Article Text

Abstract
Objective Poor diet is a leading cause of death worldwide. Doctors are well placed to provide dietary advice, yet nutrition remains insufficiently integrated into medical education. Enforcement of curriculum or accreditation requirements such as nutrition requires relevant regulatory frameworks. The aim of this review was to identify nutrition content or requirements for nutrition education in accreditation standards or formal curriculum guidance for medical education internationally.
Design Non-systematic comparative analysis.
Data sources An internet search using the Google Search engine, the WHO Directory of Medical Schools and Foundation for Advancement of International Medical Education and Research Directory of Organizations that Recognise/Accredit Medical Schools was conducted through September 2020 to identify government and organisational reports as well as publications from regulatory and professional bodies relevant to medical education.
Eligibility criteria Eligible publications included (A) accreditation standards, (B) competency standards or a framework, (C) curricula, and (D) assessment content.
Data extraction and synthesis We stratified findings by country or region and both preregistration and postregistration education. Findings were synthesised based on the existence of nutrition content or requirements for nutrition education within systems used to guide medical education internationally.
Results This review found that despite an emphasis on meeting the needs of the community and the demands of the labour market, only 44% of accreditation and curriculum guidance included nutrition. Nutrition remains inadequately represented in accreditation and curriculum guidance for medical education at all levels internationally. Accreditation standards provide a mandated framework for curricula and inclusion of nutrition in accreditation frameworks provides an incentive for the integration of nutrition into medical education.
Conclusions This review is a call to action for the medical profession including government, health agencies and educational and accreditation entities. The inclusion of nutrition in medical education has appeared throughout medical education literature for more than five decades, yet without consensus standards there is little likelihood of uniform adoption.
- preventive counselling
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
Doctors are well-placed to provide dietary advice, yet nutrition remains insufficiently integrated into medical education.
Despite an emphasis on meeting the needs of the community and the demands of the labour market, review of global medical regulation identified less than half of accreditation and curriculum guidance included nutrition.
To incentivise inclusion of nutrition in medical education, it must be embedded within curriculum or accreditation requirements, and part of relevant regulatory frameworks.
This top-down approach may be necessary to finally make progress to increase nutrition knowledge and skills in medical professionals.
Introduction
Poor diet is a leading cause of death worldwide.1 The WHO estimates that approximately 80% of non-communicable diseases could be prevented by following a healthy diet, staying physically active, avoiding tobacco and consuming alcohol in moderation.2 The United Nations (UN) Decade of Action on Nutrition and the ICN2 Framework for Action underscore the need for scalable health workforce capacity in nutrition to end malnutrition in all its forms.3 4 Doctors are well placed to provide dietary advice and are perceived by those in their care to provide trustworthy and individualised nutrition care.5 6 General practitioners, in particular, have the potential to elicit improvements in nutrition behaviour and risk factors in individuals with lifestyle-related chronic disease, and are powerful role models.5 Their regular contact with large numbers of individuals also provides opportunities for referral to other nutrition services, such as dietitians, where further expertise is required. Despite this, there is evidence that physicians are not capitalising on opportunities to provide nutrition care to patients with chronic disease. For example, obese patients reported receiving dietary counselling during only 25% of clinic visits7 and a Centers for Disease Control and Prevention report has noted a 10% decrease in the frequency of preventive counselling provided between 1996–1997 and 2007–2008.8 In order to provide nutrition care as part of routine clinical practice, doctors require the relevant nutrition knowledge, skills and attitudes (competence). However, despite the centrality of nutrition to health, it remains insufficiently integrated into medical education, regardless of country, setting or year of medical education.9 Deficits in medical nutrition education present an ongoing barrier to the provision of nutrition care in practice.9
According to the World Directory of Medical Schools, a joint initiative of the World Federation for Medical Education (WFME) and the Foundation for Advancement of International Medical Education and Research (FAIMER), there are 3387 medical schools currently operational internationally.10 Accreditation systems are used to ensure the quality of medical education, facilitated by medical schools, and can be institutional or programmatic and voluntary or mandatory.11 Accreditation has been linked to improved medical student outcomes.11 According to the WHO and WFME, the purpose of accreditation and quality improvement in medical education is to ‘adjust medical education to changing conditions in the health care delivery system and to prepare doctors for the needs and expectations of society’.12 A limitation of the accreditation process is the potential for mismatch between the agreed-upon content of medical education and community needs.12
Our previous research has highlighted potential competencies for nutrition in medical education. However, without a regulatory framework to enforce this, it will always be difficult to implement. Fundamental to improvements in medical nutrition education and subsequent nutrition practice behaviour is the need to first identify any formal expectations for nutrition education by regulatory bodies including accrediting bodies, and representatives of the medical profession. Accreditation standards (regulations) provide an incentivised blueprint for curricula, by setting a benchmark for outcomes, the process of educational delivery and in some cases required programme content.13 Amending accreditation standards to require nutrition education as a formal outcome would provide incentive to include nutrition in medical education programmes in order to receive and maintain accreditation. Therefore, the aim of this review was to identify nutrition content or requirements for nutrition education in accreditation standards or formal curriculum guidance for medical education internationally. It is anticipated that the results of this review will provide insight into formal opportunities to integrate nutrition into medical education.
Methods
For the purposes of this review, we initially defined key concepts and terms based on published definitions and author experience (table 1).14
Definitions of key concepts and terms related to medical education used within this review
This review took a pragmatic approach to search and identify literature. An internet search using the Google Search engine was conducted through September 2020 to identify non-peer-reviewed government and organisational reports as well as publications from regulatory and professional bodies relevant to medical education and training. The WHO Directory of Medical Schools and FAIMER Directory of Organizations that Recognise/Accredit Medical Schools were used to identify relevant literature for this review.15 16 Specifically, we identified regulatory bodies in medicine in each continent, and in specific countries, and searched for standards (typically identified as accreditation standards) or curriculum policy (including competency standards or a framework and guidelines for curricula and assessment) for medical education and training using keywords related to medical education, accreditation and regulation. Keywords included terms of ‘medical education’, ‘standards’, ‘regulation(s)’, ‘accreditation’, ‘competencies’ and ‘curriculum’. Eligible types of publications included the following: (A) accreditation standards, (B) competency standards or a framework, (C) curricula, and (D) assessment content. Where a publication was not available in English, the Google Translate website (https://translate.google.com.au) was used to translate the information to the English language.17
We examined key professional medical documents, namely guidelines for accreditation and curricula, to identify the existence of nutrition within these systems for medical education and training internationally. For the purposes of this review, nutrition was defined as any explicit or implicit reference to ‘nutrition processes as well as the components of food, their actions, interaction and balance in relation to health and disease’.18 The search function in Microsoft Office was used to identify explicit terms such as ‘diet’, ‘nutrition’ and ‘food’. Following this, each document was reviewed in full to identify other (implicit) references to nutrition. For example, concepts related to food hygiene, breast feeding and fluid and electrolyte balance, and skills such as anthropometric assessment were considered a reference to nutrition. For reporting of results, at least one exemplar country was selected from a group of countries or regions, which represent a similar model of medical education. All findings were stratified by country or region following the typical chronological career path of a medical student. Findings were synthesised based on the type of guidance (accreditation standards, competency standards or a framework and guidelines for curricula and assessment) to identify the existence of nutrition content or requirements for nutrition education in systems used to guide medical education.
Patient and public involvement
There are no patient and public involved in the study.
Results
Accreditation standards and curriculum guidance (including competency standards or a framework and guidelines for curricula and assessment) (n=57) from 20 countries and 40 organisations were included and grouped into eight regions for review (table 2).
Organisations involved in guidance for medical education for each region included in this review
Although similar numbers of documents were sought across continents, only two documents were obtained from South America, and only two documents were included from all of Asia (two from China) (table 3). Less than half (25/57) of the documents in this review included nutrition (table 3). There was no pattern regarding the amount or scope of nutrition in medical accreditation and curriculum guidance between individual organisations, countries or regions. Generally, the number of documents that included any reference to nutrition was less in Europe (31%) compared with the African region (4/7; 57%) and India, Sri Lanka, Nepal and Bangladesh (5/9; 56%). Accreditation and curricula policy and guidance for medical education and training in South America did not include any reference to nutrition.
Accreditation and curriculum documents including nutrition per country or region
Just over half of the documents included in this review (n=30/57) were accreditation standards or regulations, with a relatively even split between preregistration (30/57) and postregistration (27/57) medical education (table 4). Only two documents outlined assessment.
Number and type of documents included in this review by stage of medical education
Twenty-five of the documents included any reference to nutrition, with 14 of these related to preregistration (table 4). Requirements for nutrition education were most frequently found in a curriculum framework or syllabus (n=11/25) followed by a competency framework or educational outcomes (8/25). The two documents referring to assessment included requirements for inclusion of nutrition education in this assessment (2/25) (table 4).
Accreditation standards
Many of the accreditation standards included in this review were limited to academic and professional outcomes such as purpose, criteria for admission, faculty requirements, administration and evaluation. National accreditation standards for preregistration in China, India and Nigeria included requirements for nutrition education (table 5). Four accreditation standards included nutrition, and as these standards form part of a formal regulatory framework, the nutrition education in these countries is mandated. Requirements for nutrition education in accreditation standards and regulation were stipulated (A) competencies19 or (B) an education programme or curriculum20–22 for medical education. Nutrition was integrated into subjects (eg, human anatomy)19–21 or by medical specialty (postregistration) (eg, surgery).22
Accreditation and curriculum documents including nutrition
In China, the Working Committee for the Accreditation of Medical Education provides mandatory accreditation of undergraduate (basic) medical programmes under the authority of the Ministry of Education and former Ministry of Health. The Accreditation Standards for Basic Medical Education in China stipulate that the medical school must, in the curriculum, ‘identify and incorporate the contributions of public health sciences’, including nutrition and food hygiene, ‘to develop students’ awareness of population health and disease prevention strategies, allowing them to function well in health education, promotion and management efforts’ and ‘introduce complementary medicine and their roles’, such as food and food therapies.21
Medical education in India is regulated by the Medical Council of India (MCI), which makes accreditation recommendations to the Indian government. To fulfil the roles of the profession, this council stipulates that the Indian Medical Graduate would have obtained a set of competencies delineated by domain (roles) at the time of graduation. This includes the ability to ‘prescribe and safely administer appropriate therapies including nutritional interventions…’ across the care spectrum and demonstrate an understanding of the ‘importance of nutrition in health and disease…’.19 Regulation for undergraduate medical education in India also includes items on how to integrate competencies horizontally and vertically to ‘enable students to make clinical correlations…’.19
Curriculum framework or syllabus
Less than half (5/11) of curriculum guidance for medical education in this review which included nutrition is mandated (table 5). Requirements for nutrition education in curriculum guidance were embedded in (A) a topic or content list,23–25 (B) a competency-based curriculum,23 26–28 (C) clinical training guidance,29 30 or (D) learning objectives and/or descriptors.31 32 Nutrition education was integrated into recommendations for clinical skills curricula, which are not a stipulation, but provide guidance regarding ‘the design and implementation of clinical skills curricula in the undergraduate medical experience’.30
The MCI’s national Competency-Based Undergraduate Curriculum for the Indian Medical Graduate includes mandatory competencies related to nutrition assessment, intervention and dietary counselling.26 The model of undergraduate medical education in India is unified in that the MCI Graduate Medical Education Regulations (accreditation standards) provide global competencies defining the roles of the Indian Medical Graduate which are aligned with ‘sub-competencies’ and suggested learning experiences outlined in the national competency-based curriculum.19 26 The curriculum guidance is relatively specific with regard to nutrition.
The curriculum is organised by subject and phase (eg, preclinical subjects such as physiology and medicine and allied health subjects such as community medicine). The MCI curriculum for undergraduate medical education in India also indicates subjects within the same phase and other phases for teaching of a topic. For example, the medical graduate should be able to ‘discuss the nutritional requirements of surgical patients, the methods of providing nutritional support and their complications’.26 The curriculum suggests this competency may be vertically integrated into preclinical biochemistry and suggested teaching/learning methods including lecture, small group discussion and bedside clinic. The curriculum also includes instruction on deriving assessment methods from competencies; for example, skill-based assessment methods such as bedside clinic or a ‘Demonstrate, Observe, Assess, Perform’ session are recommended for development of the ability to ‘assess and counsel a patient in a simulated environment regarding appropriate nutrition in pregnancy’.26
While not mandatory, the Curriculum for Undergraduate Medical Education in Bangladesh, set by the Bangladesh Medical and Dental Council, has some similarities with the curriculum for undergraduate medical education in India in that the curriculum is organised by subject (eg, physiology, health education) and includes instruction on teaching/learning strategies, time dedicated to content and assessment methods.31 The curriculum includes over 40 learning objectives related to basic principles of food and nutrition, the role of nutrition in health and diet prescription.31 The Curriculum for Undergraduate Medical Education in Bangladesh also recommends integration of particular topics across multiple subjects, also known as spiral learning theory, where a topic is revisited multiple times throughout the learning journey for consolidation and to provide context on old learning.33 For example, the learning objective ‘describe common nutritional disorders of the country’ could be integrated into both community medicine and paediatrics.31
Competency frameworks
Four of eight (50%) of competency frameworks which included requirements for nutrition education in this review are mandated (table 5). Requirements for nutrition instruction were integrated into competency frameworks as (A) competencies34–37 or (B) broad learning outcomes or objectives.21 34 35 38–40
Medical education in Egypt is regulated by the National Authority for Quality Assurance and Accreditation of Education (NAQAAE), an independent entity who provides voluntary accreditation. The NAQAAE National Academic Reference Standards (NARS) for the medical sector represent the ‘minimum academic quality requirements’ to protect the interests of students and the community. The NARS—Medicine recommend the medical graduate be able to ‘discuss the role of nutrition and physical activity in health’ and conduct nutrition assessment including anthropometric measurements as fundamental physical examination skills.36
The General Medical Council (GMC) set mandatory standards and expected outcomes for all stages of medical education and training in the UK. The 2018 GMC Outcomes for Graduates is a regulatory framework and provides the basis for UK medical schools to develop medical school curricula. The outcomes are organised under three domains: outcome 1—professional values and behaviours, outcome 2—professional skills, outcome 3—professional knowledge.38 Within outcome 1, newly qualified doctors in the UK must be able to ‘identify factors that suggest patient vulnerability and take action in response’ including the contribution of poor nutrition to ill health.38 Within professional knowledge, newly qualified doctors in the UK are required to apply principles, methods and knowledge of nutrition and population health to medical practice and integrate these into patient care.38
Postgraduate medical education in Spain is coordinated by the Spanish Ministry of Health. Postgraduate programme curricula are set by national specialty boards, which are regulated through site visits by government experts. Endocrinology and nutrition is a recognised specialty in Spain, for which the current training programme is prepared by the National Commission for the Specialty of Endocrinology and Nutrition and is verified by the National Council of Medical Specialties, the Human Resources Commission of the National Health System and the Ministry of Education and Science.37 General and specific objectives and competencies of the specialty are written into Spanish law and therefore mandated.37 General objectives of the specialty include the ability to ‘understand the pathophysiology, investigate and recognize the clinical manifestations, as well as practice appropriate preventive, diagnostic and therapeutic actions… in alterations of metabolism and human nutrition’. Mandatory competencies of the specialty of endocrinology and nutrition in Spain include malnutrition, eating disorders, overweight and obesity, and ethical and legal aspects of clinical practice in nutrition.37
Assessment or examination content
Only two assessment or examination outlines were identified and both of these included nutrition (table 5). Requirements for nutrition education were integrated into examination content for the state medical licensure examination (Approbation) in Germany, which is written into law,41 and the content outline for the US Medical Licensing Examination, sponsored by the Federation of State Medical Boards and the National Board of Medical Examiners.42
Requirements for undergraduate medical curricula in Germany, including number of classes, minimum requirements and content for state board examinations, are defined by federal officials of legislature and are written into law as the Licence to Practise Medicine.41 Each university has the autonomy to execute these requirements as they see fit, resulting in location-specific undergraduate medical curricula. However, as students are required to pass the examination to acquire medical licensure in Germany, it is likely the assessment outline will inform curricula. Content for the medical licensure examination in Germany includes ‘applied physiology including nutrition’ and ‘basics of nutrition’.41
Global guidance on medical education
The WFME is a non-governmental organisation whose main objective is to ‘enhance the quality of medical education worldwide, with promotion of the highest scientific and ethical standards in medical education’. The WFME global standards programme provides a framework for national or regional accreditation as well as for reform and quality improvement. The Basic Medical Education: WFME Global Standards for Quality Improvement and the Postgraduate Medical Education: WFME Global Standards for Quality Improvement do not include requirements for nutrition education.43 44
Discussion
This review provides preliminary evidence that explicit nutrition content or instruction on nutrition education is missing from important accreditation and formal curriculum guidance for medical education internationally. Although there was emphasis on meeting the needs of the community and the demands of the labour market, only 45% of accreditation and curriculum guidance mentioned nutrition, or included requirements for nutrition education in this review.
Accreditation systems have been adopted internationally for quality control and quality improvement in healthcare and have been shown to improve the provision of care.45 46 For example, programmatic accreditation standards which encompass breast feeding were reported to improve rates of breast feeding.47 While approximately half of the documents included in this review were accreditation standards for medical education, only 20% of these included nutrition. Despite emphasis on health prevention, very few accreditation standards in this review require nutrition education. Nutrition remains insufficiently integrated into medical education, regardless of country, setting or year of medical education.9 In contrast, concepts related to pharmacotherapy are consistently represented in accreditation and curriculum policy for medicine (data not shown). For example, accreditation standards for undergraduate medical education in Nigeria state the medical graduate should ‘Understand the principles of writing medical prescriptions and be able to write prescriptions for common manifestations of disease…’.20 While pharmacotherapy is obviously an essential competency for doctors to demonstrate proficiency, the centrality of nutrition to health promotion and disease prevention may also be considered essential.1 Many guidelines focus on treatment of disease where nutrition is relevant across the spectrum in both prevention of disease and treatment in certain conditions. Improvement of diet could potentially prevent one in every five deaths globally and there is potential for doctors to support nutrition care, as they are often the first point of contact to the healthcare system for most individuals.1 Furthermore, nutrition care has been shown to improve health outcomes with reduced risk, side effects and costs when compared with pharmacological interventions.48 A culturally sensitive paradigm shift must take place, whereby nutrition care is embraced across the care continuum as an evidence-based first-line intervention, just as pharmacotherapy is.
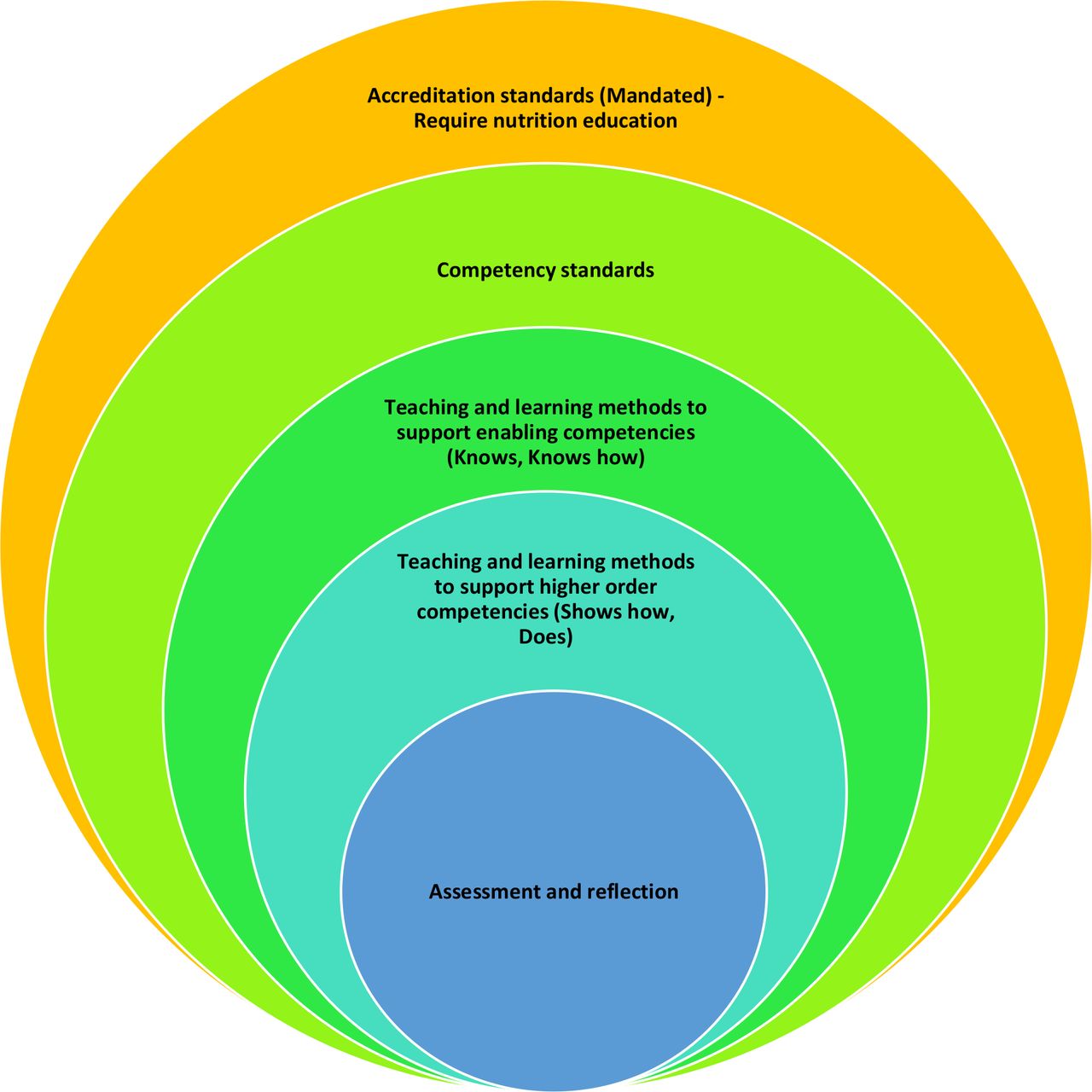
Accreditation standards provide a mandated framework for curricula and therefore the inclusion of nutrition in accreditation frameworks will provide incentive for the long-awaited integration of nutrition in medical education. An example of where nutrition is formally included in accreditation standards for medical education is India. Despite being one of the largest medical education systems in the world, comprising 457 operational medical schools, the competency-based system is considered standardised and in keeping with recent global trends.10 49 As India produces many physicians who emigrate internationally, the quality of Indian medical education has relevance globally.50 Accreditation in India is compulsory, and standards for medical education require medical schools meet a defined set of competencies, which include nutrition.19 26 The use of competency-based education in improving medical nutrition education has been previously established51 and has been shown to increase a clinician’s ability to integrate nutrition into patient care.52 This system is illustrative in using regulation and quality assurance entities to drive health education reform. While the curriculum might be considered prescriptive, the standards require nutrition competency for medical graduates. Therefore, there is incentive for nutrition to be formally integrated into the medical curriculum to receive and maintain accreditation. Amending accreditation standards to require nutrition competency has been previously recommended as a policy lever for the inclusion of nutrition in medical training.53 Without incentive, nutrition will continue to fall through the cracks. Figure 1 provides a conceptual representation of the relationship between the accreditation system, namely accreditation standards which require nutrition education, and the subsequent development of nutrition competency as informed by Miller’s Pyramid of Assessment.54 However, there is a lack of consensus on required nutrition competencies for medical professionals.9 Consensus on core or minimum nutrition competencies for medicine must first be established as a global benchmark for accreditation.
{kind=link}
Illustration depicting the use of accreditation systems to drive the integration of nutrition in medical education.
If mandated accreditation standards require competency in nutrition, there is incentive for medical education providers to prioritise nutrition education to maintain accreditation. On a local level, development of nutrition competency must be supported by varied and innovative teaching and assessment methods (figure 1). If schools can adapt or replicate existing nutrition education interventions which have been successful elsewhere, this increases the likelihood that nutrition will be included in curricula. Nutrition education interventions that have proved effective include hands-on culinary medicine training, simulation-based training with deliberate practice, interprofessional and multidisciplinary team-based education and technology-based learning or resources.9 55–60 Of interest, doctors with a healthy personal lifestyle are more likely to provide behaviour counselling to patients than doctors with less favourable health behaviours.61 Competency can be considered a journey, and while knowledge-based nutrition competencies are essential to interpret new concepts, higher order skill-based and attitude-based competencies underpin the application of nutrition in clinical practice.54 Skill-centred training in nutrition has been shown to improve medical students’ confidence in lifestyle counselling and the delivery of nutrition care in practice by medical clinicians.56 62 This is of importance, given the plethora of evidence, which suggests medical students and clinicians alike do not feel adequately prepared to provide nutrition counselling to their patients and identify poor translation of nutrition to a clinical context as a barrier to nutrition care in practice.9 63–67
Ultimately, regulatory frameworks including nutrition would aim to improve outcomes for those receiving medical care. Nutrition education interventions which encompass a combination of individual, social and environmental changes have been shown to improve nutrition-related health outcomes in Indigenous Australian populations, a typically underserved community.68 The inclusion of participatory nutrition education in medical training may promote understanding of wider social determinants of health and public health inequities. The 2019 report ‘Doctoring Our Diet’ recommends federal and state grant funding as a viable incentive-based model to support medical schools to provide nutrition education by covering up-front costs required to adapt curricula, develop teaching and learning methods, train teachers and assess impact.53 Successful nutrition education initiatives provide a model for the innovative integration of nutrition in medical education. However, this approach relies on voluntary action without addressing the need for mandatory nutrition education in formal standards.
A scarcity of faculty for teaching of nutrition education and limited collaboration with nutrition professionals have been identified as barriers to the adequacy of medical nutrition education.66 Interprofessional education (IPE) has gained momentum internationally and is recognised by the WHO as an ‘innovative strategy that will play an important role in mitigating the global health workforce crisis’.69 Research reports that IPE can lead to downstream improved patient outcomes and measurable and significant improvements in interprofessional and collaborative competencies for medical students, as outlined by the Interprofessional Education Collaborative.57 70 Interprofessional nutrition education is considered an essential component of medical training and may therefore be an effective tool for the delivery of nutrition education.71 It is the position of the Academy of Nutrition and Dietetics that registered nutrition professionals (such as dietitians) represent a highly valuable resource and should play a significant role in medical nutrition education.71 Nutrition professionals can model the effectiveness of nutrition care and promote the centrality of nutrition in health and disease.9 66 71 72 Furthermore, interprofessional nutrition education fosters a mutual appreciation of the role of other professions in patient care and promotes the perception of their own role in an interprofessional team, including recognition of when a referral to another health professional is required, such as a dietitian, who is able to provide specialised nutrition advice.9 71 73 Many teaching settings and strategies have been suggested for nutrition professionals to take a leadership role in preparing future doctors to initiate dialogue around nutrition and health with their patients, consult with nutrition experts (such as dietitians) and refer patients for medical nutrition therapy.71 For example, at one medical school, an interprofessional case-based approach to teaching nutrition counselling led to statistically significant improvements in confidence to provide nutrition counselling and collaborative competency among first year medical students.57 Again, without the requirement for nutrition education in formal standards, it is unlikely that nutrition professionals can prioritise nutrition as part of IPE. Nutrition professionals have an important role in championing the integration of nutrition into medical education. Furthermore, they have the potential to be involved in the development of accreditation standards and competencies for medical education by ensuring adequate representation of nutrition in educational standards and assessment.74
Strengths and limitations
There are several strengths to this study. First, this review provides preliminary evidence that requirements for nutrition education are poorly represented in important accreditation and curriculum guidance for medical education internationally. This review provides new insight into how accreditation systems might be used to mandate nutrition competency. This review calls for accrediting entities to amend accreditation standards to require nutrition education. This would provide formal incentive for medical education providers to integrate nutrition into education in order to maintain accreditation status. However, limitations do exist. We may not have included all relevant documentation despite attempts to be representative internationally and as comprehensive as possible. Differences in education and accreditation systems, health systems and medical terminology may have limited our ability to identify but also summarise information. Although many documents were available as translated English documents, the translation may also have limited our ability to identify relevant concepts in documents. The lack of consensus on relevant nutrition competencies for medicine might be considered a limitation to the integration of nutrition in accreditation systems, as recommended by this review.
Conclusion
This review found that nutrition remains inadequately represented in important accreditation and curriculum guidance for medical education at all levels internationally. This presents both a barrier and opportunity to medical nutrition education. As we approach the halfway mark in the UN Decade of Action on Nutrition (2016–2025), this review is a call to action for the medical profession including government, health agencies and educational and accreditation entities to do better. There is a need to assess consensus on relevant nutrition competencies for the medical workforce, and for accreditation standards to require nutrition education. The inclusion of nutrition in medical education has appeared throughout medical education literature for more than five decades, yet without consensus standards there is little likelihood of uniform adoption.
References
Footnotes
Contributors BL, EB, KJM and SR contributed to the design of the review. BL did the literature search, performed data analysis and drafted the manuscript. All authors contributed to revision of the manuscript and approval of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no data sets generated and/or analysed for this study.