Article Text

Abstract
Background Vitamin D delivered transdermally may suppress hyperactivity in nociceptor pain receptors and alter pain intensity, offering a useful addition to localised pain management in varying clinical settings. Currently, little is known about long-term usage of continuous-release vitamin D patches.
Method We conducted a randomised parallel pilot trial to evaluate safety and tolerability of daily application of patented (US8821921B2) transdermal vitamin D patches over 8 weeks and assess time-level profile of serum vitamin D. Compliance, tolerance and sun exposure were monitored daily, serum 25(OH)D measured 2-weekly and dietary intake and safety markers 4-weekly.
Results Thirty healthy adults were randomised to two treatment groups: big patch and small patch. mean age was 36 years (20–68 years) with a 63% female to 37% male split. Patches differed in size but contained identical ingredients including 30 000 IU cholecalciferol. Physical and blood safety markers remained stable, within normal clinical parameters, and with no clinically meaningful changes throughout. Five big patch participants experienced skin irritation, which was mild and occasional for three, but continuous for two leading to patch withdrawal. There were no skin reactions in small patch group. average, serum 25(OH)D levels increased by +14 nmol/L (SD 11.63, range, −4 to 40 nmol/L) between baseline and week 8, with no significant differences between patch sizes. There was a shift in overall vitamin D status between baseline and week 8 (23% deficient (<30 nmol/L) decreasing to 0%, and normal (>50 nmol/L) increasing from 37% to 70% at week 8).
Conclusion Based on these results, long-term (8 weeks) application of patented transdermal vitamin D patches was found to be safe. There may be minor skin tolerance issues with big patches for some, which appears to relate to patch size. Larger trials are warranted to explore the increase in vitamin D levels beyond 8 weeks.
Trial registration number NCT04851990.
- musculo-skeletal health
- nutritional treatment
- nutrient deficiencies
- precision nutrition
Data availability statement
Data are available upon reasonable request. Data available on reasonable request from corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Vitamin D is systemically absorbed when applied to the skin, but blood level–time vitamin D profile with daily application of vitamin D patches has not previously been explored.
WHAT THIS STUDY ADDS
Daily application of patented patches containing vitamin D3 is safe and well tolerated by most healthy adults over an 8-week period. Serum 25(OH)D levels increased but remained within safe parameters and vitamin D status improved in all participants.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Daily application of vitamin D patches has been shown to be safe and well tolerated by most individuals. Larger scale trials are now warranted to further explore the efficacy of transdermal delivery of vitamin D for both vitamin D status and nociceptive pain relief.
Introduction
Vitamin D is the subject of wide-ranging research into the relationship between intake, status and overall health outcomes.1 Vitamin D3 (cholecalciferol) is formed in the skin following exposure to UltravioletB (UVB) light and occurs naturally in a limited range of foods or may be added through fortification. Regardless of source, vitamin D is processed by the body to become physiologically active 1,25-dihyroxyvitamin D.
Adequate vitamin D is important for skeletal health, immune function and suppression of inflammatory response.2 Interest is developing into the role of vitamin D in pain management as supplementation may decrease pain scores and improve chronic pain.3 Both observational and intervention studies support this altering of pain intensity, making vitamin D a potentially useful addition to pain management in varying clinical settings.4–6
Vitamin D acts on nociceptor pain. Nociception is the stimulation of sensory nociceptor nerve cells by chemical (a classic example is capsaicin found in chilli peppers), mechanical (cutting or crushing) or thermal (heat and cold) stimuli, which produce pain signals.5 7 Vitamin D acts on the transient receptor potential vanilloid 1 pain receptors, helping prevent hyperactivity of these receptors in chronic inflammatory conditions such as arthritis, or in soft tissue injuries, thus reducing pain.4 5
Transdermal (via skin) therapeutics such as salves, ointments and patches have been used since ancient Egyptian and Babylonian medicine (around 3000 BC).8 Routine use of transdermal drug delivery systems has only become common practice in the latter part of the 20th century with the advent of delivery technology capable of precise and reproducible administration through the skin for systemic effects.8 Potential efficacy and suitability of patch drug delivery is normally determined by blood level–time profiles for the active components.
Vitamin D3 is lipophilic with a half-life of around 15 days and enters the circulation following application to the skin; however, little is known about its blood level–time profile via this route.9–11 Topical application of D3 (5000 IU in aloe vera gel) has been shown to raise serum levels after 4 months above a target threshold of 30 ng/mL, but blood level–time was not measured.10 11 A recent review concluded that transdermal delivery of vitamin D is both safe and effective, and a promising route of supplementation, but to our knowledge there are no publications demonstrating blood level–time profile.12
This pilot study was undertaken to evaluate tolerability and safety of the daily application of patented (US Patent 8821921B2) transdermal vitamin D3 patches over an 8-week period and to measure the blood level–time profile for serum 25-hydroxyvitamin D (25(OH)D) arising from continuous patch exposure. The patches adhere to the skin for at least 24 hours, continuously releasing vitamin D3 and glucose into the epidermis.
Methods
Study design, setting and participants
A prospective, single-centre, open-label, pilot, parallel design study to evaluate tolerability, safety and blood level–time profile from of daily application of vitamin D3 patches over 8 weeks. Participants were healthy adults aged between 18 and 70 years with a body mass index (BMI) between 18 and 32 kg/m2, who were willing to comply with study restrictions. These included: maintenance of habitual diet; no overseas travel, plus avoidance of the following: strenuous exercise, swimming, water sports, prolonged sun exposure, sun lamps, tanning beds, hot tubs and saunas. Exclusions included: supplement use; pregnancy or lactation; screening serum 25(OH)D≤15 nmol/L or ≥100 nmol/L; use of medications known to interfere with vitamin D metabolism (eg, steroids, orlistat, cholestyramine, phenytoin, statins, thiazide diuretics etc); skin conditions such as psoriasis or eczema; or known allergy to plasters. Participants of childbearing potential were required to use effective contraception. Recruitment was via a research database, general practitioners and newspaper advertising. This study ran for 4 months from March 2021.
Sample size and randomisation
There were no previous data on which to base a power calculation. The sample size of 30 was based on pilot study rule of thumb proposed by Whitehead et al, who recommend 15 participants per pilot study treatment arm, assuming a main trial designed with 90% power and two-sided 5% significance, with a medium standardised effect size.13 A computer-generated randomisation list was block generated, with participants randomised to one of the two treatment arms in blocks of two or four. The list included 14 blocks in total.
Study intervention, blinding and allocation
The two intervention arms were big patch (118×80 mm) or small patch (113×22 mm), each containing identical levels of active substances (cholecalciferol 30 000 IU+dextrose 13 mg). As an open-label study both participants and study personnel were aware of which patch each participant received.
One fresh patch was applied to the outer upper arm by 9:00 each morning. Patches were worn continuously for 24 hours before removal, cleansing and application of a fresh patch for the next 24 hours.
A smartphone app enabled completion of a daily e-dairy (Keepers Solutions) for compliance, illness, adverse events (AEs) or medication use. The app also delivered reminders to undertake 2-weekly testing, with additional text reminders and phone calls. The date of vitamin D finger prick tests and confirmation of posting were recorded in the app.
Outcomes and measures
Outcomes were tolerability and safety of daily application of patented transdermal vitamin D3 patches over an 8-week period, and evaluation of blood level–time profile for serum 25(OH)D.
Primary safety outcomes were AEs and treatment emergent adverse events; discontinuation or withdrawal; clinically meaningful change to vital signs and full safety bloods profile (full blood count and chemistry). An AE would be reported where there is a shift outside normal clinical boundaries, or significant clinical worsening from baseline in a laboratory measure or vital sign, with no explainable cause for the abnormality seen. Laboratory analysis was undertaken by Eurofins Biomnis Laboratories, Dublin, Ireland. E-diaries were monitored daily and study visits for assessment conducted at screening, baseline, week 4 and week 8.
Serum vitamin D levels (25(OH)D) were measured at 2-weekly intervals using self-administered finger prick tests and analysed by Medlab Pathologies, Dublin, Ireland (now Eurofins) using Electro-Chemiluminescent Immunoassay (the Elecsys Vitamin D total II) on the Roche Cobas e601 platform. Based on US Institute of Medicine clinical classifications vitamin D ranges were defined as: deficient<30 nmol/L, low 30–49 nmol/L and normal≥50 nmol/L.
Patch compliance was monitored via e-diary entries and return of any unused patches. Dietary intake was assessed using a validated vitamin D-specific Food Frequency Questionnaire administered at baseline, week 4 and week 8.14 Time spent outdoors (potential sun exposure) and use of sunscreen were recorded daily.
Enrolment and data collection
Enrolment is summarised in figure 1. Baseline information included demographic, health, socioeconomic characteristics and whether they were regularly outdoors, for example, for work (see tables 1 and 2). Socioeconomic characteristics (data not shown) were similar between the two treatment groups and ethnicity was predominantly Caucasian (90%, n=27). Vital signs, body weight and height were logged, and BMI calculated. Medical history was recorded, along with current and recent medications. For individuals of childbearing potential a pregnancy test was performed. Fasting bloods were collected and serum 25-OHD level measured.

Consolidated Standards of Reporting Trials 2010 flow diagram.
Baseline demographic and anthropometric characteristics
Are you regularly outdoors?
Eligible participants returned after 14 days to commence the intervention (day 0). Consent was checked and confirmed, full verbal and written instruction provided, e-diary app installed, paper diary provided to document time spent outdoors, time of day and if sunscreen was applied, plus 4 weeks of patches. Following instruction, a vitamin D finger prick test was self-administered, and kits provided for at-home 2-weekly testing.
Monitoring visits were carried out at days 28±3 days and 56±3 days. At each, vitals were checked, medical history and medication reviewed and bloods collected. Patch compliance was corroborated, and unused patches collected. At day 28, further patches, testing kits and paper diary were provided for the remaining 4 weeks.
Data management and statistical analysis
Data were entered into an electronic Case Report Form. Regular-blinded data reviews ensured no missing data points or errors. Descriptive statistics were reported through range, mean and SD for continuous variables and frequency tables for categorical variables. All statistical analyses were conducted using SPSS V.27.0.
Repeated measures (RM) Analysis of Variance (ANOVA) measured change over time for the total sample (n=30) for serum vitamin D (nmol/L), dietary vitamin D intake (µg) and anthropometrics. Paired samples t-tests assessed change over time within each arm (small patch n=15; big patch n=15) for serum vitamin D (nmol/L), dietary vitamin D intake (µg) and anthropometrics. Significance between arms was considered at p<0.05.
Results
Overall, 11 men and 19 women were enrolled and randomised. All completed the study. The mean age was 36.2 years (SD 13.2) and mean BMI 25.1 (SD 2.9). There were no changes in BMI (p=0.34) or total body weight (p=0.32) from baseline to week eight in the total sample or within intervention arms (BMI small patch p=0.05, big patch p=0.47: body weight small patch p=0.05, big patch p=0.53).
Adverse events
Vital signs and safety blood panels remained stable over time and within normal clinical parameters. No significant AEs were reported. Overall, 30 mild or moderate AEs were recorded ranging from reaction to COVID-19 vaccination, to a minor car accident and insect bites (see table 3). One low platelet count was reported in the safety blood panels at week 8. This could potentially be related to patch wearing; however, two of the four blood panels for this subject could not be analysed due to clumping, which made clinical interpretation difficult. All results were reviewed by the medical doctor and deemed to be safe at all timepoints. In the big patch arm, five participants experienced mild or moderate skin irritation AEs related to the patch. These were occasional, mild and spontaneously resolved in three participants; however, for two became continuous and patch application was terminated early. No skin irritation AEs were reported in the small patch arm.
Frequency of causality (n=30 AEs reported) per patch and total sample for participants who reported an AE (n=18)
Compliance
Compliance (≥80 %) was calculated as:

Overall compliance was 93.75% indicating good tolerability. Three participants fell below the protocol compliance threshold of ≥80%, due to patch withdrawal (n=2) and skin irritation (n=1).
Serum vitamin D levels
Five 25(OH)D measurements were taken between week 0 and week 8. Mean serum 25(OH)D level was 45.5 nmol/L (SD 17.51) at baseline (r=20–82 nmol/L), increasing to 62.9 nmol/L (SD 19.86) (r=32–111 nmol/L) by week 8, giving a mean increase of +14 nmol/L for the total sample (see figure 2).

Mean vitamin D levels (nmol/L) over time as measured by the finger prick test by patch size (n=15 per group).
Serum 25(OH)D levels increased gradually from week 0 to week 8, with the greatest change occurring between weeks 4 and 6 (see table 4). Change over time was assessed using RM ANOVA with pairwise comparisons for the total sample and within group comparisons for each patch size (see table 5). A statistically significant increase occurred over time from week 0 to week 8 in the total sample (p<0.001), and within both patch groups (small patch p=0.009; big patch p<0.001). Between weeks 6 and 8 change was not statistically significant in the big patch arm (p=0.128) but remained significant in the small patch arm (p=0.027).
Descriptive statistics for change between timepoints in finger prick serum 25(OH)D levels (nmol/l) at each timepoint by patch (n=15 per patch) and by total sample (n=30)
Pairwise comparisons to assess change over time in finger prick vitamin D results for the sample by treatment arm
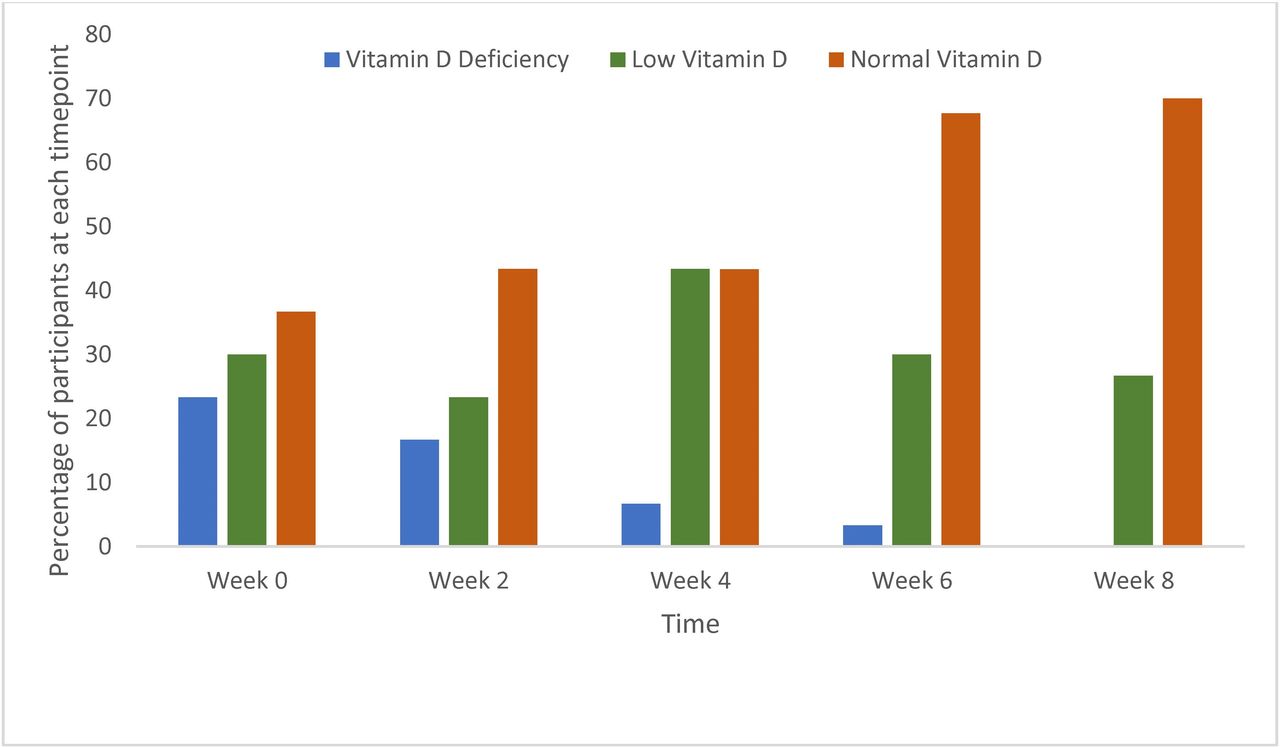
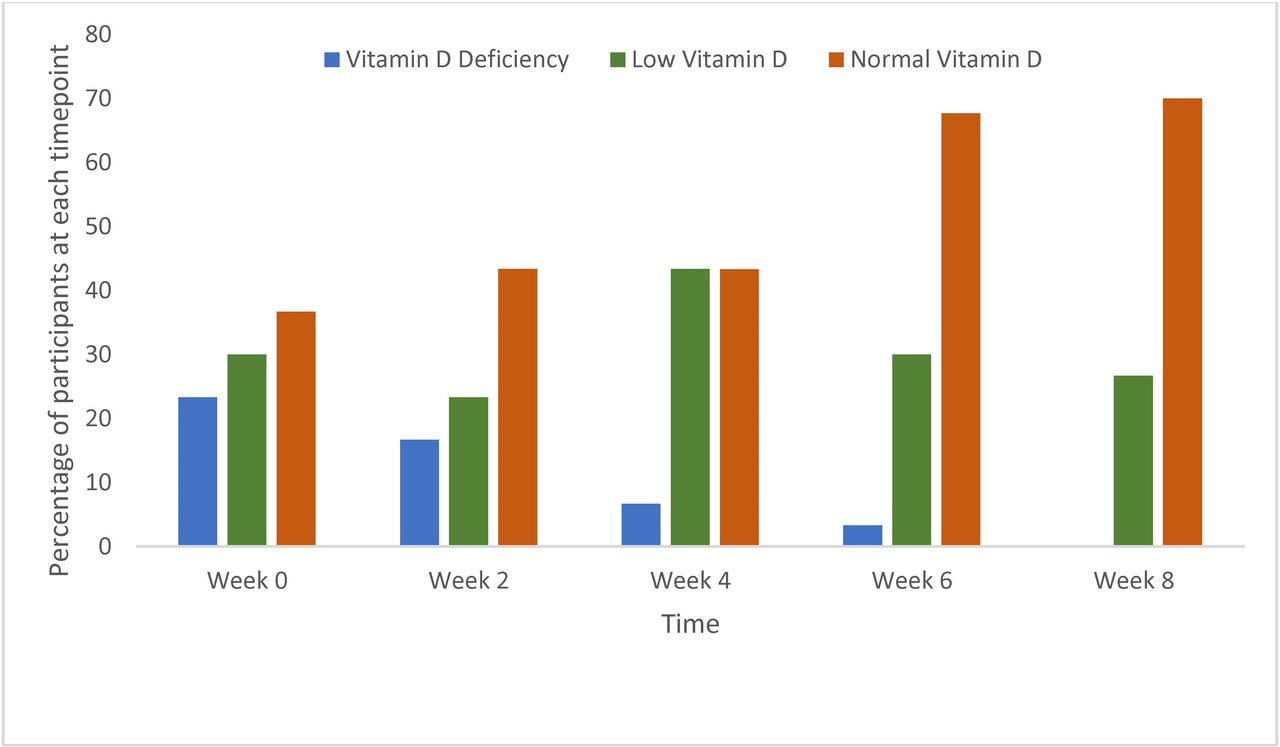
Serum vitamin D status shifted towards normal for all participants (see figure 3). At baseline, 23% (n=7) were vitamin D deficient (<30 nmol/L) reducing to 0% by week 8. Four (13%) moved from deficient to low (30–49 nmol/L) by week 8 but did not reach normal levels. Numbers in the normal range (≥50 nmol/L) increased from 37% (n=11) at baseline to 70% (n=21) at week 8. Regardless of patch size, no participant was deficient or above a safe upper limit of >150 nmol/L at week 8.
{kind=link}
{kind=link}
{kind=link}
25-Hydroxyvitamin D status over time as measured by the finger prick test for the whole sample (n=30).
Dietary intake of vitamin D (µg/day) was assessed over time using RM ANOVA and paired t-test. There were no statistically significant changes in total sample (p=0.40) or within each patch size (small patch p=0.92; big patch p=0.07). It can be concluded that dietary intakes were not a confounder for serum vitamin D.
Sun exposure
This intervention was delayed to March 2021 due to Irish Government COVID-19 pandemic restrictions, making sun a potential confounder. Study participants were required to avoid prolonged sun exposure and compliance was checked at each study visit (table 2). A daily diary was completed reporting time spent outside, time of day and sunscreen application. Data were logged daily from the Irish Meterological Service (Met Eireann) on sun, cloud and weather conditions for Cork Airport (www.met.ie). Average total time spent outdoors was 40 min per day. Based on the work of Parisi et al and Engelson et al, we assumed no vitamin D production would occur with 6+ okta of low or medium cloud cover.15 16 After excluding time between 10:00 and 16:00 where weather was either ‘cloudy’ (defined as 6–8 okta of low or medium cloud) or ‘rain’ for the entire period or where sunscreen was applied, participants spent on average 8.4 hours mixed weather conditions (sun, fair, cloudy, rain) when dermal vitamin D production might be possible, equivalent to 9 min per person, per day.
Discussion
This pilot trial achieved the objective of evaluating safety and tolerability of daily application of patented transdermal vitamin patches. There were no significant AEs in terms of physical or biochemical markers, which remained stable with no clinically meaningful changes throughout the 8-week intervention. None of the participant vitamin D levels increased into the ‘elevated’ range (>150 ng/mL/>375 nmol/L) suggesting little risk of toxicity.
The two arms differed only in terms of patch size; however, after randomisation, the two arms had a difference in mean age (31 vs 42 years). An extensive review of percutaneous penetration and the dermatopharmacokinetics of transdermal products found no age-related differences in the pharmacokinetic profiles and concluded that skin age is not a limiting factor for absorption.17 No significant differences in absorption of drugs from transdermal drug delivery have been observed across different adult age groups, and the barrier function of healthy skin is unaffected by ageing.18–20 The mean age difference in study arms should therefore have no effect.
Minor, occasional skin irritation was reported by three participants (10%) in the big patch arm and 2 (6%) developed continuous irritation requiring termination of patch application. There was no cross over in treatment and it is not known if these individuals would react to a small patch. There were no irritation reports in the small patch arm, so we assume that irritation was likely due to patch size rather than ingredient sensitivity. Between 20% and 50% of users of Transdermal Drug Delivery Systems are reported to experience irritant dermatitis, therefore our rates are lower than might be anticipated.21 22
Serum vitamin D levels increased steadily with each 2-week interval, with the largest change for both patch sizes occurring between weeks 4 and 6. For the big patch arm, change between weeks 6 and 8 (day 42–56) was not significant, which may imply that a plateau for vitamin D was being reached. This is a similar timeline for plateauing of effect seen in other supplementation studies.23 24
A clear shift was seen from deficient and low vitamin D status towards normal with a mean increase of +14 nmol/L, and 70% of participants achieving>50 nmol/L by 8 weeks, similar to rates seen among Irish supplement users (70%).25 A recent pilot study carried out in Italy between May and June 2021, also delayed by the pandemic and controlling for sun exposure, explored serum response to a daily oral dose of 2000 IU vitamin D3/day (5 times the current UK recommendation) and at day 28, found a mean increase of 22 nmol/L.26 Doses of 5 µg or 10 µg D3 over 28 days have been shown to increase serum 25(OH)D by 13.6 nmol/L and 19.6 nmol/L, respectively.27
This study was to be conducted during winter months to avoid potential confounding from sunlight; however, COVID-19 pandemic restrictions delayed the start to March 2021. Steps were taken to limit exposure, with participants required to avoid prolonged sunlight exposure and report daily on any time spend outdoors between 10:00 and 16:00. None of the participants worked outdoors and so time outside was limited to work breaks and weekends. Lockdown restrictions meant that prior to 7 June activities involving travel, eating outside of the home and sport (both playing or viewing) were all strictly limited.
Weather conditions in Cork were generally poor throughout the study period with rainfall three times the normal average during May 2021 and only 8 days where cloud-free sun featured at any point between 10:00 and 16:00 in the Met Eireann data. Ireland experiences total cloud cover 55% of the time with a mean hourly cloud level of 5–6 okta (www.met.ie). This is due to geographical position off the northwest of Europe, close to the path of Atlantic low-pressure systems, which tend to keep humid, cloudy airflows for much of the time. With average monthly temperatures of just 9.5°C in May and 13.3°C in June, skin exposed is likely to have been limited to hands and face. Our population averaged 40 min outdoors per day, which is one-third less than the 69 min per day typical for the British population.28 After adjusting for total cloud cover (6+ okta) and sunscreen use participants averaged 9 min outdoors in mixed weather conditions between the hours of 10:00 and 16:00. O’Sullivan et al determined daily average vitamin D stimulating UVB dose across Ireland based on data from a 10-year period, and after cloud correction concluded that achieving sufficiency (>50 nmol/L) from sunlight was not possible in Ireland throughout the whole year.29 Median vitamin D levels within their cohort were 49 nmol/L during winter and spring, rising to 56 nmol/L in summer and 63 nmol/L in autumn. Modelling of seasonal variation due to sun exposure suggests that public health advice to spend 10–20 min daily in sunshine during the summer months contributes a maximum increase of 5–10 nmol/L between May and September.30
Modelling from UK and Irish data shows 25(OH)D levels to peak during August–September31–34 with the greatest increase in levels during July–September.25 Seasonal variation is suggested to account for around 13% of the increase in summer compared with winter, even in the sunshine state of Florida, USA.35 The Irish Longitudinal Study on Ageing (TILDA) shows a mean peak of 60.4 nmol/L in August, with an average difference of 6.2 nmol/L between seasons for women and 11.9 nmol/L for men.32 Multiple linear regression analysis found vitamin D supplement use to be a far greater contributor to 25(OH)D levels (+27.2 nmol/L) compared with sunlight. The Trinity, Ulster and Department of Agriculture (TUDA) Study, also carried out in Ireland, measured a peak in global solar radiation exposure in the month of July with peak 25(OH)D levels occurring in August, representing a lag period of ~1 month.33 TUDA also found supplement use to make the greatest contribution to 25(OH)D, adding between 21.4 and 35.4 nmol/L.33 The final vitamin D measurements in our study took place from mid-June to early-July, before the anticipated seasonal effects of sunlight exposure in Ireland would have taken place.
The COVID-19 restrictions in place in Ireland for the duration of our study meant that many outdoor activities were strictly limited, and no foreign sun exposure occurred. Sunny holidays abroad for those living in the UK have been found to make a significant contribution to normal summer vitamin D status, with individual taking holidays overseas achieving summer (June–August) 25(OH)D levels more than 10 nmol/L higher (population mean 56 nmol/L; with sunny holidays 64 nmol/L; no overseas holidays 52 nmol/L).36
Our pilot study has shown a marked improvement in status, with a 22% increase in mean vitamin D from baseline to week 8, achieving by early summer the vitamin D status that might be expected within a healthy Irish adult population at the late summer/early autumn peak of a non-pandemic summer (including foreign holiday travel). While we cannot determine for certain the contribution of skin exposure to change in vitamin D status in our study population, the local weather conditions, on-going pandemic restrictions, combined with study requirements limited this as far as possible under free living conditions. Daily brief exposure of 9 min in mixed local weather conditions is likely to have had limited effect on 25(OH)D levels.
This pilot trial has shown that these patented transdermal vitamin D patches are safe for daily application, with no effects on safety parameters or risk of vitamin D toxicity. There was a positive shift in vitamin D status for all participants. Further work is now warranted to explore in detail the efficacy of these patented vitamin D patches both in terms of the alleviation of pain, and as a route of supplementation.
Limitations
The study was single centred and conducted in the population of Cork and participants were almost all white-Irish heritage, the finding may therefore not be equally applicable across different skin types. Although planned to be carried out during winter months delays due to the COVID-19 pandemic meaning that the lack of a control group became a limiting factor. Sun exposure was self-reported using a paper diary and it was assumed that continuous low cloud cover of 6+ okta between the hours of 10:00 and 16:00 occluded vitamin D production.
Data availability statement
Data are available upon reasonable request. Data available on reasonable request from corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study was designed and conducted by Atlantia Food Clinical Trials, located in Cork, Ireland according to the principles of International Conference on Harmonisation Good Clinical Practice and the Declaration of Helsinki. This study involves human participants and was approved by CREC Review Reference Number: ECM4(m), on 09 February 2021. Clinical Research Ethics Committee of the Cork Teaching Hospitals Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the team at Atlantia Food Clinical Trials, Heron House Offices, First Floor, Blackpool, Cork, Ireland, who undertook the research and provided all statistical analysis and access to data.
References
Footnotes
Twitter @angie_nutrition
Contributors CB initiated the study. AJ managed the conceptualisation and design of the study. CB and AJ appointed Atlantia Food Clinical Trials to carry out the research. AJ project managed research delivery. Drafting of the manuscript and critical revisions: AJ and CB. AJ is the guarantor of content.
Funding All funding was provided by To Better Days (previously Horopito).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.