Article Text

Abstract
Introduction 15% of all presentations to our emergency department last year were chest pain related. This presented an opportunity to evaluate the impact of a brief physician counselling intervention on patient-reported changes in cardio-protective foodstuff intake.
Methods This is a prospective non-randomised before and after comparison study without controls, conducted between an emergency department presentation and a scheduled follow-up visit at a cardiac diagnostics department. Participants were recruited between February and March 2021. The selected dietary components for inclusion after review of the literature were green leafy vegetables, other coloured vegetables, wholegrains, legumes and fruits. A food frequency questionnaire was completed by patients before and after a physician counselling intervention aided by a dietary infographic. Additionally, using the transtheoretical model for health behaviour change, we assessed each patient’s evolution during the study.
Results 38 patients were recruited. For patients with total baseline consumptions of five or fewer per day, there was an increase in cardioprotective foodstuff intakes (z=−2.784 p<0.005 effect size 0.39). Corresponding to this, there was a participant shift observed towards the action and maintenance phases of behaviour change from the contemplation and preparation phases.
Discussion We demonstrated a statistically significant change with moderate effect size using a simple infographic, coupled with brief physician counselling, to promote increased intake of cardioprotective foodstuffs by patients with poor baseline intakes (<5 cardio-protective foods per day) and known modifiable risk factors for ischaemic heart disease.
Conclusion Diet is one arm in the prevention of cardiovascular disease that is often neglected by physicians. This study found that a brief dietary counselling intervention applied in an emergency department setting, administered by non-nutritionists can have a role in changing patient dietary behaviour.
- Nutritional treatment
- Nutrition assessment
- Malnutrition
- Dietary patterns
- Preventive counselling
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
There is growing evidence in favour of plant-based nutrition and health behaviour change counselling to empower patients and their physicians to turn the tide on cardiovascular disease.
This research found that a brief counselling intervention coupled with a dietary prescription given by emergency medicine physicians can increase patient intake of cardioprotective foodstuffs with moderate effect size (z=−2.784, p=<0.005, r=0.39).
Emergency department presentations provide a unique opportunity to engage patients in lifestyle change. Future studies should be considered in this setting.
Background
Coronary artery disease has been described as the number one killer of women and men in the western world.1 As populations age, its prevalence is forecast to increase along with the associated costs to society.2 Prevention and early intervention must be the focus to ameliorate this trend. One way to do this is through diet as well as other well-established interventions such as smoking cessation and exercise.
Inverse associations between vegetable protein and coronary artery disease have been previously described.3–5 Okinawa, Japan, for example, has one of the lowest rates of mortality due to cardiovascular disease and is a leading area for longevity in the world. Their vegetable intake is high and their sodium, total fat and total calorie intakes are low (plant-based diets are nutrient dense but calorically dilute).6 7
In a study of 40 countries, calories obtained from vegetable foods were negatively correlated with coronary artery disease mortality (r=−0.80, p<0.001).8 Another study spread over 52 countries found significant inverse associations between higher intakes of raw or cooked vegetables (OR 0.68 (0.60–0.77)), green leafy vegetables (OR 0.69 (0.60–0.78)) and fruit (OR 0.70 (0.63–0.79)) with acute myocardial infarction.9
Persons consuming eight or more servings of fruit and vegetables daily can achieve a 20% lower risk for coronary artery disease (0.80, 0.69–0.93) than those eating less than three servings per day. The strongest effects are seen from green leafy vegetables and vitamin C-rich fruit and vegetables.10 Increase in combined fruit and vegetable intake to six or more portions per day improves vascular function, resulting from increased plasma nitric oxide and reduced vascular adhesion molecules.11 Plant-based foods reduce oxidative stress and inflammation in the body. They reduce blood pressure and are high in minerals and fibre while being low in saturated fat and containing no cholesterol.12 13
There are many more such studies describing other dietary components independently associated with lower risk of coronary artery disease, namely, green leafy vegetables, other coloured vegetables, whole fruit, whole grains and legumes.14–21
For overall health, a deficit of plant-based foods in the diet is concerning as mortality rate increases of over 50% have been demonstrated in individuals consuming no fruits and vegetables compared with those eating five servings of fruits and vegetables each day.19 In the USA, the Department of Health has identified a number of shortfall nutrients and its guidelines recommend increased intake of dark green and yellow vegetables, fruits, legumes, whole grains, nuts and seeds to address this.22
Doctors have little training in nutrition or behavioural modification, yet attention to diet from a patient’s physician can empower them to become the locus of control for their own disease management.23 To aid risk factor modification, it is important to actively promote a high-quality diet for our patients.24
In recent years, interest in theories and models of behaviour change has grown .25 These theories and models consider a wide range of factors such as emotions, habits and routines. They can support interventions by describing how behaviours develop and change over time. There is a strong body of evidence that using these theories in the design and implementation of interventions increases their effectiveness .26 One of the most commonly applied theories is the Transtheoretical Model.27
This model acknowledges that health behaviour change is difficult and that individuals go through several phases when faced with the dilemma of change. The default psychological position is to retain the status quo. The change stages described are: precontemplation (no intention to change behaviour), contemplation of changing behaviour in the future, preparation to change behaviour more immediately (and already making small steps in that direction), actioning of the new behaviour, maintenance of the adopted behaviour and finally relapse (no longer maintaining or struggling to maintain the change). The model also recognises that people can go back and forth between the stages at different times in their lives, so it is very much a dynamic living process.
We propose that an acute presentation with chest pain presents an opportunity for healthcare providers to engage with patients in dietary change. Here, we evaluate the impact of brief physician counselling in line with the transtheoretical model of behaviour change using a dietary infographic on patient-reported change in cardioprotective foodstuff intakes. To our knowledge, this is the first study to evaluate the effect of a prevention-focused nutrition counselling intervention in an emergency department setting.
Methods
Study design, study setting and study population
This is a prospective non-randomised before and after comparison study without controls, conducted between an emergency department presentation and a scheduled follow-up visit at the cardiac diagnostics department. The hospital setting was that of a University Teaching Hospital.
Our emergency department uses a Chest Pain pathway to standardise care of patients who present with chest pain concerning for a cardiac aetiology.
This pathway stratifies patients into three groups: low, medium and high risk according to the well-established History, Electrocardiogram, Age, Risk Factors and Troponin (HEART) score for major cardiac events. The score achieved is a composite of the physicians’ interpretation of signs and symptoms backed up by the results of ECG and blood investigations.28
This research focused on consecutive patients who were discharged from the emergency department and scheduled to attend for urgent ambulatory cardiac diagnostics in 1 week. The reasons for focusing on this group were: first, these patients have known risk factors for cardiovascular disease which can be modified by diet and second, by being sent back to their own home environment, behaviour modification out of the hospital setting can be implemented.
All patients who fulfilled inclusion criteria during the study period were given the opportunity to take part. All emergency medicine physicians were involved in recruitment and dietary counselling ensuring good 24 hour cover 7 days a week during the study period.
Inclusion criteria
Low-risk chest pain of suspected cardiac aetiology.
Adult patients (16 years old and above).
Known risk factors for coronary artery disease.
Planned to represent for urgent ambulatory cardiac diagnostics.
Exclusion criteria
Persons with a body mass index <18.5 or eating disorders were not included on the grounds of safety (no such persons were detected in the recruitment for this study).
Brief intervention and assessment
The brief intervention consisted of physician counselling in line with the transtheoretical model of behaviour change using an infographic whose content was derived from a review of the background literature. This indicated the dietary components that have been associated with reduction of cardiovascular disease risk.14–21
Study questionnaire
The questionnaire (online supplemental figure 1) was piloted prior to use and designed with a variety of literacy levels in mind with text being accompanied by images (online supplemental figure 2) and allowing free text inputs, so that patients could express intake in quantity per day, per week or per month. Frequency of consumption was later standardised to times per day for data analysis. In addition to this, we also assessed each patient-reported stage of health behaviour change at both visits during the study (online supplemental figure 3) based on the transtheoretical model.
Supplemental material
Supplemental material
Supplemental material
Emergency presentation
At this initial visit, patients who satisfied inclusion criteria and consented to participate were given the food frequency questionnaire to fill out while they awaited their standard blood tests. Participants were then provided with the infographic in the style of a prescription (online supplemental figure 4) by their doctor who would briefly review its recommendations verbally with them to encourage uptake of the advice. The infographic also directed participants to established national healthy eating resources for more information (online supplemental figure 5).
Supplemental material
Supplemental material
Planned cardiac diagnostics visit
One week later, patients were asked to complete follow-up (identical) questionnaires while in the waiting room for their diagnostic procedure by technicians not connected with the study.
Statistical analysis
The analyser of the data was blinded to study participant details.
Sample size determination
Using a confidence level of 95%, an SD of 3 and error set at 1, we determined a minimum sample size of 35 participants would be required.
Statistical methods
SPSS V.26 (SAS Institute, Cary, North Carolina) was the package employed for our statistical analyses.
To compare food frequencies reported pre and postintervention in the study group, we used Wilcoxon signed ranks test. To compare stage of health behaviour change before and after counselling intervention, we used Fishers exact test. Statistical significance was defined as p<0.05.
Results
This study consisted of 38 participants (55% men, n=26) with a mean age of 57 years (SD=2) and an age range of 30–81 years. The participants were recruited over a period of 2 months between February and March 2021.
A minority of study participants (n=12) reported consuming greater than five of the study foodstuffs per day at baseline.
Changes in intakes post-intervention
Including our baseline high performers consuming more than five study foodstuffs per day (n=38), there was no statistically significant increase pre and postintervention. Mean total intake pre-intervention=4.7537 (SD=1.77085) and 5.3224 (SD=2.44031) post-intervention. Z score=−1.067, p=0.29.
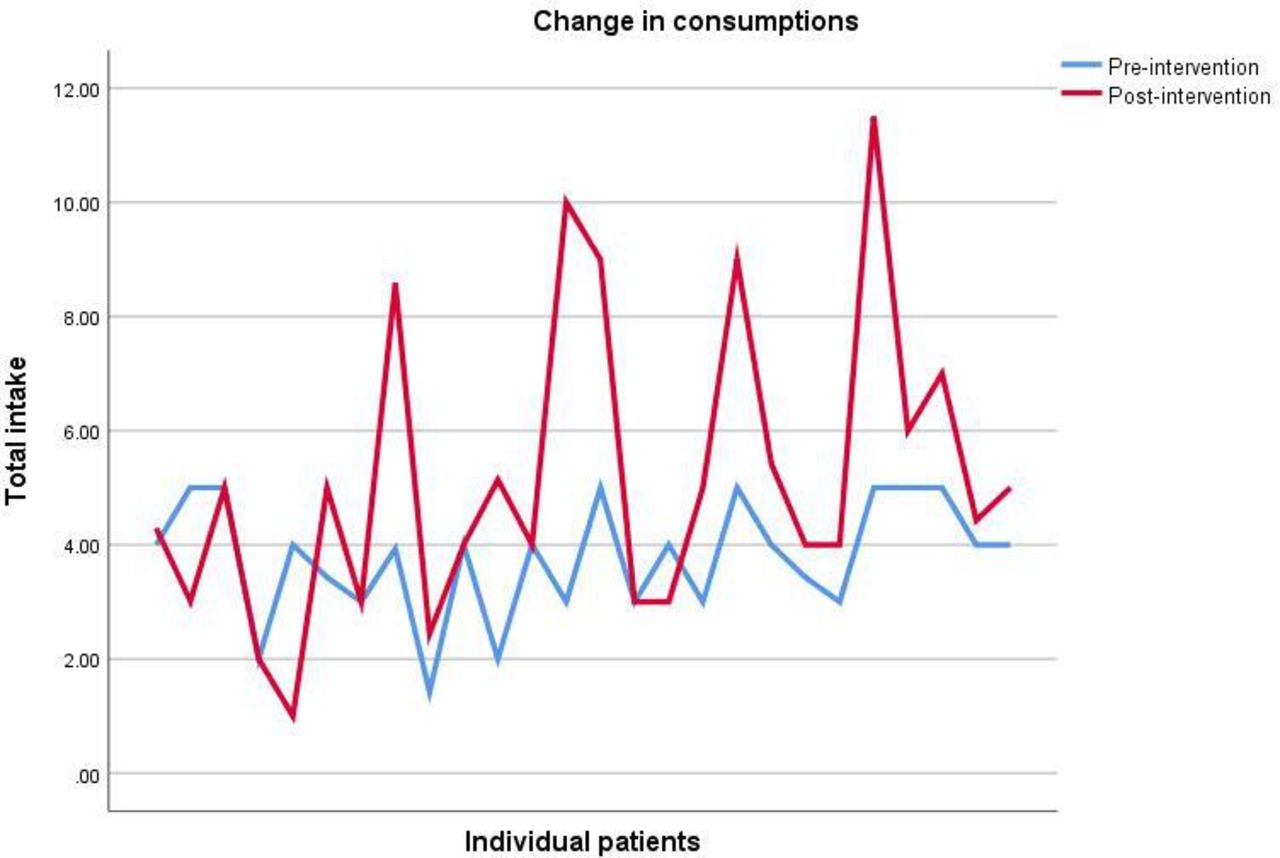
For the lower performers in the study with total baseline consumptions of five or fewer per day (n=26), mean total intake pre-intervention=3.7773 (SD=1.020) and 5.1469 (SD=2.60040) post- intervention were significantly different. Z score=−2.784, p=0.005, r=0.39 effect size. These changes are visually depicted in figure 1.

Visual depiction of change in consumptions for study participants (n=26) consuming five or less per day at baseline.
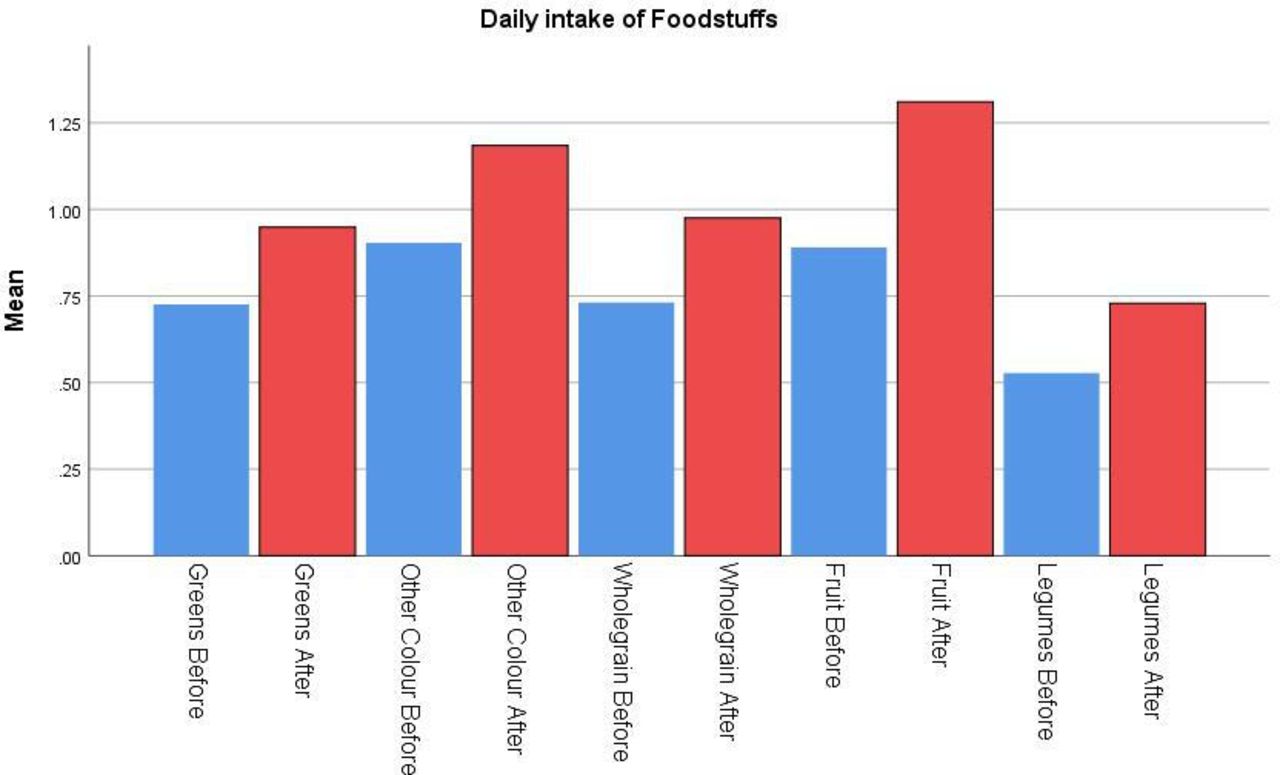
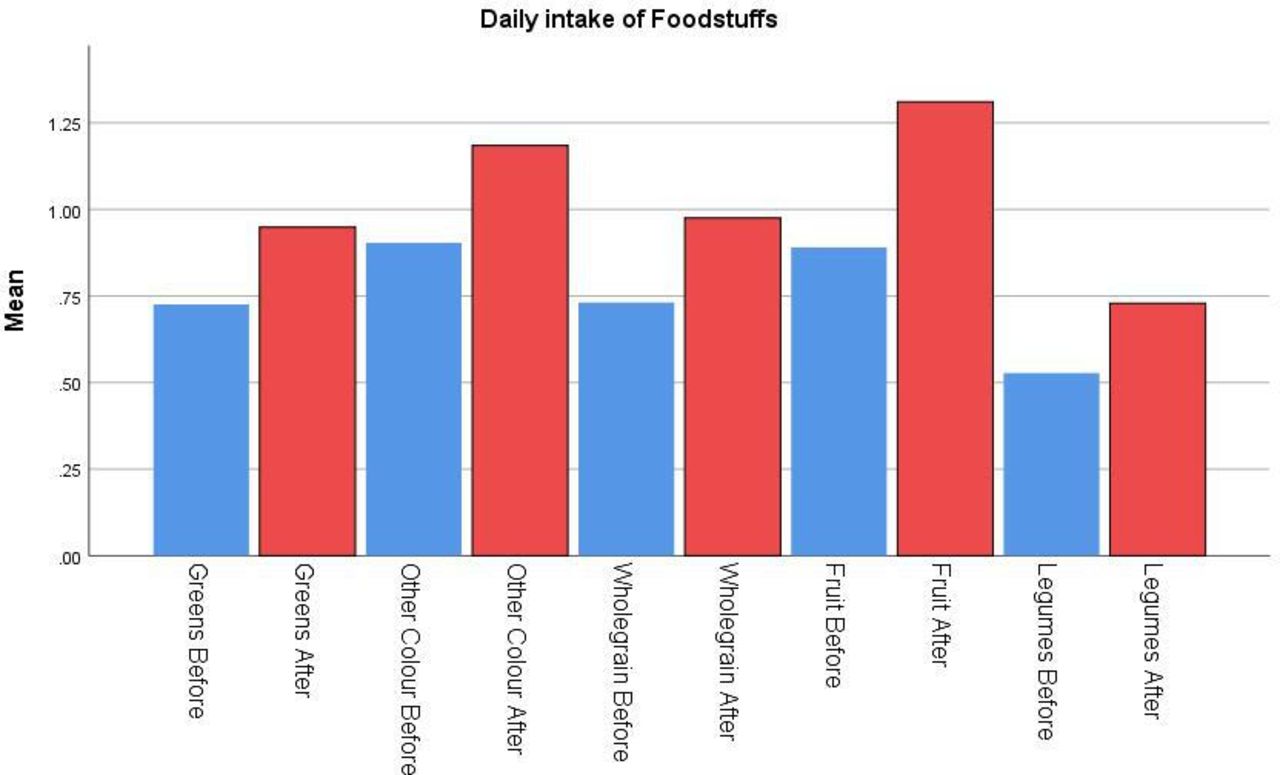
No individual food group investigated made up a majority influence on this change in total intake (figure 2), and there were no significant differences observed by gender.
{kind=link}
{kind=link}
Details of intake change by study food group in participants consuming five or less per day at baseline. No one food group made up a significant majority impact on the overall change observed (p>0.05).
The number of persons in the action and maintenance stages of behavioural change increased post the initial visit counselling intervention (n=5 to n=12, Fishers exact test p<0.007). This corresponded with a decrease in the number of persons in the contemplation and preparation stages of behaviour change (n=16 to n=9, Fishers exact test p<0.005). Four participants remained in the precontemplation stage throughout the study. One of the participants remained in the relapse stage.
Discussion
We proposed that an acute presentation with chest pain presents an opportunity for healthcare providers to engage with patients in dietary change. We evaluated the impact of brief physician counselling using a dietary infographic on patient-reported change in cardioprotective foodstuff intakes. We demonstrated a statistically significant change with moderate effect size using a simple infographic, coupled with brief physician counselling, to promote increased intake of cardioprotective foodstuffs by patients with known modifiable risk factors for ischaemic heart disease who have poor baseline intakes (<5 cardioprotective foods daily). We also showed a participant shift towards the action and maintenance phases of behaviour change from the contemplation and preparation phases.
To our knowledge, this is the first study to evaluate the effect of a cardioprotective nutrition counselling intervention in an emergency department setting. The effect observed here is similar to other brief health promoting interventions in the literature and those encouraged by established guidelines relating to exercise, alcohol intake and smoking cessation.29–32 We further highlight the role of brief opportunistic interventions during healthcare contacts as a measure to help deal with the epidemic of chronic lifestyle-related diseases affecting society.
Men can be particularly difficult to engage in health behaviour change.33 Previous successful health promotion initiatives have focused on male-specific interventions delivered in settings where they present, for example, football clubs.34 While men use general practice and preventative health services less frequently than women, they use hospital emergency departments more frequently, providing another potential setting for intervention. Our cohort was mainly men and we observed significant improvements in cardioprotective foodstuffs which is encouraging and further demonstrates the potential for incorporating a brief intervention in the acute healthcare setting.
We followed the transtheoretical model in this study. Behavioural change is a complex process and people can move back and forth through its phases over long periods of time.35 As a result of this, health behaviour reinforcement at every opportunity is necessary to ensure individuals progress in the desired direction or are guided back on course towards positive change where that is necessary.
Simple dietary counselling should occur, where possible, at all engagements with healthcare professionals. Underlying this is a key tenet: that modern healthcare systems must enable change in population behaviour from being passive recipients of healthcare to actively partaking in the creation of health.36 This is a necessary paradigm shift if we are to turn the tide on the epidemic of chronic disease, which is burdening healthcare systems worldwide.
Recommendations for health promotion are more easily conveyed to patients when they are based on patterns of food intake (promoting or avoiding certain foods) rather than on specific nutrients.9 Diet is one arm in the prevention of cardiovascular disease that is often neglected by physicians.23 It is imperative this change as physicians are core caregivers in the patient journey.
This study has several strengths. We minimised selection bias by consecutive sampling. The food frequency questionnaire used had face validity. Response bias was minimised by technicians not involved in the study giving the participants their follow-up food frequency questionnaire to complete. To minimise ascertainment bias around the initial questionnaire, physicians were instructed that the questionnaires were to be filled out by the patient prior to counselling and infographic administration. The physicians conveyed simple dietary information using an infographic to increase the intake of plant-based foodstuffs, which do not have cautious daily caloric intake limitations. The analyser of the data was blinded to patients involved. The variety of participant baseline intakes depicts a wide spectrum of the population rather than just those with an already established interest in healthy eating.
Good external validity was achieved by performing this study in an emergency department setting with emergency physicians who had no background in clinical nutrition.
Limitations included a lack of a control group in the intervention. In addition, we focused on reported overall dietary pattern change rather than portion size recorded in food diaries, so this study cannot assess the dietary change which occurred in detail. Nuts (which also have known health benefits) were not included as there is more nuance to their consumption than could be addressed by this study. Nut portion size can have a significant impact on calorie intake. This study’s focus was to get patients thinking more about their diets and dietary health behaviour change, rather than providing detailed dietary plans. As part of the study, they were directed to an abundance of open access healthy eating material commissioned by official sources locally (online supplemental figure 5). Sample size limited a detailed assessment of the contribution made by individual foods to the overall increase pre and postintervention.
Although the results are indeed promising, we consider the current study to be exploratory and further study in a larger group of patients and with the inclusion of a control group would provide more clarity on effect size and generalisability of results.
Conclusions
This study indicates that a brief dietary counselling intervention in an emergency department setting, administered by non-nutritionists, may have a moderate effect in changing patient dietary behaviour, where poor baseline intakes of cardioprotective foodstuffs exist.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Sligo Research Ethics Committee. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
All Emergency Medicine Physicians at Sligo University Hospital, Republic of Ireland.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design: RM and LK. Acquisition of data: AAR. Statistical analysis: RM. Drafting of the manuscript: all authors. Revision of the manuscript: all authors. Guarantor: RM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.