Article Text

Abstract
Vitamin D deficiency, which impedes good immune function, is common during winter and spring in regions of high latitude. There is good evidence that vitamin D deficiency contributes to the seasonal increase of virus infections of the respiratory tract, from the common cold to influenza, and now possibly also COVID-19. This communication explores key factors that make it more likely, particularly in combination, that individuals are vitamin D deficient. These factors include old age, obesity, dark skin tone and common genetic variants that impede vitamin D status. Precision nutrition is an approach that aims to consider known personal risk factors and health circumstances to provide more effective nutrition guidance in health and disease. In regard to avoiding vitamin D deficiency, people with excess body fat, a dark skin tone or older age usually need to use a moderately dosed daily vitamin D supplement, particularly those living in a high-latitude region, getting little ultraviolet B exposure due to air pollution or staying mostly indoors. Carriers of the GC (group-specific component) rs4588 AA genotype also are more likely to become deficient. Very high-dosed supplements with more than 4000 IU vitamin D are rarely needed or justified. A state-by-state Mendelian randomisation analysis of excess COVID-19 mortality of African-Americans in the USA shows a greater disparity in northern states than in southern states. It is conceivable that vitamin D adequacy denies the virus easy footholds and thereby slows spreading of the contagion. This finding should drive home the message that vitamin D supplementation is particularly important for individuals with dark skin tones. Vitamin D deficiency, even for a few months during the winter and spring season, must be rigorously remedied because of its many adverse health impacts that include decreased life expectancy and increased mortality. Slowing the spread of COVID-19 would be an added bonus.
- precision nutrition
- infectious disease
- nutrient deficiencies
- pulmonary disease
- dietary patterns
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What does this paper add?
Individuals with high age, excess body fat, dark skin tone or risk-predicting genetic variants are likely to need extra vitamin D, particularly during the dark months of winter and spring.
Precision nutrition aims to make nutrition guidance more effective by taking into account key factors that are already known to influence requirements.
The greater excess of COVID-19 deaths in northern US states appears to support the hypothesis that vitamin D deficiency in African-Americans contributes to their disproportionally higher risk.
Prevention of vitamin D deficiency at any time of the year must be pursued in earnest, particularly in people most likely to be at risk due to easily identifiable common characteristics.
Background
Rationale
As the COVID-19 pandemic is rapidly expanding, we need to proactively explore plausible options to slow its seemingly inexorable progress and be better prepared for new waves of epidemic severe respiratory infections. We would be amiss if we did not look earnestly for low-risk nutritional interventions that can be deployed to the entire public. Correcting deficient vitamin D status may be a good target for such an intervention1 because the possibly seasonal outbreaks of COVID-19 and the previous severe acute respiratory syndrome (SARS) epidemic could point in this direction. Vitamin D deficiency is extremely common during winter and spring in regions located at higher latitude, which may be defined as places at a latitude greater than 40° and includes the UK, Central and Northern Europe, Canada and the northern half of the USA, and similarly some regions in the southern hemisphere. This short communication will explore key factors that increase the likelihood of individuals to have low vitamin D status during winter and spring as a permissive factor for viral infections of the upper respiratory tract, such as and including COVID-19.
To make it clear at the outset, this presentation concerns only measures that ensure adequate vitamin D status within currently accepted guidelines and is not suggesting the use of very high oral doses that exceed currently set upper limits.
The consideration of factors that make it more likely for an individual to have vitamin D deficiency is an important example for the practical application of precision nutrition (PN).
A brief synopsis of current and earlier severe acute respiratory infections
SARS was caused by the SARS virus, a member of the coronavirus family. It affected more than 8000 people in 29 countries. First observed in November 2002 in Guangdong of the southern part of China and then spreading elsewhere, it eventually disappeared in July 2003, after intense public health interventions (https://www.cdc.gov/dotw/sars/).
Middle East respiratory syndrome was caused by the Middle East respiratory syndrome coronavirus, another member of the coronavirus family. Though first identified in September 2012 in Saudi Arabia, it was eventually traced back to cases that occurred as early as April 2012 in Jordan, and caused a small number of infections, with the largest cluster reported for South Korea (https://www.cdc.gov/coronavirus/mers/about/index.html).
The current pandemic COVID-19 is caused by yet another member of the coronavirus family, SARS coronavirus 2 (SARS-CoV-2). Early infections were observed during November 2019 in Wuhan of Hubei province of central China. The disease has since spread to many other countries around the globe (https://www.cdc.gov/coronavirus/2019-ncov/about/index.html).
Current evidence for a role of vitamin D in fighting respiratory infections
The active vitamin D metabolite, 1,25-dihydroxyvitamin D (1,25D) is produced in immune cells and stimulates there the expression of numerous genes related to a healthy immune response.1 2 Examples of 1,25D-related actions are the accelerated maturation and recruitment of macrophages, promotion of phagocytosis, increased production of cathelicidin, defensins and other antibacterial peptides. 1,25D also appears to act on various types of epithelial cells and trigger their own immune-defensive mechanisms. Another important benefit of sufficient vitamin D status may be its suppressive effect on excessive cytokine release which can be a lethal consequence of severe respiratory virus infections.
A recent editorial pointed out that countries below the latitude 35° North and all the way across the southern hemisphere see lower COVID-19 mortality rates than countries further to the north.3 The authors hypothesise that lower capacity to produce vitamin D at higher northern latitudes at this time of the year impairs vitamin D status, which then could be a cause for the observed high mortality.
Key modulators of vitamin D status
Dietary intake
Intake of the most common natural form of vitamin D, cholecalciferol (vitamin D3), increases 25-hydroxyvitamin D (25(OH)D) levels in most, if not all people. The rare exceptions are usually due to acquired or inherited disruptions of vitamin D absorption and metabolism, such as severe cholestasis and abetalipoproteinaemia. Ergocalciferol (vitamin D2) is now a less common form in dietary supplements with lower bioavailability and potency than vitamin D3, but has been used extensively in the past because of the low cost associated with its production.4
Only a few foods, mainly fatty coldwater fish, like herring, sardines, mackerel and salmon, contain naturally significant amounts of vitamin D. Some foods, such as milk in the USA and fortified cereals in many countries, contain artificially added vitamin D, typically as vitamin D3. Another important vitamin D source for some people are dietary supplements.
After vitamin D is absorbed from the small intestines and bound to vitamin D-binding protein (VDBP) in circulating blood, it eventually reaches the liver and is then rapidly converted by cytochrome enzymes, mainly CYP2R1, to the 25(OH)D form found in circulating blood.4
Higher vitamin D intake then tends to be associated with higher 25(OH)D concentrations. Representative oral doses of 400, 4000 and 10 000 IU supplemental vitamin D3, in addition to approximately 200 IU from foods, were seen after 3 years to increase initially adequate 25(OH)D levels by about 0%, 63% and 78%, respectively.5 It is evident that the 400 IU dose induced little change, while the very high 10 000 IU dose raised the 25(OH)D level not much more than the high 4000 IU dose. Clearly, adaptive mechanisms respond to excessively high intakes, limiting increases of 25(OH)D concentrations in blood. These observations are largely in line with findings in other studies.
However, most people get no more than very modest amounts of vitamin D from dietary intake. Elderly individuals often do even worse than younger adults, not least because of their lower total energy intake. Milk fortification in the USA is only of limited help for many older people, particularly for those with African ancestry, due to often limited lactose tolerance and therefore common avoidance of milk. It should not come as a surprise that older people in the USA were found to get less than 140 IU per day on average from food and dietary supplements combined.6
Ultraviolet B (UV-B) exposure
By far the most of the vitamin D in blood comes from skin exposed to the UV light with wavelengths between 280 and 315 nm, usually referred to as UV-B.7 In this process, the precursor 7-dehydrocholesterol from the cholesterol synthesis pathway is converted via an intermediary step to vitamin D. The newly formed vitamin D in skin moves into blood and is then converted by liver enzymes (mostly CYP2R1) into 25(OH)D, just like vitamin D from dietary sources.4
Typical production of vitamin D in people working outdoors with generous exposure of skin to summer sun in the American Midwest (latitude 41.5° North) averaged the equivalent of around 2800 IU (70 µg) vitamin D intake.8
Spending much time indoors, severe air pollution, prolonged cloud cover, covering skin with garments and using sunscreen each can limit vitamin D production in the skin to varying degrees. For example, sunscreen with a sun protection factor of 15 decreases vitamin D3 production in skin by 99%.9 As might be expected, skin pigmentation also limits vitamin D production, which will be discussed in more detail below.
Ageing
Finally, high age is another important factor associated with lower vitamin status. The lower 25(OH)D levels are commonly due to spending much time indoors and often due to deliberate avoidance of sun exposure for fear of skin cancer. There is also progressive thinning of the skin. This has been thought to decrease the amount of the 7-dehydrocholesterol precursor available for conversion to vitamin D and 25(OH)D level declines accordingly in advanced age. However, the expected decline in 25(OH)D levels in older adults was not confirmed in a later, targeted study.10 Instead, diminishing ability of vitamin D to counterbalance rising parathyroid hormone concentration triggered by declining renal function was seen as the key driver.
Body composition
A meta-analysis of 18 studies found that obesity greatly depresses vitamin D status and that it limits the ability of dietary supplementation to raise vitamin D concentration in blood.11 The resulting decreased vitamin D status is reversible when some of the excess weight is shed.12 For example, a weight loss intervention sustained over 1 year with a 26% decrease in visceral adipose tissue mass was accompanied by a 26% increase of 25(OH)D levels, from initially 19 to 23 ng/mL a year later.
The mechanisms responsible for depression of circulating 25(OH)D levels by obesity continue to be under debate. There may be sequestration of available vitamin D in the higher fat mass volume. Another explanation has been seen in adjustments of vitamin D metabolism that lead to greater production of 1,25D and suppression of 25-hydroxylation of vitamin D in the liver.12
Genetic variation
Skin tone
The capacity to make vitamin D in skin is limited by skin pigmentation. Genetically inherited variants in several genes control typical skin tone and thereby the capacity to produce vitamin D in skin. One recent study of people residing in the USA found that nearly all non-Hispanic blacks (97%) and most Mexican-Americans (90%) had vitamin D insufficiency.13 Another study, this one of Chicago residents, found average serum 25(OH)D levels of 17.2 ng/mL in African-Americans and of 24.2 ng/mL in European Americans, similar to findings in other regions.14 In another study of participants sampled from 12 southwestern states in the USA, mean 25(OH)D concentrations were 17.5 ng/mL in African-Americans and 27.2 ng/mL in European Americans.15 These observations illustrate the distinct difference by race, with dark-skinned individuals having around a third lower 25(OH)D concentrations than light-skinned individuals. Obviously, there is still great variation in skin tone within racial categories, though quantitative vitamin D information by skin type is sparse. This means that we also do not know enough about the amount of UV-B needed to prevent vitamin D deficiency in the majority of the global population with dark skin tones. We can just be reasonably sure that 400 IU per day will not be enough for many of them at some time of the year or stage of their life.
Vitamin D synthesis, transport and metabolism
A recent compilation of more than 30 studies including almost 80 000 participants with predominantly European ancestry and used available data to estimate as part of a genome-wide association study the effects of common variants on 25(OH)D concentrations.16 The genes with the strongest associations were GC (encoding VDBP), CYP2R1 (encoding vitamin D 25-hydroxylase), the region around DHCR7 (encoding 7-dehydrocholesterol reductase) and CYP24A1 (encoding 1,25-hydroxyvitamin-D3-24-hydroxylase). Variants in these four genes account for about 1.5% of the total variance. This may appear to be an inconsequential amount, but as will be demonstrated now, just a single variant in one of these genes can have almost as much impact on 25(OH)D levels as dark skin tone. It is important to remember these variants arose after all as adaptions to cope with lower and lower doses of UV-B exposure as early humans migrated out of Africa near the equator to ultimately the very high latitudes of Scandinavia and northern Asia.
The gene with the variant most closely associated with circulating 25(OH)D, GC (group-specific component) encodes the VDBP. The rs4588 A allele is particularly predictive for lower 25(OH)D concentrations in people with Caucasian ancestry. Elderly people in Switzerland with two copies of the rs4588 A allele, constituting about 8% of the local population, had about 36% lower levels than those without the A allele.17 Others have found smaller differences attributable to the rs4588 A allele, but the effect is consistently observed in European populations, though not in people with African ancestry. Contrary to common assumptions, the effect on 25(OH)D concentration of this genotype alone is comparable to the effect of dark skin.
Clinical relevance
Consequences of vitamin D deficiency for individual health and the COVID-19 epidemic
In the absence of sufficient UV-B exposure and dietary intake, 25(OH)D levels depend heavily on the release of stored vitamin D built up during periods of high vitamin D availability, most from heightened UV-B exposure. It is well documented that vitamin D stores decline and 25(OH)D levels greatly decrease during the dark season. Winter and spring levels at higher latitudes, such as in Central and Northern Europe, Canada and the northern half of the USA, commonly drop to half of the summer and autumn levels or less. People who are elderly, obese, have dark skin tones or carry genetic risk variants tend to be more severely affected than others living in the same region.
Deficient vitamin D status as indicated by low 25(OH)D levels undermines the maintenance of good health. There is little doubt that very low concentrations of 25(OH)D leave an opening for various health harms, from accelerated progression of osteoporosis,18 greater risk of falls,18 increased prevalence of obesity,11 heightened vulnerability to perinatal depression,19 impairment of glucose homeostasis,20 to reduced life expectancy and increased overall mortality,21 not least due to respiratory diseases.22 Thus, even if it turns out that a permissive effect of vitamin D deficiency for infection with SARS-CoV-2 and the health outcomes following from that infection does not exist, there is still broad consensus that nobody should be vitamin D deficient at any time, neither in winter nor in old age, neither due to obesity nor due to a dark skin tone or other genetic risk factors. As far as we know, vitamin D deficiencies in all of these situations can be remedied, it is just a matter of will and action. Numerous associations and governmental agencies already have clear policies in place to avoid vitamin D deficiency, but they are obviously not taken seriously enough.
A problem for eradicating vitamin D deficiency may be that there is too much of a focus on typical or average people, which leaves out some vulnerable individuals because they do not fit expected standards. Nutrition being a hard science, we must take into account the full spectrum of what we know when we want to be effective.23 This is where PN comes into play because this approach aims to take into account known conditions and vulnerabilities that affect nutrient needs.24 25 The goal should be to avoid deficiency, not to raise already sufficient blood levels. At this point, we are lacking clear guidelines for ensuring adequate vitamin D status for people with extra body fat, dark skin or common genetic risk variants. They do not constitute a negligible minority, but rather add up to a sizeable number. There is not much to guess when it comes to counting dark-skinned people living at high latitudes because we can easily see them in large numbers in states like Illinois, New York or New Jersey. The same goes for overweight and obesity. Finding out about genetic risk variants is a bigger challenge, but we know they are there and must not be ignored.
In the case of the current COVID-19 pandemic, vitamin D deficiency may provide the virus with an unguarded opening to spread from deficient to deficient individual when there are just too many of them. The spread of the virus may well proceed through a small number of individuals whose defences are weakened by vitamin D deficiency. The deficiency just has to be common enough that there is a sufficient number of people among the infected person’s contacts who are also deficient. In other words, every individual with severe vitamin D deficiency is a potential stepping stone for the virus to get to its next few victims. The majority of people with enough vitamin D would not matter much as long as there are enough stepping stones to bypass them. This could explain how only a few out of a large number of known contacts, at large sports events, church gatherings or popular concerts become infected. If some of the contacts have deficient vitamin D status and therefore an impaired immune defence, the reproduction number R0 may rise above the critical value of 1 and the spread of the virus will take off.
A more speculative consideration concerns the observation that children are much less affected by COVID-19. This could well be because they tend to be less likely to have severe vitamin D deficiency when they have plentiful playtime outdoors in the summer, and they also tend to have less fat mass than older adults. Children who do not get to play much outside or who are obese might still have a higher risk.
How can we know more?
A now well-established method for testing the effect of exposures, such as vitamin D, on outcomes, such as infection and death from SARS-CoV-2, is Mendelian randomisation.26 This approach takes advantage of the fact that some exposures are predictably influenced by inherited disposition and that the effect of the exposure on the outcome can be assessed more conveniently by using the inherited disposition as a proxy for the less easily measured exposure.
Here we want to test the hypothesis that vitamin D deficiency is a permissive factor for COVID-19-related outcomes. We can use the known fact that dark-skinned individuals need much more UV-B light to generate vitamin D in skin than light-skinned individuals.27 Thus, latitude of residence can serve as a proxy for vitamin D production in skin. Metrics of COVID-19 infections and deaths may then be compared with latitude in some crude approximation for testing the hypothesis.
In this context, the striking observation is now coming to light that, at least in the USA28 29 and the UK,30 many more dark-skinned people are infected and more are dying from the disease than light-skinned individuals. As mentioned above, dark skin tone tends to be associated with much lower vitamin D levels than light skin tones, particularly during the months of winter and early spring.
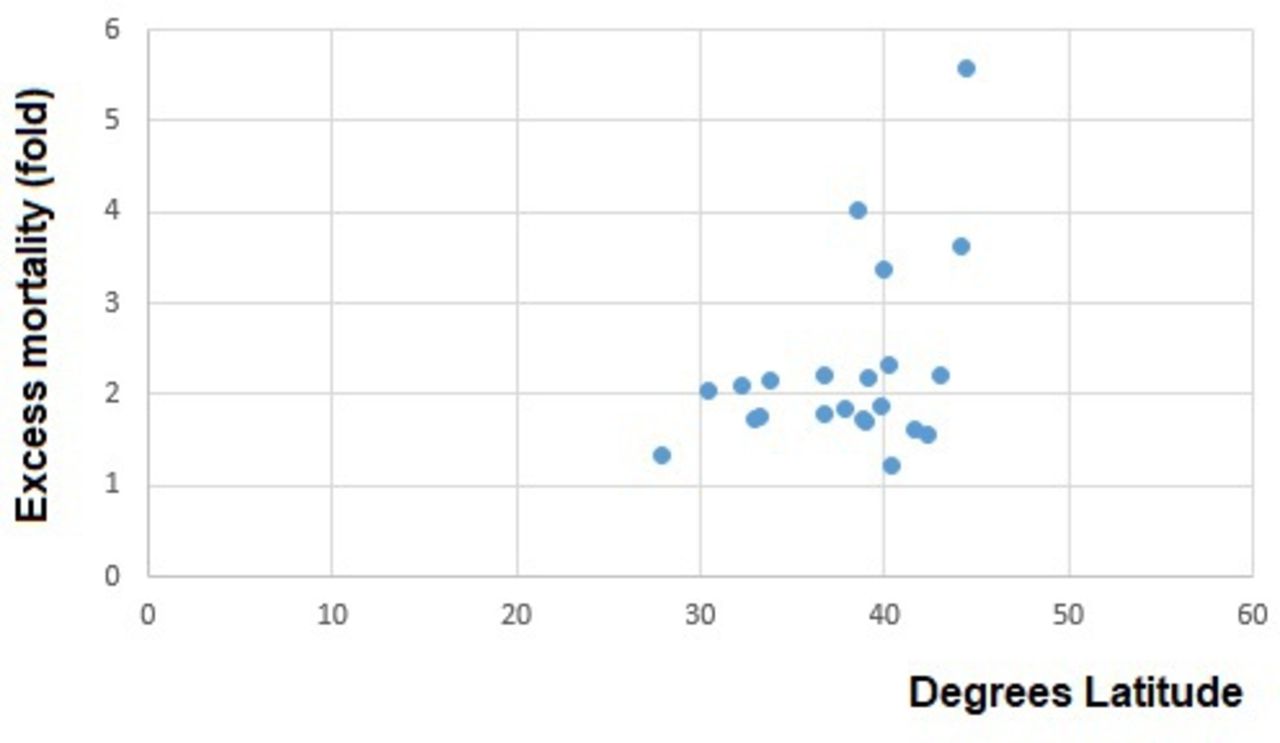
For conducting a Mendelian randomisation analysis, COVID-19 mortality data reported for the time until 16 April 202029 were used. The results of this crude comparison indicates a relationship of state latitude, the chosen proxy for vitamin D, with COVID-19 mortality in African-Americans (r=0.427, excluding the three states with 15 or fewer cases, see table 1) and less clearly in the others (r=0.352). The mortality excess of African-Americans (ratio of percentage of African-Americans among those who died with a COVID-19 diagnosis in the state to percentage of African-Americans among the state population) was related to the nominal latitudes of the reporting states (r=0.435, figure 1). Accordingly, the over-representation of African-Americans among COVID-19 deaths was much greater in the northernmost US states with sufficient data (Wisconsin, 5.6-fold; Michigan, 3.6-fold and New York, 2.2-fold) than in the southernmost states (Alabama, 2.1-fold, Louisiana, 2.0-fold and Florida, 1.3-fold). As should be expected, the steepest gradient was apparent between about 44° North (Wisconsin) and near 40° North (New Jersey). The intensity of UV-B is too low at latitudes above 40° during winter and spring to generate vitamin D in skin, assuming that anybody was even tough enough to bare their skin to the dim sun for extended periods of time. The higher the latitude the longer the period without vitamin D production extends into March and April.27 31

{kind=link}
Correlation of excess mortality of African-Americans with average latitude of their state of residence (r=0.435, 22 states, p=0.02). Data were collected until 16 April 2020. States with fewer than 16 deaths of African-Americans (Washington, Minnesota and Arizona) were excluded. The data were extracted from reporting by Associated Press News.29
African-American (AA) population frequencies and mortalities as of 16 April 202029
Of course, numerous types of racial disparities, such as social status, healthcare access and pre-existing health conditions, are of importance and could not be taken into account for this preliminary analysis as they eventually should. While these numbers are necessarily tentative and are lacking the appropriate adjustments, they provide a real-life hint on the importance of vitamin D deficiency for the current COVID-19 epidemic in the USA. The effect is most likely to be modest and the amounts of additional vitamin D intake needed to level the difference between northern and southern states is relatively small.
A Brookings report based on a smaller number of states suggests that a similar racial disparity exists in regard to infection rates, with greater excess infection rates in Michigan and Illinois to the north28 than in the Carolina’s further south. These data thus far do not support calls for very high vitamin D intake or excessive UV-B exposure. The difference in vitamin D synthesis between Wisconsin (44.5° North) and Florida (28° North) might result in an estimated difference of 7.2 ng/mL (18 nmol/L) in blood 25(OH)D concentration. The Northeners would have to get an extra dose of about 240 IU per day to make up for the shortfall in 25(OH)D concentration. The estimate is based on data extracted from Jääskelainen et al 32 and Mendes et al.27 It needs to be understood that this estimate is only meant to address the gap in excess deaths of African-Americans from COVID-19 and would have to be on top of the amount needed to cover their basic needs, which in dark-skinned people are already higher than in light-skinned ones.
How much vitamin D should people get?
A very important first step would be to ensure that all people get at least as much vitamin D with a dietary supplement as recommended for the various countries. The recommended daily amount is 400 IU in the UK. US recommendations are 600 IU for adults up to 70 years of age, and 800 IU for people over the age of 70.33 Individuals with known risk factors need more, but current recommendations are silent on their specific needs. Higher intakes are likely safe as long as the amounts are well under 4000 IU per day.
Conclusions
We have known for a long time that 25(OH)D concentrations of people living at high latitudes drop due to the lower daily UV-B light exposure during the dark months of the year. And still, not enough is done to offset the typical seasonal drop in 25(OH)D concentrations at higher latitudes by using appropriately dosed vitamin D supplements. Now in the context of the current COVID-19 pandemic, renewed attention to the very high prevalence of severe vitamin D deficiency there and elsewhere is in order. Advanced age, obesity, dark skin tone and risk-related genotypes, particularly in combination, are alarm signs that should prompt corrective action, typically with a moderate, individually tailored dose of supplemental vitamin D. While the preventive potential of supplemental vitamin D should not be exaggerated and the dose kept within recommended ranges (typically well under 4000 IU per day), preventing vitamin D deficiency should be a widely shared goal.
References
Footnotes
Contributors MK is the sole author of this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All the data used is in the public domain and comes from the cited sources.