Article Text

Abstract
Objective To assess weight loss maintenance, diabetes status, mortality and morbidity 15 years after a very low calorie diet programme (VLCD) in patients with obesity.
Design General practice data bases were interrogated for subjects coded for group therapy with VLCD in the 1990s. Causes of death, occurrence of vascular disease and remission or development of diabetes were ascertained from patient records and national stroke and cardiovascular disease data bases.
Results 325 subjects engaged in the programme and had sufficient data for analysis. Baseline characteristics were: age 47.8±12. 8 years; body mass index (BMI) 36.1±6.8 kg/m2; 79.1% female/20.9% male; 13.5% had type 2 diabetes. After 15±4 years weight had changed from 97.9±19 kg at baseline to 100±20.8 kg. 10 with diabetes at baseline were in remission at 3 months, but only two remained in remission at 5 years. 50 new cases of type 2 diabetes and 11 of impaired fasting glucose developed during follow-up. Only 5.9% who remained healthy at follow-up had maintained >10% body weight reduction. Neither diabetes incidence nor diabetes free survival were related to percentage body weight lost during VLCD. Only baseline BMI was related to development of new impaired fasting glucose or diabetes by 15 years (p=0.007). 37 subjects had a cardiovascular event. Age (p=0.000002) and degree of weight loss after VLCD (p=0.03) were significantly associated with subsequent vascular events.
Conclusion Long-term maintenance of weight loss after VLCD was rare in this single centre retrospective study 15 years later. Glucose intolerance developed in 21.4%. Lasting remission of type 2 diabetes or prevention of later glucose intolerance were not achieved. Vascular events were more frequent in those who lost most weight. Risk management during weight regain should be studied in future to assess potential for reduction in adverse cardiovascular outcomes.
- diabetes mellitus
- weight management
- nutritional treatment
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Many studies have shown successful short-term induction of weight loss in persons with obesity, but long-term weight loss maintenance has been disappointing.
What this study adds
This is the first observational study to report long-term outcomes (15 years) after successful weight loss with very low calorie diet (VLCD).
Weight regain in 95% was associated with vascular events and development of type 2 diabetes.
How this study might affect research, practice or policy
Prospective long-term outcome studies will be required to ascertain whether intensive follow-up of low carbohydrate dietary interventions including VLCD can achieve weight loss maintenance without cardiovascular risk.
Introduction
The central importance of nutrition in development of type 2 diabetes is widely accepted.1–4 Type 2 diabetes results from a combination of beta cell failure and insulin resistance, the latter almost invariably associated with some degree of obesity.5 Population wide weight loss has been associated with a reduction in prevalence of type 2 diabetes. The most recent example of this has been the Cuban experience from 1990 to 2010. As a result of forced austerity from 1990 an average weight loss of 5 kg was sustained in the adult population of Cuba. The prevalence of type 2 diabetes declined over 10 years. This trend was reversed in the subsequent 10 years after the ending of austerity.6 This highlights the possibility that community-based weight loss programmes could reduce the prevalence of obesity and type 2 diabetes.
One recent pharmacy based study has shown maintenance of 10% wt loss at 132 days after intervention with very low calorie diet (VLCD).7 Meta-analysis of successful weight loss with VLCD has confirmed equal success in those with and without type 2 diabetes. Weight loss was better sustained for 18–36 months with a variety of dietary strategies.8 In another study from Scotland, retrospective analysis of weight loss maintenance following VLCD has shown impressive results for up to 3 years.9 However, in this study, only 10% of the participants recruited at baseline were intensively followed up at 3 years, the outcome for the majority-90% is not reported.9 A recent prospective controlled study of VLCD has shown remission of early type 2 diabetes accompanied by resolution of ectopic hepatic and pancreatic fat. This has renewed interest in the concept that a long-term remission in glucose intolerance might be achievable.10 11 These findings have also focused interest in VLCD intervention in the community, in order to reduce future development of type 2 diabetes.12 The high risk of cardiovascular disease associated with long-term obesity might be mitigated if VLCD induced weight loss could be sustained long-term as shown in follow-up of bariatric surgery.13 14
In the 1990s in South Devon, UK, a VLCD formula was made available only with private prescription from the general practitioner. The whole cohort of 351 patients who engaged in the programme were identified and retrospectively assessed for maintenance of weight loss achieved on the programme, subsequent development of diabetes and vascular events.
Methods
Patients with obesity who were prescribed VLCD in the early 1990s, were identified from general practice data and hospital records confirming private prescription of ‘Lipotrim’ (Howard Foundation, Cambridge, UK). The study protocol has been described fully in a previous report.15 Ninety-five per centof the practice populations in 1990 were ethnically White British. The VLCD weight loss programme was advertised in four general practice reception areas, and included in discussions of obesity and health during doctor and nurse appointments. Patients who selected VLCD were required to attend weekly group sessions with a nurse, counsellor and initially a doctor. Weekly meal replacements were issued on completion of each session. Timing of these community-based sessions was arranged to suit participants convenience. The complete nutritional replacement provided 450 kcal (30 g carbohydrate) per day for women and 650 kcal (58 g carbohydrate) day for men. The meal replacements were provided in the form of sachets and flapjacks. The cost to the patient of meal replacement was £18 for females and £24 for males per week, paid weekly. Ten patients on benefits were included in the programme without cost to them. Exclusion criteria were blood pressure >150/90 mm Hg, serum creatinine >120 µmol/L, active retinopathy or neuropathy if living with diabetes, active treatment for cancer or known cardiovascular disease.
A total of 325 of 351 patients who attended the first session completed the programme figure 1. Group sessions of 8–10 took place in general practice and all participants were exposed to the same discussions on nutrition and practicalities of total meal replacement with VLCD. Group cooking demonstrations and group discussions to focus healthy eating on cessation of the VLCD programme were included in the programme. Medications for diabetes and hypertension were stopped during the first week of treatment and weight, blood pressure, urinary ketones and blood glucose measured weekly.

Outcome at 15 years follow up of very low calorie diet therapy. BMI, body mass index; VLCD, very low calorie diet.
Permission was granted by the Primary Care Trust and the four general practices involved in the VLCD programmes in the 1990s to audit 15-year outcomes. Records of patients with obesity who received private prescription of the VLCD formula ‘Lipotrim’ (Howard Foundation, Cambridge, UK) were searched to document age, gender, baseline and final diabetes status, baseline weight and body mass index (BMI). Weight loss in the 3 months after commencing VLCD (or during total time on VLCD if longer than 3 months), weight regain and 15-year weight (final weight was used if patients had deceased earlier) were also ascertained. Practice diagnosis of type 2 diabetes during follow-up was confirmed from records by Haemoglobin A 1c (Hba1c) ≥48 mmol/mol (6.5%) or fasting serum glucose ≥7 mmol/L (126 mg %); and impaired fasting glucose (IGT) with serum glucose ≥6 but ≤7 mmol/L (108 to 126 mg %). Morbidity and mortality were ascertained from practice records and confirmed through Heart: Myocardial Ischaemia National Audit Project (HQIP/A-Z of National Clinical Audits/Heart: Myocardial Ischaemia National Audit Project).16 Reported stroke and heart failure were identified from practice records and confirmed from hospital records. The data were anonymised before analysis.
Statistical methods
The Kaplan-Meier method and Cox proportional hazard models were used to estimate overall survival and type 2 diabetes free survival. Time from the end of VLCD intervention was used as time 0, and censored at date of death or development of type 2 diabetes. All data were analysed in ‘R’ open software V.1.2.5019.
In addition, a binomial modelling approach was used to identify factors associated with development of IGT or diabetes and identify factors associated with the development of cardiovascular events (atrial fibrillation, acute coronary syndrome, congestive cardiac failure and stroke).
Results
Numbers of records searched, those excluded and diabetes status after 15±4 year are depicted in figure 1. All were of white British ethnicity. A total of 3713 adults on the combined general practice lists were obese in 1995. Between 1995 and 2010, obesity and diabetes prevalence in the combined practices increased from 11.7% to 27% and 3.1% to 5.1%, respectively.
Table 1 describes the characteristics of whole cohort and subgroups according to baseline and incident glucose intolerance status. Baseline and follow-up weights in each of these subgroups can be seen in table 2.
Baseline characteristics of 325 subjects undertaking very low calorie diet programme between 1993 and 1998 in South Devon, UK
Weight changes in 325 subjects in the 15 years following a VLCD treatment programme
Ten of the 44 patients with baseline type 2 diabetes normalised blood glucose levels after the VLCD treatment at 3 months (weight reduced from 103±24 to 89.5±21 kg, serum fructosamine reduced from 336±56 to 258±25 mmol/L). Weight and serum fructosamine at 3 years increased to 103±30 Kg, and 349±68 mmol/L, respectively. Only two sustained remission at 5 years, and none at 15 years. Full details shown in online supplemental table 1.
Supplemental material
55 patients achieved >10 kg weight loss at 15 years follow-up: Of these four had undergone bariatric surgery, three had poorly controlled diabetes, six developed terminal cancer, three were in severe heart failure, two suffered severe strokes and one was living with dementia, (online supplemental table 2.
Supplemental material
Thirteen of 220 with no diabetes at any time and who remained in good health maintained 10% wt loss at 15 years representing a 5.9% wt loss maintenance associated with intervention with VLCD 15 years before.
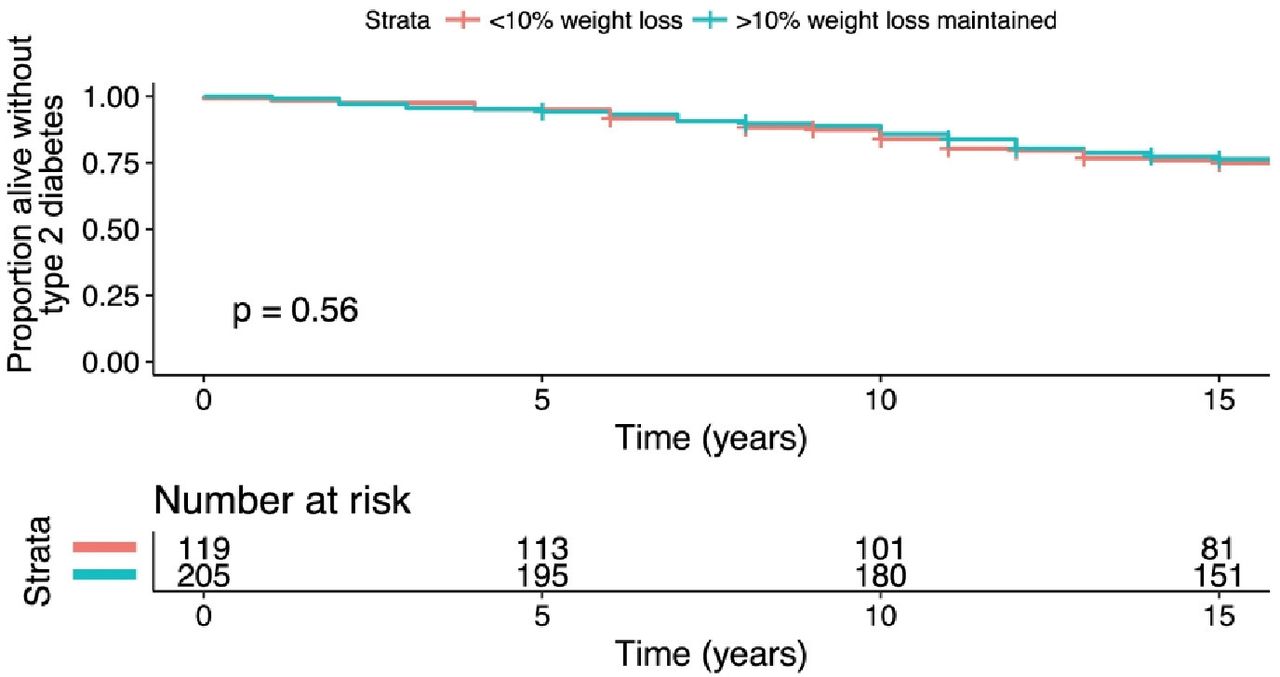
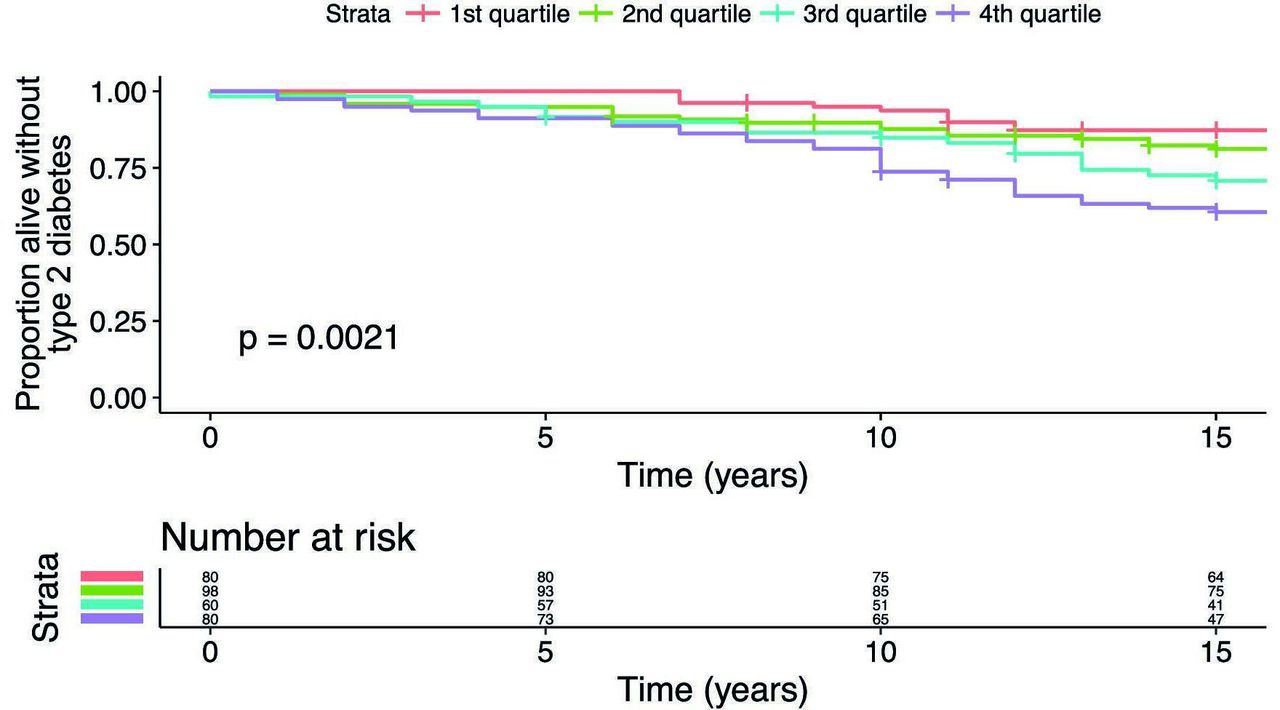
The binomial model result included covariance of weight, BMI change, gender, baseline BMI, weight difference by 15 years and age on the development of IGT or diabetes. In the 281 patients without baseline diabetes the results were: null deviance: 292 on 276 degrees of freedom Z value: 2.6. All terms were rejected by the model except baseline BMI, which maintained a significance of p=0.007 see figure 2. Outcomes are expressed as quartiles of baseline BMI. Diabetes free survival was not associated with percentage of baseline body weight lost during the VLCD intervention, or at the end of the study, see figures 3 and 4.
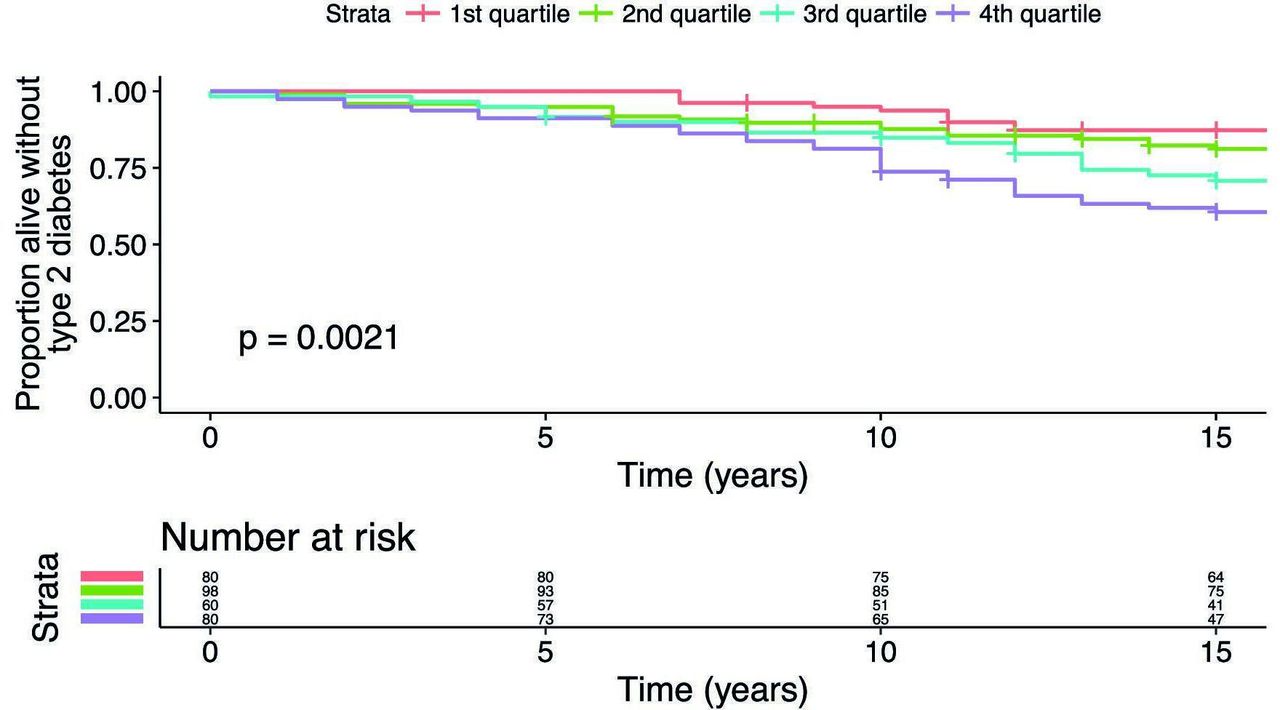
Survival free from type 2 diabetes mellitus following weight loss in lipotrim study, Stratified by quartile of baseline BMI. BMI, body mass index.
Survival free from type 2 diabetes mellitus following weight loss in lipotrim study, stratified by weight loss <10% versus weight loss >10% during lipotrim study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival free from type 2 diabetes mellitus following weight loss in lipotrim study, stratified by weight loss <10% versus weight loss >10% maintained by study end.
Factors associated with cardiovascular outcomes (stroke, atrial fibrillation, coronary artery disease, congestive cardiac failure) in binomial modelling of the whole cohort of 325 patients with obesity were baseline age (p=0.000002) and weight lost during VLCD (p=0.03). The mean (±SD) characteristics were: age in years 57.7 (±8.2); weight in kilograms at baseline 109.8 (±14.9); weight loss on VLCD 18.2 (±9.1); final weight 117.9 (±20.9). 21 were female 16 male, 8 had diabetes at baseline and 12 developed diabetes. Events occurred 9.2±4.3 years after VLCD.
Weight loss achieved on the VLCD programme was significantly related to baseline BMI, r=0.1323, p=0.017 for those with any diabetes, baseline or incident diabetes, and r=0.1244, p=0.0005 for those with no diabetes online supplemental figure 1—).
Supplemental material
Discussion
In this 15-year follow-up of one intervention with VLCD, 55 patients sustained >10 Kg weight loss at follow-up, but a number of confounding factors have contributed to final weight achieved in many of them. Fifteen had serious or fatal illness, three had poorly controlled diabetes and others undertook later weight loss interventions such as bariatric surgery (three) or other meal replacement programmes (four). It is internally consistent but not surprising that weight loss on the VLCD programme was related to baseline BMI as the intervention involved fixed caloric intake of 450 kcal/day for women and 650 kcals/day for men.
Fifteen years after intensive VLCD intervention 21.4% of those without baseline diabetes developed type 2 diabetes or impaired fasting glucose during follow-up (50 type 2 diabetes; 11 impaired fasting glucose). This compares with the results of the EPIC study, an ethnically similar group, showing a 10-year diabetes incidence of 5.3% with baseline BMI 26 and age range 25–75 years.17 The National Health and Nutrition Examination Survey, study of self-reported weights over 8 years in North American female healthcare workers those aged 59 years with higher BMI 35–40 Kg/M2 the cumulative incidence of type 2 diabetes was 43%.18 A Cochrane review of bariatric surgery trials the cumulative incidence of diabetes in control subjects was 25.8%.19 In the Swedish Obesity Survey control group the 15-year incidence of diabetes was 21.9%.20 In the Whitehall study analysis at 14 years in civil servants aged 52 years with 75% male gender and baseline BMI of 29, 9.7% developed type 2 diabetes by follow-up.21 The figure of 21.4% glucose intolerance in our group is broadly comparable to diabetes rates in these studies allowing for differences in baseline BMI and gender.
There was no correlation between weight loss during the VLCD programme and final weight loss, or with development of diabetes. In this respect the analysis of incidence of diabetes and vascular disease in Cuba from the 1980s until 2010 is relevant. The population effects of weight reduction over 10 years were lost with weight regain, though the outcomes for individuals who lost most weight during austerity is not known.6 None of our patients had clinically manifest renal or cardiac disease, sight threatening retinopathy or neuropathy at baseline. Nevertheless the 15-year vascular outcome was poor in our patients with either baseline or incident type 2 diabetes. This was despite the temporary remission in obesity. The Look Ahead study which included partial meal replacement with low calorie products to induce weight loss in type 2 diabetic subjects failed to demonstrate reduction in vascular events.22 Analysis of the Framingham data has shown an increased mortality among participants whose weight varied substantially during follow-up suggesting a harmful effect of so-called yo-yo dieting.23 The association of cardiovascular events with greater weight lost during VLCD in this study requires further investigation in randomised prospective studies. All of these participants not only regained weight but many exceeded their baseline weight by 15 years. This large increase in weight would inevitably result in development of adverse cardiovascular risk. Study participants with similar age, gender and ethnicity to those in our study showed significant associations of weight regain with glucose intolerance, hypertension, hyperlipidaemia and mental ill health 5 years after bariatric surgery.24
Advantages of this audit are that it reflects the outcome in a high proportion of obese individuals who undertook a standardised total VLCD meal replacement programme over a short time period in one area of the UK. In addition, all received the same support video, advice on re-feeding and exercise. As the programme was delivered in the local community it was possible to arrange group session times for patient convenience. The limitations are that the cohort is exclusively of white British origin, reflecting the local population demographic. Other ethnic groups have a higher incidence of cardiovascular disease and lower BMI threshold for the development of type 2 diabetes.25–29 VLCD trials in this and other ethnic groups should be undertaken to establish risks and benefits before large scale interventions are undertaken.
There is a potential source of bias in that the patients were required to purchase the meal replacements on a weekly basis by private prescription and were willing to attend group sessions. However, weight loss programmes delivered in the community are commercially based and extremely popular with evidence of short term success30 (https://www.weightwatchers.com, www.slimfast.co.uk, www.slimmingworld.co.uk). More work would be welcome to evaluate the comparative efficacy of weight loss strategies as purchased meal plans or a prescribed free therapy, particularly as the majority of persons with obesity seeking support in losing weight in the community will do so by engaging in proprietary weight loss programmes. It is of interest though not generalisable that all the 10 patients with obesity whose prescriptions were offered free because of financial difficulty failed to engage beyond the first week (the 10 subjects in figure 1 ‘failed to collect prescriptions’).
The lack of evidence that this intense VLCD programme induced lasting remission in type 2 diabetes or significantly reduced incidence of glucose intolerance is disappointing but not surprising as weight regain occurred in 95%. Only 8.7% of patients with obesity in the combined practice lists undertook the VLCD programme. These findings highlight the challenges in engaging patients at risk of serious ill health in this case due to obesity. This also constitutes a bias in that the majority of persons with obesity not included in the programme may have responded differently to VLCD and had different rates of development of diabetes. The precise outcomes for the non-participating persons with obesity is not known.
Better engagement of patients with type 2 diabetes and good outcome at 2 years has been achieved with low carbohydrate diet (28.7%) in a single-centre study with the crucial difference that VLCD (which can be considered as a prescribed low carbohydrate diet) replaces usual food as a short intervention, while a low carbohydrate diet modifies food intake and can therefore be continued long term.31 A recent metanalysis of dietary carbohydrate restriction in treatment of type 2 diabetes has emphasised the inter-relationships between total energy restriction, VLCDs, and focused low carbohydrate diets.32
It is likely that the combination of obesogenic environment, availability of high energy dense ‘junk food’ and food addiction will all have played a part in the development of obesity at baseline, and weight regain after VLCD experienced by the subjects in the study.33 34 Future meal replacement studies to induce remission in or prevent type 2 diabetes might result in longer term weight loss maintenance if effective post-VLCD lifestyle intervention strategies such as those employed in the diabetes prevention programmes were implemented.35 A cogent case for integrated care in obesity treatment has been proposed.36 This comprehensive review of tier 2 (community-based lifestyle intervention) and tier 3 (specialist weight management services) concludes that their efficacy remains uncertain. Difficult access to treatment for obesity, poor outcomes of intervention, rigidity in pathways and weight stigma are cited as continuing barriers. Facilities to deliver such a multifaceted intervention were not available at the time of our study This contrasts with the positive metanalysis of short term success of VLCD intervention in patients with type 2 diabetes in 2015.37
More options are becoming available for long-term weight loss maintenance. Excellent sustained weight loss has been demonstrated in a recent randomised controlled study of a weekly Glucagonlike Peptide Agonist (GLP1 agonist) in population with obesity.38 Currently, this would be an expensive option for weight loss maintenance for very large numbers of obese persons. The efficacy of low carbohydrate diets in long-term weight loss has been demonstrated particularly in insulin resistant individuals in single-centre cohort studies.39 Randomised long-term studies of a range of low carbohydrate diets designed to evaluate sustained weight loss and cardiovascular outcomes are much needed. Randomised controlled studies of bariatric surgery have unequivocally demonstrated substantial reduction in obesity, severity and prevalence of diabetes. The rarity of substantial weight regain post bariatric surgery is likely to contribute to the reduction in cardiovascular events,40 while the long-term effects of low carbohydrate diets (including VLCDs) on cardiovascular outcomes are only beginning to be tested in prospective studies.31
Conclusion
To our knowledge, this is the first report of very long-term outcome following VLCD with over 90% follow-up. Of a total of 325 subjects, only 5.9% who remained healthy sustained >10 kg weight loss at follow-up. Neither sustained remission in diabetes, nor an effect on incident diabetes were achieved. The higher incidence of cardiovascular events in those who lost most weight during VLCD requires further investigation. The effect on long-term outcomes after VLCD of intense multidisciplinary follow-up and cardiovascular risk management have not been reported. Finally, a reflection on the results of this and many other weight loss interventions would suggest an urgent need for prevention of development of type 2 diabetes in those with pre-diabetes,35 41 42 and public health strategies to reduce population levels of obesity, though these latter interventions have so far met with only limited success43
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Torbay Local Research Ethics CommitteeTorbay Hospital,Lawes Bridge,Torquay TQ27AA1992 ref T19/11/92 Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The VLCD programme was set up commercially and supported by Dr S Kreitzman PhD, Biochemist and V Beeson, Nurse practitioner of Howard Foundation Ltd. Practice groups were run by practice nurse leads for diabetes Stacey Fricker, Jane James, Karen Rundle and Sue Finch. This work has been presented in part as a poster at the Association of British Clinical Diabetologists meeting Manchester UK on 22 April 2016. We would like to thank Beverley Coombes for expert assistance in validating cardiovascular outcomes through the national cardiovascular disease and stroke data bases. Melvin Cowie, graphic design, undertook formatting of the figures. Above all we are grateful to the subjects who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RiP initiated the study and led the audit. CD, WH, RB and DG organised the practice based groups and collated practice data for the audit. JF and RoP managed the patients living with diabetes and contributed to writing up the manuscript. CP performed statistical analysis and contributed to referencing and writing up the manuscript. RiP is guarantor for the study.
Funding Torbay Special Medical Projects grant PS/MAO/T/PAIS001. Torbay Hospital and the practices facilitated the audit. Transparency of data is confirmed and data sharing acceptable.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Submitting author R Paisey is guarantor and responsible for supplying source data on reasonable request
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.