Article Text

Abstract
Background to issue Future sustainable healthcare delivery and systems need reflective practitioners and critical thinkers to engage the public to achieve health policy aims and objectives. Therefore, this descriptive review introduces a generic conceptual framework, adopting a specific theme to illustrate and demonstrate a model of care or any other context. Whatever the purpose, context or philosophical stance in healthcare and health literacy, there is no standardised generic conceptual framework to structure reflection and critical thinking. This work presents a pragmatic solution focused on the one-to-one relationship of learner–mentor, patient–clinician, public health professional–public and groups.
Methods The method is constructivist, an educational exercise, practical and the target group can be defined/viewed as student, teacher, patient, carer or member of the public in a health promotion campaign, for example. The building blocks are health and care concepts that arise clinically in practice, or for a student writing an assignment. As will be explained, concepts (including the Sustainable Development Goals) are assigned by the subject(s)—in this instance the authors—to a domain of knowledge.
Results As two-by-two tables, the results represent the structure of the conceptual framework, framing the content in a series of four knowledge (care) domains. The contents, ultimately the Sustainable Development Goals, may then be linked and relationships discussed. Results are produced gradually, building a cognitive or mind-map. The results, it must be stressed, are therefore qualitative.
Conclusion Drawing on educational theory and practice, the results are explored and justified using the theme of nutrition, and the often stated desirability in education of reflective practice and critical thinking abilities. Providing a series of cross-disciplinary, the reader will gain insight into the potential of Hodges’ model to facilitate integrated, person-centred and care that improves parity of esteem, supporting students and qualified personnel in their learning careers.
- Cognitive performance
- Dietary patterns
- Mental health
- Nutritional treatment
- Nutrition assessment
Data availability statement
No data are available. This essay did not involve data gathering from research subjects.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Modern healthcare and medicine is marked by the Cartesian divide.1 This division is evident in knowledge terms, communities of practice (health disciplines) and can be experienced as fragmented, poorly integrated care.2 Ongoing clinical practice by the first author confirms what appear to be legacy issues for new learners, and disparity in integrating care across disciplines (physical and mental) and between health (National Health Service) and social care service. This work is concerned with situations, their endless variation, our need to make sense of them which in turn raises the issue of having a means to structure our deliberations. Integration of care is necessary at individual and global health levels, hence this review is predicated on the potential benefits of a generic framework that provides a structure for reflection, critical thinking and ultimately an accessible scaffold to help integrate care.3 By generic framework we refer to a structure that is global in scope, and open; creating a series of conceptual spaces4 in which a student, practitioner, patient (carer) or member of the public can critique a situation. By open, and as genericity suggests, the framework transcends professional and disciplinary boundaries; and yet, it is simultaneously simple and complex enough to integrate and conjoin what can be epistemological and disciplinary silos.
Such a framework should be accessible to as many people as possible (simple on first encounter), this means cognitively accessible to people with minimal literacy, who rely on language and basic drawing skills. In healthcare a global resource must be deemed as ethnoculturally neutral to be considered, learnt, accepted, used and shared. Paradoxically, an open, accessible and neutral tool is also political; socioeconomic access to resources is a further desideratum. The pandemic, climate crisis, conflicts and policy are further confounding factors for any candidate model or framework. This descriptive paper introduces a conceptual framework, (or) a model of care for the self, population and planet (a resource follows the references and provides a bibliography).
In their initial professional education and training healthcare practitioners also learn to teach. An ability to teach patients, their carers and new learners is a vital part of a professional’s role. Clinicians should therefore, recognise the relevance of learning theories including behaviourism, cognitivism, constructivism and social constructionism to their work.5 This paper invites readers to reflect on the gamut of lived experience, as encountered in healthcare and the disciplinary expanse of knowledge that contributes to learning, sense-making (whether ‘listened to’ or not) and of course life, death and recovery. This review concerns a tool that can encompass these learning theories and provide a scaffold for learners. Helping to support vocabulary and conceptual development, reflective and problem-solving abilities, literacies (broadly—emotional, technology, cultural…), technical competency, awareness and expertise, peer working and being socialised into a profession within society.
Hodges’ model was created in the early-mid 1980s by Brian Hodges, a senior lecturer (retired) at what is now Manchester Metropolitan University, UK. A small bibliography sees Hodges’ model applied in several contexts, including recovery and disaster response.6 7 The model is best explained through a diagram as per figure 1, which shows Hodges’ model in its simplistic, basic (template) form. The model is, however, potentially complex and can form the basis for a ‘rich picture’.8 As shown in figure 1, the model’s two axes intersect. The horizontal axis differentiates between HUMANISTIC–MECHANISTIC activities and phenomena. The vertical axis is the INDIVIDUAL–GROUP (population). The intersection of the axes creates four quadrants, domains within which relevant concepts can be placed. Each quadrant is associated with knowledge content as follows: (1) Sciences; (2) Intrapersonal–Interpersonal; (3) Sociology and (4) Political.
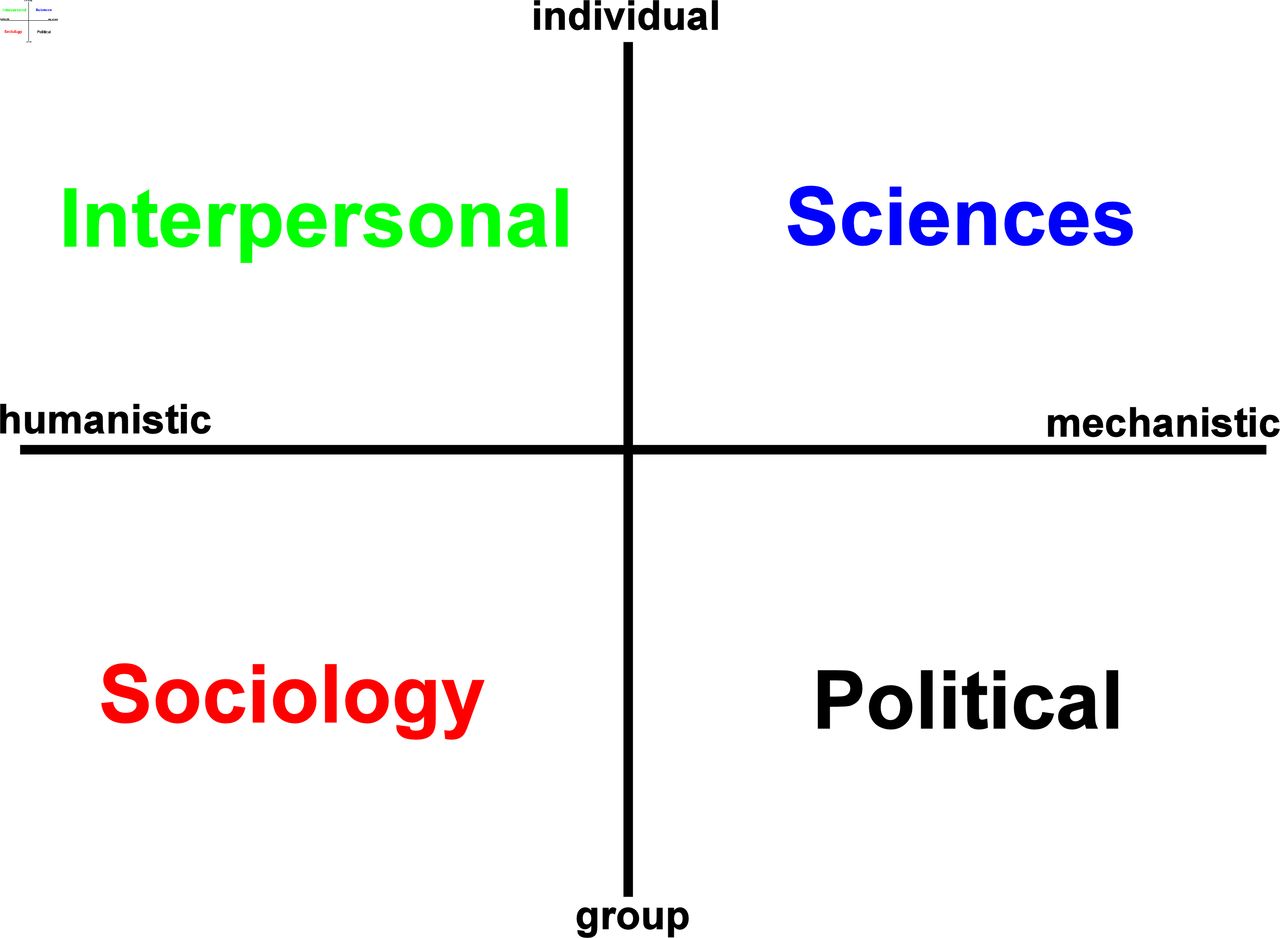
The axes and domains of Hodges’ model: the two axes provide a structure, a conceptual scaffold that creates four quadrants, care or knowledge domains within which the user of the model can place keywords as per a situation or context.
These domains of care, for contextual, situated knowledge are not placed arbitrarily, but can be confirmed through a series of questions (a Socratic dialogue) drawing out the subjects (persons) and agents (formal and informal) and types of activities and interventions that fall under the auspices of health and care. Accordingly, the placement of concepts depends on the specific purpose and situation of the person(s) using the model. This situatedness accounts for the model’s simplistic, complex (‘rich’) and dialectical potential. The original purposes of Hodges’ model were to facilitate integrated care, person centredness, reflective practice and help bridge the theory–practice gap.
There is no specific theory to account for, or explain the placement of concepts in the model. Language, grasp of vocabulary and understanding of concepts are key. If figure 1 is a blank template (an empty set), then we can develop the list of domains as follows:
Sciences—Nutritional data/labelling on foodstuffs.
Intrapersonal–Interpersonal—Anxiety provoked by thoughts of body-image and eating.
Sociology—Social behaviours and learning based in school regards nutrition.
Political—Policies on advertising of ‘junk’ high-calorie foods.
While there is no theory, a student using the model would be expected to explain and justify their reasoning. Mentoring and supervision at an individual and group level are a pivotal part of applying the model and learning. Therefore, the goal of this brief review is to explore, explain and demonstrate the potential utility of a generic conceptual framework, especially its scope, potential user-base and application.
Method
Hodges’ model draws on the ideas and theories that underpin linguistics, the semantic web and educational theory and practice. Of course, it is the student’s interpretation and conceptualisation of a situation that is fundamental to learning. Discussed by Bender, Hodges’ model presents a means to provide a metaparadigm for nursing: ‘a gestalt, a global perspective, a total world view or cognitive orientation which is held by the majority of members of a discipline’.9
Here the authors adopt Vygotsky’s socio-constructivist approach,9 using Hodges’ model as a scaffold for reflection.10 In this review, the authors use the Sustainable Development Goals (SDGs) as input, and decide on where in the aforementioned model, the primary concepts in the SDG should be placed. The outputs are presented as figures (two-by-two tables).
Mapping the United Nations SDGs
The 2030 Agenda for Sustainable Development and its 17 SDGs were adopted by the United Nation (UN) in 2015, and are based on three principles: being transformative, universal and indivisible.11 The task is to take each SDG (as numbered 1–17) from ‘No poverty’ through to ‘Partnership for the Goals’ and assign each to a domain of Hodges’ model. The model’s idealised nature, the interpretive nature of the exercise and its subjective quality are realised in that some SDGs may span more than one domain. Two figures will depict the model using a 2×2 tabular format, ‘mapping’ the SDGs to Hodges’ model in progressively more detail. The SDGs include SDG-3 and SDG-4 on health and education, respectively. The SDGs are ‘objectives of a programme that aims to be a comprehensive blueprint for human development’.12 In turn, ‘Good health is a precondition for, an outcome and measure of, sustainable development’.12
Figure 2 maps the three pillars grouping of the SDGs12 to Hodges’ model. ‘Specific health interventions’ spans the domains concerned with the individual, the interpersonal and sciences domains. This encompasses mental health and physical health. ‘Environmental protection’ straddles the physicality of habitation, urban, remote, governance and the law of land, sea and air.13 ‘Shared Prosperity’ and ‘Social Justice’ are placed in the domains that cover social and political phenomena. Placing subjective judgements aside, in figure 2, a concentration of the SDGs on the right-hand (mechanistic) side of Hodges’ model is noted. This can be accounted for in the materialist explanation of health inequity, the existence of a social gradient in resource usage and the lived experience of social (im-)mobility.14 A conceptual clustering apparent in figure 2, is continued in figure 3. Figure 3 provides a more detailed view of the 17 SDGs mapped to Hodges’ model.

The SDG pillars mapped to Hodges’ model. SDG, Sustainable Development Goal.
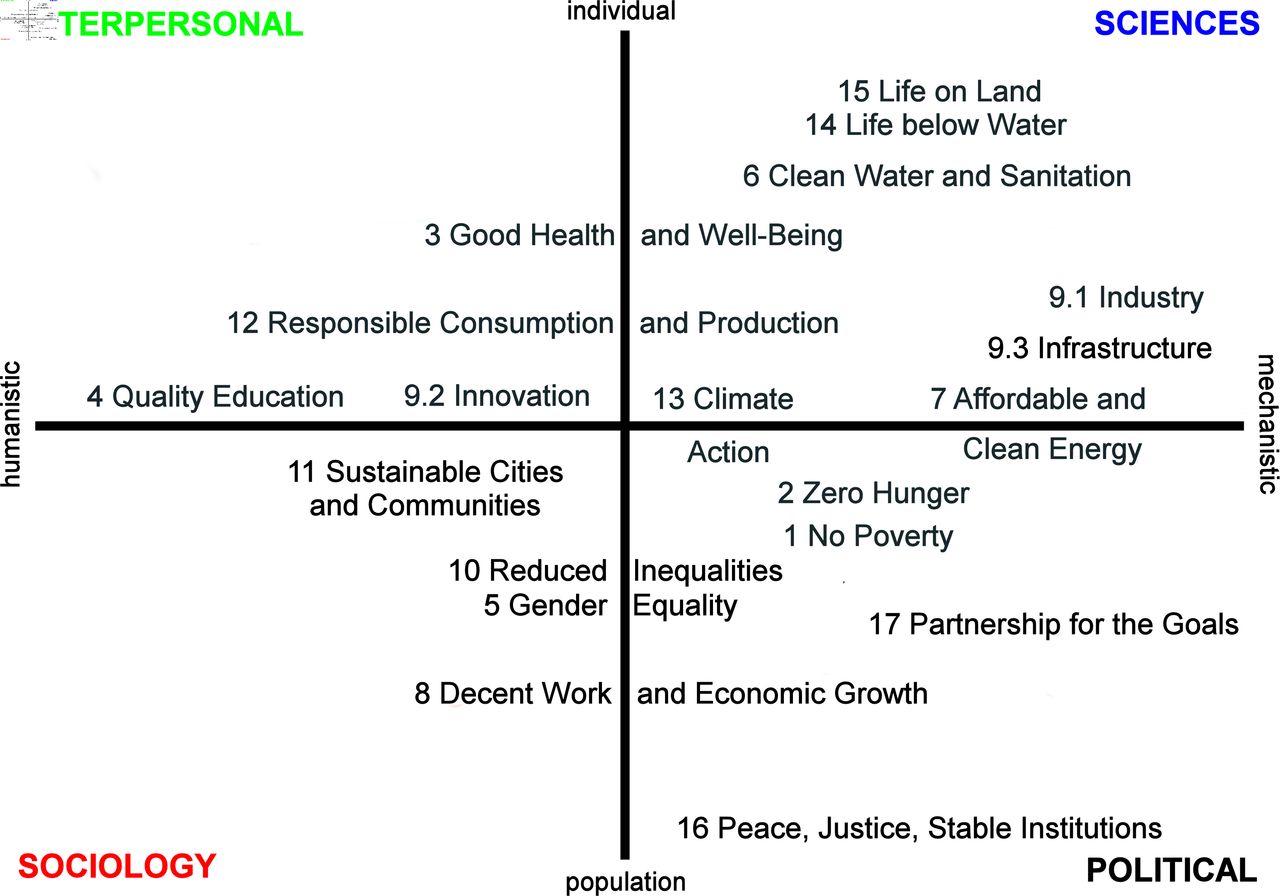
The 17 Sustainable Development Goals mapped to Hodges’ model.
Results
What conclusions can we derive from the figures thus far? The primacy of the mechanistic domains continues in figure 3, the listed SDGs stress the environment and natural resources. Results here are not ‘data bound’ but will be found in reflection, critique and discussion associated with the figures. For example, the dichotomy of developed versus developing economies. The fact that developed nations have benefitted socioeconomically from natural resource extraction (without local degradation).
‘Quality Education’ holds a prime position in the intrapersonal–interpersonal domain. If education seems isolated in its placement, what might we deduce from this? Hodges’ model prioritises the individual as the focus of health interventions and yet helps us navigate between: think global, act local! Climate change, COVID-19 and the Ukraine conflict reinforce the interdependencies between people, nations (we suddenly see the geopolitical disciplinary bridge) and SDGs and taken-for-grantedness of food and water (from irrigation and free access to ports). Collectively, what are the systems of production, safety standards, labelling and applicable policies and land rights14? If the humanistic domains of Hodges’ model are sparse in the preceding figures, does this highlight the dependency on physical and political factors?
Type 2 diabetes is an example, the treatment is dietary advice and exercise. Attention needs to be paid to the person’s level of (health) literacy, the balance of the individual’s existing diet, shopping and factors such as income—budget for meals, health and technology (device) literacy—use of ‘Apps’, reading, food labelling, mobility, transport and accessibility. Referral to welfare, community meals and other services may be indicated. Figure 4 relates broad concepts related to nutrition to the model including children, diet, exercise and sports.15

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nutrition within Hodges’ model. SDGs, Sustainable Development Goals.
Discussion
The goal was to explore and apply a generic framework—Hodges’ model. The results and figures show (1) the conceptual scope of this model, revealed by placement of the SDGs; (2) the structure afforded by the model’s axes; (3) the results of the reflective process; (4) the dialogue generated and critique of the content. We are responding to Dewey:
‘Reflection is turning a topic over in various aspects and in various lights so that nothing significant about it shall be overlooked— almost as one might turn a stone over to see what its hidden side is like or what is covered by it.’16
The vertical axis of Hodges’ model takes the engaged reader from personal/individual health to family and the collective public (mental) health and the population health of nations and consideration of global and planetary health.17 18 The model is metacognitive and metaconceptual. Hodges’ model is also a system of systems, as in, the need to differentiate between ‘health systems’ and ‘healthcare systems’ and language use, as in ‘population health’.19 20 Ban Ki-moon, a former United Nations Secretary-General (2007–2016) can explain figure 3 and the pursuit of constant economic growth: ‘We don’t have plan B because there is no planet B’.21
The placement of SDG-3 ‘Health and Well-being’ may be interpreted as sustaining the mind–body dichotomy; but, in defence, recognition of dichotomies and oppositions is essential to minimise the impact of siloed thinking and stresses the need for integration. This division in healthcare is a historical legacy: the Cartesian divide. Lack of parity of esteem between physical and mental healthcare can provoke ringfenced finances.22 Disciplinary silos and their professional expression and advocates do have a function.23 Also in assuring that public health is inclusive of (public) mental health. ‘Quality education’ appeared isolated in figure 3. We usually seek balance, equilibrium and yet the imbalance here may be positive as follows:
Acknowledges the distinction between people’s social situation and the determinants that trap so many (this is not the form of sustainability we seek).
Points to diametrical oppositions in this model, especially between the (intrapersonal) interpersonal and political domains.
Accentuates the individual–collective axis via the vulnerability of the individual.
The UN SDGs Knowledge Platform outlines the history of the SDG’s development. Important here is the multilateral nature of their genesis in 2015 and their being subject to annual review and follow-up by the United Nations High-level Political Forum on Sustainable Development.24 The Paris Agreement and Agenda 2030—‘both represent internationally agreed, universal visions. Their implementation is based on a “bottom-up” process, meaning that countries identify and subsequently act and report on their own priorities, needs and ambitions’.24 This is also affecting the policy coherence of plans and strategies and aggregate analysis is lacking between the national situation and national responses. Furthermore, it is highlighted ‘not all UN-recommended indicators yet have a defined methodology’.25
Interdependencies abound, as expected. The dependency of environment protection on international cooperation and law are clear; the politics of climate change, the fate of Amazonia, the pace of ecological degradation, the limitations and delays of climate negotiations.23 Birds and bees act as a bell-weather for crop security and environmental quality. Pollution may be a factor in male fertility, associated with plastics in the environment.14 Air pollution is incorporated in SDG-3 and associated fatalities are drawing attention.
Nutritional needs vary through the lifespan, for pregnant women, growing infants, children, adolescents, adults, athletes, older adults and the sick all have specific and individual needs. The benefits of plant-based—especially nutrient-rich whole food vegan—diets to sustainable (individual and public) health can draw on evidence-based recommendations from 1978 through to today.26 Therefore, this appeal goes out to experts and practitioners alike specialised in nutrition, sports, medicine and health, to be more open-minded and not to reject out of hand an individual’s intention to adopt a vegetarian or even vegan diet.27
Healthcare and medicine must be evidence-based,28 personalised and/or patient-centred. In contrast, it can be difficult to justify the need for broad, overarching tools. Many resources applied in the humanities, cognitive sciences, healthcare and education are inherently phenomenological. The SDGs are broad in scope. As a result goals may be stated in general terms, which impacts the ability to communicate, implement and measure.29 COVID-19 has added to pressures: ‘years, or even decades, of development progress have been halted or reversed’ and, ‘an additional 75 million to 95 million people will live in extreme poverty in 2022’.30
The sociotechnical and sociopolitical bridges are non-trivial; ‘tackling health inequities is not simply a technical matter, it is an ethical pursuit’, stressing values.31 Proof of the latter is vital to citizens in land rights, employment and economic agency32 and overcoming gender inequality and ultrapoverty.33 As the SDGs are tracked and measures of progress refined,34 35 Hodges’ model can help academics, practitioners to navigate the inevitable complexity encountered to help assure public (mental) health at individual, community and global levels and act as a ‘uniqueness preserver’36 in delivering person-centred care.
A generic, universal assessment and evaluation tool with sufficient conceptual scope and relevance can assist the implementation of the SDGs, achievement of sustainable healthcare systems and universal health coverage: a blueprint—realised. Educational theories and cognitive linguistics inform ongoing study. Threshold concepts37 and conceptual spaces4 may contribute to a theoretical foundation for Hodges’ model, as may One Health.38 To fully apprehend nutrition—clinically, socioeconomically, politically, locally and globally… we must, as an example, incorporate and navigate the potential benefits of agritech, to reduce poverty on one hand; and the fatal consequences of eating disorders (anorexia and bulimia) on the other, assuring parity of esteem (physical and mental health)?39 As shown, Hodges’ model can complement ongoing work in nutrition and recognition of the planetary scale.38 The best way to ‘Leave No One Behind’ is to ensure individuals have the requisite literacies, so they can advocate for self, family and community; and ‘not be pushed behind’.33 40
Conclusion
The authors believe that personal and global health as read in theory and realised across the world can benefit from a generic framework. We have seen how the context of nutrition is potentially challenging for new learners, qualified staff must retain high standards and maintain their professional standards pursuing lifelong learning. Through a progressive process we have shown how a simple cognitive resource can help us conceptually grasp the complexity of healthcare as presented within the SDGs. This practical review has outlined the scope and manifold utility of Hodges’ model, using the SDGs (excluding the targets) linked to nutrition. The model can conceptually encompass all forms of literacy, schools of informatics and provides interdisciplinary bridges; such as, psychosocial, sociopolitical and psychopolitical. In future the model could be instantiated in software; an ongoing research aim. Just as impoverished, arid, stony ground does not augur well for crop growth, the critical thinking that informs our work must be expansive and cross-disciplinary at the outset. This generic model can assist in assuring holistic bandwidth and as Dewey reminds us—guiding us in the stones we turn.
Data availability statement
No data are available. This essay did not involve data gathering from research subjects.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors extend thanks to Professor Judith Ellis for comments on an original draft of this paper and referees for their constructive comments. KW has provided invaluable support and encouragement in completing this work (PJ).
References
Footnotes
Twitter @h2cm
Contributors PJ is the main author based on an original paper submitted to BMJ-GH. KW provided assistance and content on nutrition since July/August 2020 to produce this latest and transferred submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed by George Kernohan, United Kingdom of Great Britain and Northern Ireland.
Author note The interested reader is kindly referred for further and deeper information to the following online source: https://hodges-model.blogspot.com/