Article Text

Abstract
Background In the tribal state of Jharkhand, there have been very few studies on micronutrient deficiency and how it is addressed among school children. This study was conceived and undertaken to assess the effect of milk supplementation on the micronutrient status of school children.
Design A comparative observational study was conducted among school children of a tribal district in India during 2017–2018. Two groups of schools/clusters were randomly selected, one with milk supplementation and the other without supplementation. A total of 318 children from the two groups of schools were recruited for biochemical analysis of certain micronutrients, such as calcium, vitamin D, vitamin B12 and iron (haemoglobin level), using cluster random sampling. Data were analysed using SPSS V.20.0 software, and multiple logistic regression analysis was done to determine the predictors of serum calcium and vitamin B12 level among school children.
Results Almost all children from both groups had vitamin D deficiency. A higher risk of lower serum vitamin B12 level (OR 2.59, 95% CI 1.61 to 4.16) and calcium level (OR 3.36, 95% CI 1.74 to 6.49) was observed in children of the control group. The difference in the proportion of anaemia in the two study groups was found to be statistically insignificant. Milk consumption was found to be the only significant predictor of normal vitamin B12 and calcium level in the present study.
Conclusions In this study, it was concluded that milk consumption may help in improving the calcium and vitamin B12 status of school children of a tribal state, whereas it does not have any significant effect on vitamin D level.
- nutrient deficiencies
- nutrition assessment
- malnutrition
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
In this study, fortified milk has helped in improving calcium and vitamin B12 amongst school children.
Vitamin D levels in the school children were very low in the study subjects, amost all were vitamin D deficient.
Milk has improved the status of anemia in the study subjects but was not statistically significant.
Introduction
India contributes to one-third of the total number of stunted children under 5 years of age globally,1 and this malnutrition continues to exist among school children and adolescents despite various ongoing nutrition programmes in the country. Malnutrition results in an underdeveloped brain, with long-lasting harmful consequences of diminished mental ability and learning capacity, poor school performance, and increased risk of nutrition-related chronic diseases such as diabetes, hypertension and obesity in the future.2–4 Not only macronutrients but micronutrients also significantly contribute to problems related to undernutrition. These problems seem to be more relevant in developing countries like India, where a significant proportion of the population are still unable to meet their hunger needs.
In the last seven decades, there have been several initiatives by the Government of India to check for nutritional problems across various age groups, but the problem of both macronutrient and micronutrient deficiencies remains a serious concern in the country.5 6Among many nutrition improvement measures in the country, the mid-day meal scheme is one such ubiquitous programme aimed to supplement the nutritional needs of school children and increase overall school attendance. State governments have got the flexibility to decide the menu for mid-day meal programmes and preferably select local food items rich in macronutrients and micronutrients for school children. The government of Jharkhand has always remained open for suggestions and innovations which may improve the nutritional status of school children. Experts from different sectors proposed that the government keep milk as an option in mid-day meals considering its wide acceptability and availability as well as established benefits in improving nutrition.
Milk is a food item enriched with good-quality nutrients. There is evidence in the literature way back in 1929 of using milk as a food supplement for school children to improve overall growth in height and weight.7 Over the years, studies across the globe have established the fact that milk is an important source of nutrition and has a significant role in improving the health of school children.8–12 Milk and dairy products contain various vitamins and minerals which contribute to the different vital functions of the body. There are macroelements (calcium (Ca), magnesium (Mg), sodium (Na), potassium (K), phosphorus (P) and chlorine (Cl)) and oligoelements (iron (Fe), copper (Cu), zinc (Zn) and selenium (Se)) in the mineral fraction of milk. Almost all lipophilic (A, D, E and K) and hydrophilic (B complex and C) vitamins are also present in the fat and aqueous fraction of milk. Evidence also suggests milk as one of the contributors to increased uptake of nutrients in children.13–15
Severe micronutrient deficiencies usually result in typical deficiency diseases such as night blindness, rickets, hypocalcaemic tetany, etc. However, milder forms of micronutrient deficiencies are much more common and frequently go unnoticed. The detrimental effects of such suboptimal status are not clear, but the assumption persists that this subclinical deficiency leads to incessant metabolic and pathological changes in the body over a period of time.16 Similar condition also holds true for macronutrient deficiency in children. Considering macronutrient and micronutrient deficiencies in rural school children, the government of Jharkhand, in collaboration with Jharkhand Milk Federation (JMF), launched a nutrition supplement initiative called ‘Gift Milk Programme’ in the Latehar district of Jharkhand, India. In this new initiative, 200 mL fortified (with vitamin A and vitamin D) flavoured milk were provided on all working days to 36 schools catering to 14 000 students during 2017–2018. In consonance with the programme, an evaluation research was designed to study the effects of milk supplementation on the health of school children. The present paper is an attempt to assess the effect of milk supplementation on the status of selected micronutrients among school children of Jharkhand.
Methodology
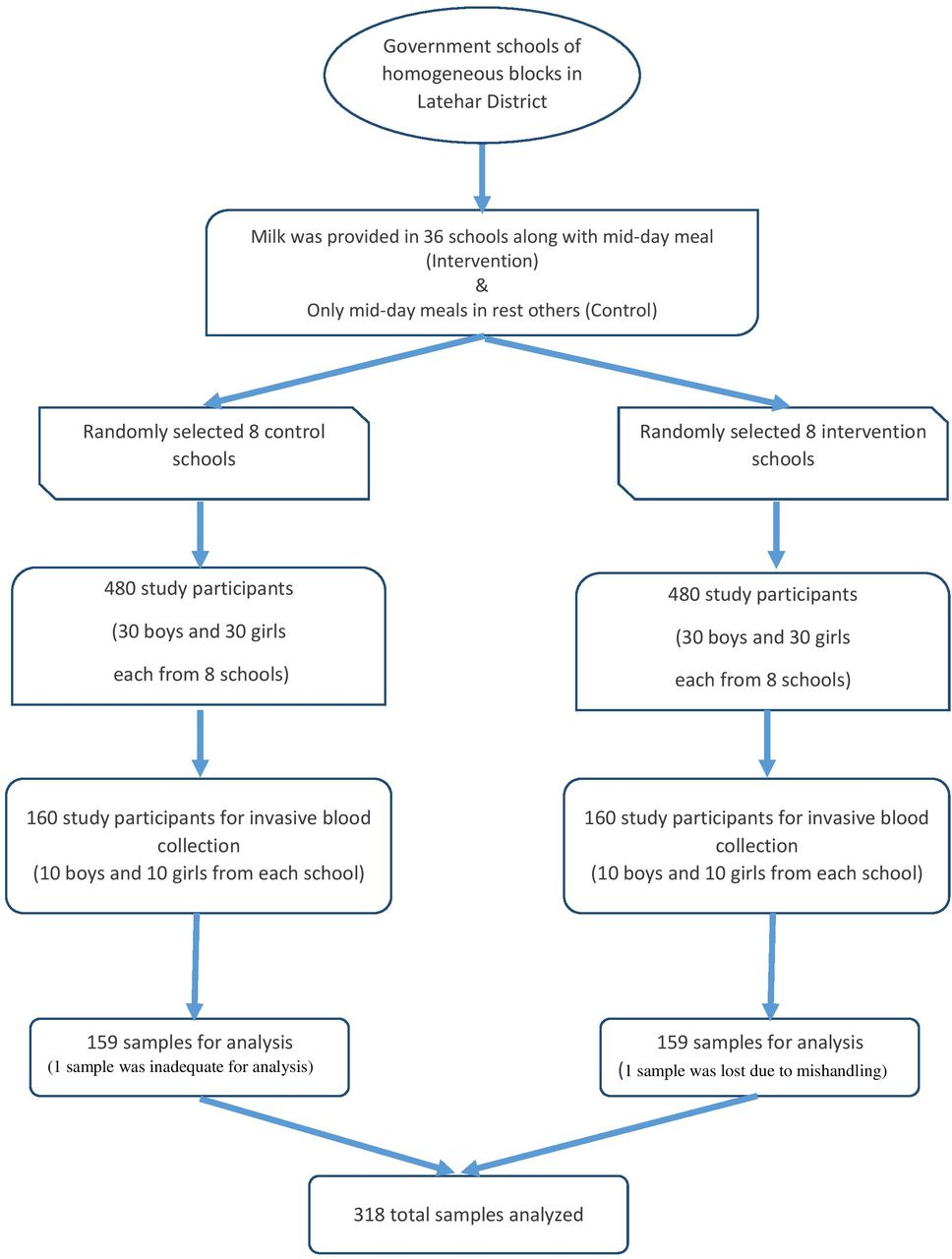
The study was conducted in selected government schools of homogenous blocks in the Latehar district of Jharkhand from October 2017 to January 2019. This was a comparative, school-based observational study using multistage random sampling method. In the first stage, all government schools of the Latehar district were listed and were further divided into programmatic/intervention schools and control schools. In the second stage, eight schools from each group were randomly selected using cluster random sampling. Each school was considered a cluster and equal numbers of subjects were recruited from each cluster. In the third stage, 60 students from each selected school were chosen as study subjects. The students were selected using systematic random sampling and the male to female ratio was maintained at 1:1. In this way a minimum of 480 school children were selected from each group. Selection of schools, sample size determination and the number of students from each school were in accordance with the statistical methods and the planned steps of multistage random sampling. A total sample size of 960 was studied considering the prevalence of malnutrition (40%), relative precision (10%), 95% CI and design effect (1.5) for this study.17 Before deciding on the schools, utmost care was taken to ensure that both the intervention and the control schools were substantially separated from each other to avoid spillover effect in the group as well as other operational issues. Only 20 consecutive children from each school (male to female ratio: 1:1) were selected from the initially sampled group of 60 students. From these children, 5 mL venous blood samples were drawn from the median cubital vein in the antecubital fossa using a vacutainer under all aseptic conditions. Thus 33% (320 out of 960) of the students were evaluated for various micronutrients considering limitations in resources, timing, and ethical and statistical considerations. Two samples were discarded, one due to less quantity and the other due to mishandling, and hence micronutrient evaluation was done for 318 samples. Therefore, the findings of the present study are limited to 318 school children only (figure 1).
{kind=link}
Flow chart showing the selection of study participants for the study.
This research was part of a longitudinal study which was divided into three phases: preintervention/baseline, intervention/programmatic and postintervention/endline assessment. During the preintervention phase, baseline data were collected from the study subjects. These comprised sociodemographic information, health status, anthropometric measurements and haemoglobin level. In the programmatic phase, school children from the programmatic/intervention schools were given 200 mL fortified flavoured milk in disposable packs during the break period of each working day for 1 year (from December 2017 to November 2018). The milk was provided by JMF in disposable packs under cold chain to all schools. Its uninterrupted supply, cold chain and quality assurance were continuously monitored by a third party under the guidance and supervision of the National Dairy Development Board Foundation for Nutrition in Anand, India. In the postintervention/endline assessment phase, data on sociodemographic profile, health status and anthropometric measurements of study participants were again collected. Apart from this, the blood samples of 20 children from each school/cluster were taken to evaluate the level of serum vitamin B12 (Serum Chemiluminescent Micro Particle Immunoassay), serum calcium (Serum/Arsenazo III), serum vitamin D (Serum Chemiluminescent Micro Particle Immunoassay) and haemoglobin (Automated Blood Cell Counter; Beckman Coulter). The blood was sampled only once during the study and was done after 1 year of intervention in a span of 20 days in December 2018 from all the control and intervention schools. For data analysis, normal level of serum calcium was considered at 8.8–10.6 mg/dL, for vitamin B12 187–883 pg/mL and for vitamin D 30−100 ng/mL. This was in accordance with the standard laboratory values of the National Accredited Board of Laboratories testing laboratory and equipment used. Anaemia among the study subjects was classified following the WHO guidelines according to age.18 Anaemia was taken as a proxy indicator of iron status. The investigators in our team carried out all research activities from data collection to data analysis.
Data analysis
Data management was done in Microsoft Excel V.2016 and statistical analysis in SPSS V.20.0. Mean and SD were used to express quantitative data, while proportions and percentages were used for qualitative data. Regression analysis was done to understand the predictors, and the association between variables was interpreted using OR. The study was done after taking consent and assent from the parents/guardians and children (adolescents), respectively. The school authorities were informed in advance about the research and permission was sought to conduct the study.
Results
In the present study, 960 children were included and 318 were chosen for biochemical analysis of micronutrient status. The gender distribution in both groups was similar and nearly equal. Majority of the subjects belonged to the 11–19 years age group. Socially, only a few of them were from the upper caste and the rest were from other backward caste and scheduled caste and tribes. There were more subjects from the ethnic tribes in the control group (44.7%) compared with the intervention group (26.4%). The birth order of the subjects was similar in both groups (table 1).
Sociodemographic characteristics of the subjects (N=318)
Nearly all subjects in both groups were found to have low vitamin D level. Serum vitamin B12 deficiency and serum calcium deficiency were more common among subjects of the control group. Using bivariate regression analysis, it was found that after milk consumption the chances of having normal serum vitamin B12 level were more than two times (OR 2.59, 95% CI 1.61 to 4.16) and that of normal serum calcium level more than three times (OR 3.36, 95% CI 1.74 to 6.49). Moreover, the mean serum vitamin B12 level and serum calcium level were also significantly higher among the subjects of the intervention group compared with the subjects of the control group. Although anaemia was found to be more common among the subjects of the control group, increased risk of anaemia was statistically not significant (OR 1.54, 95% CI 0.97 to 2.45) (table 2).
Bivariate regression analysis of the status of micronutrients among subjects from both groups (N=318)
Logistic regression analysis was done for predictors of normal serum calcium level and normal serum vitamin B12 level among the study subjects. Vitamin D and haemoglobin levels (anaemia) were statistically insignificant across the two groups and hence were not included in the regression analysis. The main predictor tested was milk consumption by study subject, gender, ethnicity and birth order. For normal serum calcium level, milk consumption was found to be an important factor (OR 3.27, 95% CI 1.67 to 6.39). Other factors were not significant for normal serum calcium level. Similarly, for normal vitamin B12 level, milk consumption was also found to be an important predictor (OR 2.95, 95% CI 1.80 to 4.85). It was also noted that tribal ethnicity was found to be associated with risk of low vitamin B12 level (OR 0.54, 95% CI 0.32 to 0.91) in comparison with non-tribal ethnicity. Other factors were significantly not associated with serum vitamin B12 level (table 3).
Logistic regression analysis of predictors of normal serum calcium and serum vitamin B12 status among the study subjects
Discussion
Micronutrient and macronutrient deficiencies in the Indian population are rampant despite the country being one of the major producers of milk, fruits, vegetables and grains.19 While there are many studies on iron deficiency, vitamin A deficiency and iodine deficiency, there are relatively fewer studies on vitamin D, vitamin B12 and serum calcium status in India especially among school children.4 The current study is unique in the sense that there have been no studies on the studied micronutrients in a tribal population.
The present study was done in children and adolescent age groups and assessed the effect of milk supplementation on their vitamin D, serum calcium, vitamin B12 and haemoglobin status. Almost all children of both groups (99.4%) have low level of vitamin D in their blood. Many Indian community-based studies have shown a higher prevalence (50%–94%) of vitamin D deficiency among their study subjects of different age groups and gender.20–23 The finding of the present study on vitamin D status is in concordance with the study done by Kapil et al 24 in Shimla in a similar age group (6–18 years) which has shown a prevalence of vitamin D deficiency of 93%. However, studies done by Basu et al 25 among subjects in the 1–16 years age group in 2015 and Angurana et al 26 among subjects in the 3 months–12 years age group in 2014 have reported a prevalence of vitamin D deficiency of 52.9% and 40.2%, respectively. However, these two studies were done in a hospital setting and there is a possibility of higher number of subjects of better socioeconomic status. These could be the possible reasons for the lower prevalence of vitamin D deficiency in their studies. Although milk contains varying levels of vitamin A, D and E, milk itself has not been considered an important dietary source of vitamin D.27 28 Also, in the present study, there was no significant difference in vitamin D level in the subjects of both groups and nothing can be attributed to fortified milk.
Vitamin B12 is an important micronutrient for the human body, and the main sources of vitamin B12 for humans are animal products.29 Among animal products, milk is considered an important source of vitamin B12 for human beings, and 250 mL cow milk may fulfil the 50% recommended dietary allowance of vitamin B12.30 31 The current study found that vitamin B12 level was better among children who regularly consumed milk for 1 year than those who did not consume milk. Similar finding was reported by a study done by Naik et al 32 in 2013 in India. Other studies across the world have also found that bioavailability of vitamin B12 in milk is better than fish or other sources.33 34 Since pure vegetarians are more likely to be deficient in vitamin B12, addition of milk in their diet can reduce this deficiency to a certain extent. This nutritional intervention can be helpful for children of lower socioeconomic status in India who are unable to consume milk daily. Unpublished data of this study also show that less than 10% of children were consuming milk on a regular basis and few (3%) children have never tasted milk in their lifetime, depicting the vulnerability of their dietary and nutritional status.
Calcium is another vital micronutrient for the human body, required for many biochemical processes. Among various dietary sources, milk, especially cow milk, is an important source of readily available calcium.35 Apart from the concentration, the bioavailability and absorption of calcium from milk are better as compared with cereals and green leafy vegetables.36–38 Our study also reported that children who consumed milk had significantly better calcium level in their body. Other studies in the world have also highlighted the beneficial effect of milk on calcium level in the body and its overall effect on bone in humans.39 40
Many published literature supports the view that consumption of milk is associated with iron deficiency anaemia, especially among infants, toddlers and young children. The main possible mechanism for this association is poor availability of iron and ascorbic acid in milk or dairy products and decreased absorption of iron from other food items when consumed with milk.41–44 Another possible mechanism for this relation between milk consumption and iron deficiency anaemia is the occurrence of microhaemorrhages in the gut especially among infants.41 45 Contrary to this evidence, the present study suggests that consumption of milk is associated with less occurrence of anaemia. In this study, the proportion of subjects with anaemia was higher among the control group compared with the intervention group. There are schools of thoughts which opine that calcium does not affect iron absorption in the long term and that absorption of iron from cereal-based diets in human body is unaffected by the addition of milk.46 47 The researchers in our study also highlighted the fact that anaemia in Indian children is not only due to iron deficiency, but may also be due to protein deficiency owing to poor quality of protein, based on earlier evidence.48 Milk supplementation in the intervention group may be providing good-quality protein along with other nutrients, helping in the better synthesis of haemoglobin, which can be the reason for the lower prevalence of anaemia in the intervention group. The difference in proportion in the two groups of the current study was statistically insignificant, and needs to be confirmed by other assays and warrants further research to support the viewpoint.
Conclusion
From this study, it can be concluded that milk consumption may help in meeting the calcium and vitamin B12 requirements of school children of a tribal state, whereas it does not have any significant effect on vitamin D level. Overall vitamin D levels in the study population are abysmally low, and providing fortified milk with the present amount of vitamin D fortification for 1 year alone may not be sufficient to meet the daily requirements and compensate for the existing low levels of vitamin D. Haemoglobin levels have improved with fortified milk supplementation, but the difference in the study groups is not statistically significant. Hence, other diet and lifestyle interventions may be needed to combat anaemia among school children.
There were some limitations to the present study. At baseline, we did not collect blood samples for biochemical assessment, which could have given a better picture of the effect of milk on micronutrients. The smaller sample size due to financial and time constraints was a major limitation of this study. The intervention phase of 1-year duration may be another limitation of the study and a longer duration could present a clear picture of the long-term effects on different nutrients. Nevertheless, the present study has shown a means to improve the status of certain micronutrients among children in remote areas and of lower socioeconomic status. A detailed study with a larger sample size and longer duration can pave the way for provision of milk supplementation for school children.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
The research was approved by the Institutional Ethics Committee, RIMS, Ranchi, Jharkhand, India.
Acknowledgments
We are grateful to all the postgraduates and lab technicians of PSM, RIMS Ranchi for their assistance in carrying out the study in the selected schools of Latehar, India.
References
Footnotes
Contributors DK, CK, AK, RKR and VK conceived the study and were involved in designing the study. VS and MK guided and supervised the data collection. SBS and NK helped in analysing the data and provided input in the preparation of the manuscript. CK and DK prepared and aligned the manuscript. All the authors read, critically discussed and approved the final manuscript. DK is the guarantor of the study
Funding The NDDB Foundation for Nutrition (NFN), Anand, India, and the Rural Electrification Corporation Foundation (REC) New Delhi, funded the research project (grant number: BE 153092).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.