipette (conventionally used in biochemical studies) to manually add precise quantities of folate and vitamin B12 to each teabag, we did not measure the precise amount of residual folate and vitamin B12 released into the final cup of tea; future studies will need to examine this issue more directly. Nevertheless, the fact that the experimental group showed a significant improvement in serum folate and serum vitamin B12 levels after 60days of daily consumption of tea suggested that sufficient functionally intact vitamins released from vitamin-fortified teabags were well absorbed. Moreover, the concomitant significant post-interventional rise in haemoglobin concentration in this experimental group (when compared with pre-intervention levels) further point to the functional clinical effects of these absorbed vitamins in stimulating erythropoiesis and resolving anaemia among many of these Indian women.
Future studies
The results of our preliminary studies, which favour proof-of-concept, points to the use of tea as a potentially ideal vehicle33 for fortification with these vitamins in India. Vitamin-fortified tea can potentially be used in India in two ways: (i), For the delivery of vitamin-fortified tea that contains a full daily therapeutic replacement dose of folate and vitamin B12 that is specifically designed to rapidly replenish all those with either borderline low folate/vitamin B12 status or frank deficiency of these vitamins. By inference, the success of this approach predicts that (ii) fortification of tea with lower (maintenance) doses of folate and vitamin B12 can subsequently be used to ensure that those hundreds of millions who subsist on an insufficiently balanced diet (containing an inadequate amount of these micronutrients) can still receive an adequate replacement of these vitamins every day.
Therefore, the immediate challenge is to initiate formal randomised controlled trials49 in Indian women of childbearing-age with borderline deficiency of these vitamins to answer several inter-related issues: (1), Studies are needed to optimise the precise dose (and duration) of vitamin-fortified tea needed for rapid therapeutic replacement of vitamin B12 and folate; and (2), to determine the precise maintenance dose of vitamins to be added to vitamin-fortified tea to compensate for ongoing insufficient dietary intake of these vitamins. Moreover, because the majority of the Indian population use ‘loose tea leaves’ to prepare tea rather than teabags, (3), additional trials will need to compare the relative efficacy of using vitamin-fortified teabags versus vitamin-fortified loose tea leaves. Finally, although initial trials will be conducted among urban women professionals, (4), it will be imperative to define if equivalent results are achieved among rural women living in remote villages within Sangli district, who represent the majority of women living in villages throughout India. Studies to test each of these approaches to replenish folate and vitamin B12 in women using vitamin-fortified tea are in the planning stages.
Some considerations related to the introduction of folate- and vitamin B12-fortified tea in India
Several novel and positive attributes to the use of tea as a vehicle for fortification in India are summarised in the box 1. However, some issues and concerns related to the potential widespread introduction of vitamin-fortified tea warrant additional discussion.
Unique characteristics of tea as an excellent vehicle for fortification with folate and vitamin B12 in India
Tea is grown in the highlands of only 4 of 28 states in India from where it is efficiently distributed to reach people of every geographical location and every socio-economic group throughout India.
Tea is a cheap beverage consumed every day by most Indian adults and is also easily affordable by the poor.
India generates over 1200 million kilograms of tea annually34: ~50% from Assam (Assam Tea), ~25% from West Bengal (Darjeeling Tea), ~15% from Tamil Nadu (Nilgiri Tea) and <5% from Kerala (Munnar Tea).
All major tea companies in India have centralised tea producing factories close to large tea-plantations where tea can be fortified.
Fortification of tea with folic acid and vitamin B12 can be carried out during the penultimate step of the processing of tea, just prior to drying and packaging.
Once fortified, the dried tea leaves retain the folate and vitamin B12 which finely coats these tea leaves.
Loose tea is usually stored in closed tin or cardboard box containers, so fortified tea is protected from direct sunlight (which can be detrimental to the stability of folate and vitamin B12).42 43
Folate- and vitamin B12- fortified tea is stable to storage at room temperature for extended periods.
Folate and vitamin B12 are both water-soluble, resistant to the near-boiling hot water used in brewing tea, so the entire dose is immediately delivered into infused tea.
Excess folate or vitamin B12 consumed in tea is excreted from the body in urine and stool.
Both vitamins are non-toxic with no upper intake level for folate51 or any upper limit for vitamin B12.52 53
Neither the taste nor colour of the tea are affected by added folate and vitamin B12.
Addition of folate or vitamin B12 as therapeutic agents to tea are in keeping with the Food Safety Standards Authority of India (FSSAI) regulations for nutraceuticals44 and the spirit of the FSSAI Joint Declaration to identify additional vehicles for fortification.47
Clinical trials in various populations need to be carried out to identify the therapeutic dose of folate and vitamin B12 required to fully replenish a deficiency rapidly among various populations at risk.
After subjects are fully replenished, additional clinical trials will need to identify the minimal fortification dose of folate-fortified and vitamin B12-fortified tea required for long-term supplementation of the diet.
Folate and vitamin B12 are relatively inexpensive vitamins so fortification of tea ought not to significantly raise the price of tea.
Costs arising from fortification of tea with folate and vitamin B12 by major tea companies in India can be attributed to their Government of India-mandated expenditures in ‘Corporate Social Responsibility’.54
(1) The Government of India has a programme that is intended to improve the iron and folate status of women of childbearing age by providing weekly supplements containing a combination of iron-folic acid tablets (composed of 100 mg elemental iron and 500 mcg folic acid). However, in practice, adolescent and young women uniformly admit to poor compliance (adherence) in taking these tablets regularly, which is commonly triggered by the side effects of iron. Indeed, among the hundreds of women we have informally surveyed throughout India (see online supplemental material), far less than 5% of women admit to consistently using weekly iron-folate tablets. Iron-folate tablets are also commonly distributed to Indian women once they realise they are pregnant, but this is usually well past the time when developmental decisions have been made regarding closure of the fetal neural tube (which occurs by the end of the fourth week after conception). Therefore, if these women have had a persistent low folate status in the periconceptional period, this fact alone increases the risk for failure in closure of the neural tube in the fetus, thereby resulting in a baby with a NTD.1 50 By contrast, the daily consumption of vitamin-fortified tea has potential to improve the periconceptional folate and vitamin B12 status among women of childbearing age, which can markedly reduce the risk of having a baby with a NTD.1 50 Importantly, this positive outcome with vitamin-fortified tea can easily be achieved without side effects and minimal effort on the part of women, since consumption of a cup of tea is an intrinsic part of their daily diet. Another issue that has not been sufficiently considered by the Government of India programme of supplementation of iron-folate to women of childbearing age is that merely administering folic acid (with iron) in the face of ongoing depleted or deficient vitamin B12 cannot possibly help fully restore folate metabolism to normal. This shortcoming can also be resolved by the introduction of folate-fortified and vitamin B12-fortified tea in India.
(2) In general, fortification of foods (milk with vitamin D, or flour with folate) has not led to increased consumption of these foods. In this context, because a large per cent of the population in India has a low folate and vitamin B12 status, there will necessarily need to be two strengths of vitamin-fortified tea: one fortified with a higher dose of both vitamins for rapid replenishment of depleted or deficient stores, and another fortified with a lower dose of vitamins for long-term maintenance of optimum folate and vitamin B12 status to compensate for a diet that is persistently low in folate and vitamin B12 content. Finally, it should be noted that even though tea is well known to interfere with iron absorption, this attribute has not altered the fact that a cup of tea remains the unanimous hot beverage of choice throughout India. Thus, the fortification of tea per se is unlikely to alter the consumption of tea in India.
(3) Nevertheless, widespread availability of any fortified food with vitamins necessarily raises questions on the potential for inadvertent vitamin toxicity if the vehicle containing vitamins (in this case, tea) is taken in excess. This has not been a clinical concern for either folate or vitamin B12 because any excess vitamin consumed in tea is easily excreted from the body in urine and stool. A recent paper points to the lack of any scientific basis for setting any upper intake level for folate.51 As also noted recently52 in the 2020-updated National Institute of Health (USA) Office of Dietary Supplements ‘Fact Sheet for Health Professionals’: ‘The Food and Nutrition Board did not establish an upper limit for vitamin B 12 because of its low potential for toxicity. 53 Even at large doses, vitamin B 12 is generally considered to be safe because the body does not store excess amounts.’ Thus, there appears to be no issue of concern related to a tolerable upper intake level for vitamin B12 in the USA (since 1998,52) with no significant potential limitations to the concept of fortification of tea with either folate and vitamin B12 in India.
(4) Finally, both folate and vitamin B12 are relatively inexpensive vitamins, so fortification of tea ought not to significantly raise its price. In addition, the added costs that arise from fortification of tea with folate and vitamin B12 by major tea companies in India can be attributed to their Government of India-mandated expenditures in ‘Corporate Social Responsibility’.54
Potential beneficial effects of folate-fortified and vitamin B12-fortified tea on target Indian populations at various stages of life
There is a large body of evidence that Indians at various stages of life—such as women of childbearing-age, the mother-fetus dyad throughout pregnancy and later in post-natal life, as well as children, adolescents and both adult and elderly men and women—can potentially benefit from the use of vitamin-fortified tea. For example:
(1) Based on an estimated 26 million births annually in India, and using a very conservative prevalence of five cases of NTDs per 1000 live births, Kancherla and Oakley32 estimate that 90% of the 130 000 cases of NTDs each year can be prevented by a robust food folate-fortification programme that ensures periconceptional folate supplements to women in India. (This estimate does not take into account the additional potential prevention of severe cases of NTDs that can also present as stillbirths).
Of additional significance, and following directly on our earlier studies in mice,55 56 several studies have consistently pointed to observations in humans that lower maternal folate status in early pregnancy is associated with psychological–neuropsychiatric disorders that present in childhood.57 Affected children can exhibit hyperactivity or inattention and peer problems, aggressive behaviour, learning deficits, anxiety and/or depression.1 4 57–62 Conversely, women with replete folate stores during early pregnancy provide an in utero environment for optimum neurodevelopment that impacts positively on the child’s intellect, emotional intelligence, cognition, language and academic performance.1 60 63 64 Thus, consumption of a daily cup of tea that is fortified with folate and vitamin B12 by all Indian women of childbearing-age and throughout pregnancy has the potential to dramatically improve the overall outlook of millions of their children each year.
(2) Indian children born to micronutrient-depleted mothers have a high propensity to have a low folate and vitamin B12 status1–3 5 from birth through childhood and adolescence, which contributes to poor growth65 and compromised optimum intellectual development, and gross motor and problem-solving skills.66 In Sangli, children 10 years of age onwards are fed a daily cup of tea (Personal Communication: Ms Lata Deshpande of Dr Deshpande Bal Vidya Mandir, Sangli); so, giving them a daily cup of vitamin-fortified tea has the potential to prevent some of these serious deficits among such children at risk.
(3) Adult Indian men also have a high incidence of vitamin B12 deficiency; thus, despite being vegetarians or professed non-vegetarians, from among 204 men and women (aged 27–55 years), 47% had serum levels consistent with vitamin B12 deficiency.6 Another study showed 67% of men of the middle and lower socio-economic strata had low vitamin B12 concentrations.7 The fact that (a) these individuals had similarly unbalanced diets containing a low dietary folate content as women, (b) many such women with vitamin B12 deficiency in this region were unable to normalise their elevated homocysteine levels after vitamin B12 administration24 and (c) serum folate is falsely elevated in those with vitamin B12 deficiency,4 all suggested that the extent of folate deficiency has been underestimated.1 4 Hence, consumption of tea fortified with folate and vitamin B12 can also benefit Indian men.
(4) Finally, among the middle-aged and elderly, chronic hyperhomocysteinaemia (which is largely due to longstanding vitamin B12 and/or folate insufficiency) is a major risk factor in occlusive vascular diseases—particularly increased small-vessel cerebrovascular disease–related strokes,67 68 dementia and Alzheimer disease.69 70 And accelerated brain atrophy is often a characteristic among those with mild cognitive impairment who then go on to develop Alzheimer disease.71–74 There are now three randomised controlled trials among elderly patients to suggest that homocysteine-lowering therapy can significantly slow down the accelerated rate of brain atrophy and improve cognition. Indeed, a recent consensus statement by a panel of experts have concluded that elevated plasma total homocysteine is a modifiable risk factor for development of cognitive decline, dementia and Alzheimer disease in older persons.70 Collectively this information and the availability of a common ‘food’ (tea) to fortify with folate and vitamin B12, as well as provision of early ‘proof of concept’, should be sufficient impetus for the Indian Ministry of Health to support projects designed to expand the population target for optimisation of folate and vitamin B12 status to also include middle-aged and elderly Indians.
Taken together, consumption of folate-fortified and vitamin B12-fortified tea in India can potentially have very significant health benefits across several stages of life.
Potential application of folate-fortified and/or vitamin B12-fortified teabags for Western countries
Fortification of teabags with vitamin B12 alone can also have utility among several groups in the West who are at-risk for vitamin B12 deficiency, particularly in regions where folate-fortification of flour is mandated. In USA, this includes between 20%–30% elderly with food-vitamin B12 malabsorption, some diabetics on metformin and approximately 8 million vegetarians.1 5 Estimates that nearly one-half of Americans consume tea every day, suggests that fortification of teabags with vitamin B12 can reach a large number. In addition, voluntary fortification appears ineffective to maintain optimum vitamin B12 and folate nutrition of older Irish adults where the prevalence of deficient or low vitamin B12 status (less than 185 pmol/L) was 12%, whereas the prevalence of deficient or low folate status was 15%.75 Since tea is a popular daily drink in Ireland and many other countries where flour-fortification with folate is not mandated, folate-fortified and vitamin B12-fortified tea could be an available option for those at-risk for these deficiencies in such populations.
Finally, it should be pointed out that oral administration of full therapeutic daily doses of vitamin B12 is now standard therapy for food-vitamin B12 malabsorption as well as pernicious anaemia1 40; therefore, tea-fortified with vitamin B12 can be tested for use in these conditions as a substitute for daily tablets.
Scope of vitamin-fortification of tea worldwide
Consumption of a daily cup of tea is common practice all over the world. It is therefore not an insignificant fact that there exist studies which document a deficiency of folate and vitamin B12 in each of the top-10 tea producing countries.1–5 23 76 Therefore, widespread adoption of tea-fortified with folate and vitamin B12 in these countries can further benefit their resident adolescents and adult populations. Although China tops the list producing over 2 million tons, with India (~1.2 million tons) as the next largest producer,34 Kenya (~430 000 tons), Sri Lanka (~340 000 tons) and Vietnam (~214 000 tons) are large producers and exporters of tea. Other top-10 tea producers include (in descending order) Turkey, Indonesia, Myanmar, Iran and Bangladesh. Thus, our preliminary studies documenting the efficacy of vitamin-fortified tea to rapidly replenish depleted stores in Indian women also points to the potential for reversing nutritional folate deficiency and vitamin B12 deficiency in these countries using this vehicle.
In conclusion, tea has several positive attributes as a scalable, contextually-appropriate, centrally-processed, affordable, widely distributed and outstanding food-based vehicle for fortification with folate and vitamin B12 in India (and other tea-consuming nations). Our preliminary study suggests that vitamin-fortified tea is acceptable, feasible and efficacious in improving the low -folate and -vitamin B12 status of Indian women of childbearing age. This warrants additional study with several formal randomised clinical trials49 as discussed above, because confirmation and successful implementation of a programme for the fortification of tea with folate and vitamin B12 has potential to dramatically improve the lives of hundreds of millions of Indians every year.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data relevant to the study are included in the article.
Ethics statements
Ethics approval
The Ethics Committees of the Kulloli Institute of Nursing Sciences, the RR Patil College of Nursing Education and College of Homeopathy, as well as the Board of Trustees of Kulloli Charitable Trust, Tatyasheb Ghatage Charitable Trust and Manavrahat Charitable Trust, all from Sangli, India, approved this study.
Acknowledgments
We thank Ms Neelam R Chand and Ms Maya K Murthy (Indianapolis, USA) who enthusiastically participated in the first set of blinded taste tests using various folic acid and vitamin B12 preparations. We also thank Dr Utpal P Dave of Indiana University School of Medicine for critical review of an early draft of the manuscript. The support and assistance of Mr Nitin B Shah and Dr Sanjyot S Patil (Manavrahat Charitable Trust), Drs Sharad T and Rohini S Ghatage (Ghatage Multispecialty Hospital and Post-Graduate Institute), Principals Smt Neha Awale and Dr Jaykumar Bhanuse (RR Patil College of Nursing Education and College of Homeopathy), Principal Ms MV Kagalkar and Dr SA Kulloli (Kulloli Institute of Nursing Sciences), Ms Kavita S Bhosale and Staff (Ghodawat Diagnostic Centre Pathology Laboratory) and Mr Dileep Shah (Maharashtra Tea Depot)—all from Sangli—in various facets of this study, is gratefully acknowledged.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Footnotes
Contributors RMV developed, designed and facilitated the study, recruited subjects, prepared vitamin-fortified tea, coordinated blood testing of subjects, collected and compiled data, revised the paper and was responsible for study oversight. MJA prepared figures, analysed the data and performed statistical analysis. ADZ prepared vitamin-fortified tea, recruited subjects and helped collect data. MSS prepared vitamin-fortified tea, recruited subjects and helped collect data. SJK developed, designed and facilitated the study. ACA conceived, developed, designed and facilitated the study, prepared vitamin-fortified tea, analysed data, wrote the paper and is primarily responsible for the final content of the paper.
Funding This study was supported in large part by funds from the Manavrahat Charitable Trust, Sangli, Maharashtra, India.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.