Article Text

Abstract
Background Healthy pregnancy and birth outcomes are greatly influenced by the intake of adequate and balanced nutrition. Pregnant women’s nutritional knowledge and practice have been identified as an important prerequisites for their proper nutritional intake. The antenatal period with the opportunities for regular contact with health professionals appears to be the ideal time and setting to institute the intervention which could maximise pregnant women’s outcome and that of their baby by motivating them to make nutritional changes.
Objective To assess the effect of nutrition education on the appropriate nutritional knowledge and practice of pregnant women.
Methodology A facility-based single-group pre–post quasi-experimental study design was employed in five health facilities providing antenatal care (ANC) service in Asmara on 226 pregnant women. A predesigned and pretested questionnaire was used to collect data regarding nutritional knowledge via interview by trained data collectors during the pretest, immediate post-test and 6 weeks later. The practice was assessed at pre-intervention and 6 weeks later only. Repeated measures analysis of variance and paired t-test were used to make comparisons in knowledge and practice scores, respectively, using SPSS (V.22).
Results Training provided to pregnant women resulted in a significant increase on the mean scores of their knowledge from 29.01/47 (SE=0.35) pre-intervention to 42.73/47 (SE=0.24) immediate post-intervention. However, the score declined significantly from immediate after intervention to 6-week follow-up by 1.79 (SE=0.22). Although the score declined, knowledge at 6-week follow-up was still significantly greater than that of pre-intervention (p<0.0001). Health professionals (70.2%) were the primary source of information for pregnant women. The pregnancy-specific dietary practice score at 6-week follow-up (M=13.13/16, SE=0.09) was significantly higher than that of pre-intervention (M=12.55/16, SE=0.16). There was no significant interaction between the categories of demographic characteristics and change in practice and knowledge.
Conclusion This study has shown that the nutrition messages given to pregnant women by trained health professionals using a holistic approach in a sustained manner played a huge role in increasing their knowledge and in introducing positive dietary practices among them. Thus, ANC clinics must play a leading role in coordinating the effort of awareness creation regarding nutrition during pregnancy.
- dietary patterns
- malnutrition
- nutrition assessment
- preventive counselling
- weight management
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
Timely provided nutrition education and counseling
Trained Antenatal care providersChange in pregnant women’s nutritional knowledge and dietary behavior
Improvement in maternal and child health
Background
Nutrition is a central and fundamental pillar of human life that is required for health and development throughout the entire life span in general and during pregnancy in particular.1 A pregnancy diet which is sufficient in energy, with a variety of nutrients, minerals and vitamins, and the mother’s avoidance of toxins and contaminants is important to ensure health for the mother and the growing fetus.2 3 In addition to that, poor quality diet during pregnancy has been found to be associated with unhealthy maternal weight gain, preterm birth, anaemia and low birthweight (LBW) babies which grow and develop less well and have poorer chance of survival than normal birthweight babies.2–7
Adequate and balanced nutrition during gestation has been recognised as a prerequisite for a healthy pregnancy and birth outcomes and this is significantly determined by their nutritional knowledge and practice.5 8–10 The WHO recognised the impact of nutrition in pregnancy and recommends that antenatal care (ANC) providers should provide adequate, specific and acceptable nutrition-related advice to their clients during every visit of antepartum. It is well studied that education holds a key factor in health promotion. Though knowledge is not behaviour, it determines the dietary behaviour. Hence, the antenatal period with the opportunities for regular contact with health professionals appears to be the ideal time and setting to institute the intervention which could motivate mothers to make changes that could maximise their outcome and that of the baby.2 11
Protein energy undernutrition and micronutrient deficiency have been associated with infant and maternal mortality, and Eritrea is no different from the many countries suffering from infant and maternal mortality. Eritrean Demographic Health Survey of 2002 came up with 2% of women, who are shorter than 145 cm, the cut-off point below which a woman is said to be at risk of giving birth to an LBW baby. It also indicates that 37% of women aged 15–49 years have a low body mass index indicating chronic energy deficiency.12 Despite that fact, it is not uncommon to observe women to eat less during pregnancy to avoid fatty babies and so to prevent difficult delivery.13 A section from Eritrean Population Health Survey (EPHS) 2002 also showed that only 4 in 10 mothers received iron tablets but almost all took the tablets for less than 60 days despite a 55% prevalence of anaemia among pregnant women, although the 2010 EPHS showed a 57.3% rate of iron consumption among pregnant women within their last birth.14 15 Such observation was also witnessed in several other countries where men are given more food than women due to a belief that men need more food because they work harder. Moreover, it is true that misconceptions and food taboos governing pregnancy still exist. This was due to the belief that certain food items will be plastered on the fetal head, fear of abortion, fatty baby and stillbirth.13 16
This study thus aimed at filling the gap of studies on the effect of educating pregnant women about pregnancy-specific nutrition on their appropriate nutritional knowledge and practice. The attainment of satisfactory knowledge and practice can ultimately result in adequate maternal diet, optimal maternal weight gain and positive infant outcomes such as satisfactory birth weight. The study will also serve as a baseline for studies and programmes working on interventions to improve national and global nutrition status of pregnant women. The intervention of this study, training and nutrition education (NE) at the ANC, and materials used can also be duplicated to cover the gap of NE in the area and the country as a whole. This research basically employed the Health Belief Model which is based on the premise that people are most likely to take health-related action (eg, eat a healthy diet), if they feel that by doing so they can avoid a negative health condition.
Method
Design and study place
A facility-based single-group pre–post quasi-experimental study design was employed from July to September of 2018 in Asmara, the capital city and largest settlement in Eritrea. According to the Municipality of Asmara, there are a total 114 640 households in the city and it is home to a population of around 416 367 people with 227 337 of them being women.
Study population
There are 18 health facilities in Asmara out of which 17 provide ANC service. Of these 3 are health centres, 3 are community hospitals and 11 are health stations. The community hospitals have a catchment population of around 50 000 and they provide service for more than three subzones. There are approximately 59 healthcare providers in the facilities. The health facilities which provide ANC service are geographically located in four subzones: Northern West Asmara, Northern East Asmara, Southern West Asmara and Southern East Asmara. The geographical regions along with their corresponding health facilities are shown in table 1 (online supplemental table 1). First and second trimester pregnant women who were attending ANC in the health facilities during the study period were the study population.
Supplemental material
Demographic characteristics of the study participants (n=215)
Sample size
Sample size was calculated using a G-power V.3 calculator using a test family of t-test. Difference between two dependent means (matched pairs) technique was used with an effect size of 0.2, with actual power and level of significance of 0.80 and 0.05, respectively. The sample size calculated was 199. Considering 10% dropout from follow-up, a final sample of 220 was determined.
Sampling technique
Stratified random sampling was used to select the study participants. The four geographical regions/subzones are considered as strata because of the similarity of the pregnant women within each subzone and differences of the pregnant women in one region/subzone with another one. Hence, each region contributed one health facility to bring about representative pregnant women from the four subzones, except in Southern West Asmara in which two health facilities were taken. The randomly selected health facilities from each subzone along with the number of pregnant women who visited the selected health facilities and samples taken are shown in table 2 (online supplemental table 2). The allocation of pregnant women in the four regions of the health facilities was done proportionally based on the number of clients who visited the ANC clinic on the same month (August) of the previous year. Then the ANC clients from each selected health facility were identified systematically. To identify the interval, the total number of ANC clients was divided by the total sample size. The kth value is 2. The first woman was selected by lottery method and then every second woman visiting the health facility was selected for the study. The immediately next woman was used if the woman refuses to participate in the study. To prevent redundancy of respondents, identity mark was put on their ANC card.
Supplemental material
Percentage distribution of correct knowledge parameters of nutrition during pregnancy among pregnant women at pre-intervention, immediate post-intervention and 6 weeks later (n=215)
Inclusion and exclusion criteria
Pregnant women who were in their first and second trimester of pregnancy and willing to participate in the study were included. However, pregnant women who were sick at the time of the study and those who cannot communicate verbally were excluded from the study.
Intervention
In the context of health education programme, an educational intervention was developed by the research team based on a training module. It was then reviewed by nutrition experts from the college and Ministry of Health (MOH) for its appropriateness and adequacy. The content included introductory messages and focused on meanings of healthy diet, eating a variety of food, sources of the main food groups and micronutrients, eating well with the locally available food, hazards of maternal malnutrition, important supplements to be taken during pregnancy, harmful substances to be avoided, gestational weight gain and measures of alleviating common discomforts associated with nutrition during pregnancy. The training module on nutrition counselling for health professionals providing ANC service is annexed and is attached as a supporting material.
The training programme was carried out in the form of counselling using printed materials and flip charts for pictorial representation. Self-reading of leaflets containing the core messages for every topic prepared in the native language of the participants was also employed as the women in the study had one each. The intervention was implemented in one session taking a minimum of 20 min while pregnant women were receiving their routine ANC care. Incentives for participants in order to increase compliance or adherence were not employed. The educational intervention was given by health professionals who were given a 2-day manual-based training regarding nutrition during pregnancy and ‘GATHER’ counselling skill. The training used presentation, drills, discussions and role-play as a method. Health professionals’ knowledge and counselling skills were assessed after the training to make sure they have acquired the necessary knowledge and skills required to implement the intervention (not shown in this study).
Data collection tools and techniques
A questionnaire sheet used in this study was prepared by reviewing an Ethiopian study done on a similar topic.5 The tool was modified and finalised to fit the local context. The questionnaire had three sections. Section I dealt with the background and locating information which also included their gravidity and ANC follow-up. The knowledge questionnaire had 14 questions to assess the knowledge level of pregnant women. There were 21 open-ended and closed-ended questions that assessed the dietary practice of pregnant women including a list of food items consumed in the past 24 hours. The quantitative data which is the knowledge and practice questionnaire was administered via a face-to face interview method after the participants were informed briefly about the study and their written consents were obtained. Five professionals who have Bachelor of Science in Nursing for data collection and two clinical nurses for the purpose of supervising the data collection period were trained for 3 days on the overall research objective and methodology, data collection tools, interviewing and recording skills. Strict instructions on consistency and completeness of the tool were also given. Informed consent sheet and questionnaire are annexed and are attached as supporting materials.
Data collection procedure
Phase I of the data collection from the pregnant women (baseline assessment) using a questionnaire immediately before receiving nutrition counselling from their ANC providers took place from 31 July to 9 August. Health professionals then started providing NE to pregnant women preselected and assessed before the intervention. Immediate post-education evaluation of the pregnant women was done by the same questionnaire used to assess in the pretest. Phase II or post-intervention data collection of pregnant women was done after the client was appointed for 6 weeks after the counselling session and this took place from 12 September to 24 September. Recruitment of participants, intervention and data collection were all done in the ANC settings of the health facilities. The set-up of the ANC clinics in some of the health facilities was modified in a way that the participant of the study was to be counselled alone.
Validity
The face and content validity of the data collection instruments was ensured as the tool was reviewed by nutrition experts from the MOH, clinical nurses and advisors from the college. Considering their suggestions and recommendations, the tool was modified and finalised to fit the local context. The questionnaire was translated to Tigrigna by local language expert and then back to English by another person in order to check for consistency between the two translations.
Reliability
The data collectors were given strict guidance on how to fill the knowledge and practice questionnaires and observe the participants so as to avoid the inter-rater biases.
Study outcomes and measures
The two outcome variables in this study were the knowledge level of pregnant women on nutrition and their appropriate nutrition-related practice after intervention. Composite scores of knowledge and practice of each pregnant woman were computed. Mean scores of the knowledge (at pre-intervention, immediate post-intervention and 6 weeks later) and practice (at pre-intervention and 6 weeks later) of pregnant women were then calculated. The pregnancy-specific NE was the independent variable in this study. Covariables on ANC clients were age, gravidity, parity, gestational age, number of ANC visits, educational status of the woman and the husband, marital status, religion, occupational status, family size and income, source of information and frequency of ANC visits.
Data analysis procedures
The cleaned data were coded and entered into SPSS V.22.0. Normality of the entered data was checked with Kolmogorov-Smirnov test and Fisher’s measures of skewness and kurtosis. Descriptive analysis of the sociodemographic and other covariates was done using frequencies (percentages), mean (SD) and median (IQR) as appropriate. In order to make comparison of the overall practice scores at two time points, paired t-test was used. Comparison of knowledge scores at three time points was performed using repeated measures analysis of variance (ANOVA) followed by Bonferroni post hoc test. Factorial mixed ANOVA was used to determine effectiveness of health education on nutrition knowledge and practice during pregnancy through categories of sociodemographic variables. Finally, the results were presented using tables and graphs. A statistical significance was considered at p value of less than 0.05 except for the Box M p value of less than 0.001.
Results
A total of 230 pregnant women were approached to participate in the study according to the eligibility criteria. Four were excluded as they did not consent to be part of the study so a total of 226 were enrolled in the study and all were successfully followed to the immediate interview. Eleven women lost to follow-up and 215 completed the assessment at the 6 weeks’ time, making them the final participants for the study whose data are taken for analysis. Hence, the response rate was 95.2%. A Consolidated Standards of Reporting Trials flow chart showing subjects initially enrolled, intervened, followed up and included in the analyses in the quasi-experimental study is attached as supporting information (online supplemental material S2).
Supplemental material
Demographic characteristics of the study participants
As shown in table 3, the mean age of pregnant women was 27.71 (SD=5.10) years and the age range was 15–44 years with the larger proportion (n=72, 33.5%) of them being in the age group 25–29 years. One hundred forty-four (67%) of the pregnant women were housewives, 135 (62.8%) had an educational attainment of secondary level, 198 (92.1%) are currently married and 170 (79.1%) were Orthodox Christians. Concerning their partner’s educational status, 131 (60.9%) have completed secondary education. The study participants had a median family size of 3 and a median monthly household income of $100. When looking at their obstetric history, 74 (34.4%) were experiencing pregnancy for the first time, 86 (40%) were nullipara and 111 (51.6%) were coming for their first ANC follow-up for their current pregnancy. The median gestational age of ANC attendants was 22, with the majority (86%) of them being in their second trimester.
Effect of educational intervention on scores of knowledge regarding nutrition during pregnancy (n=215)
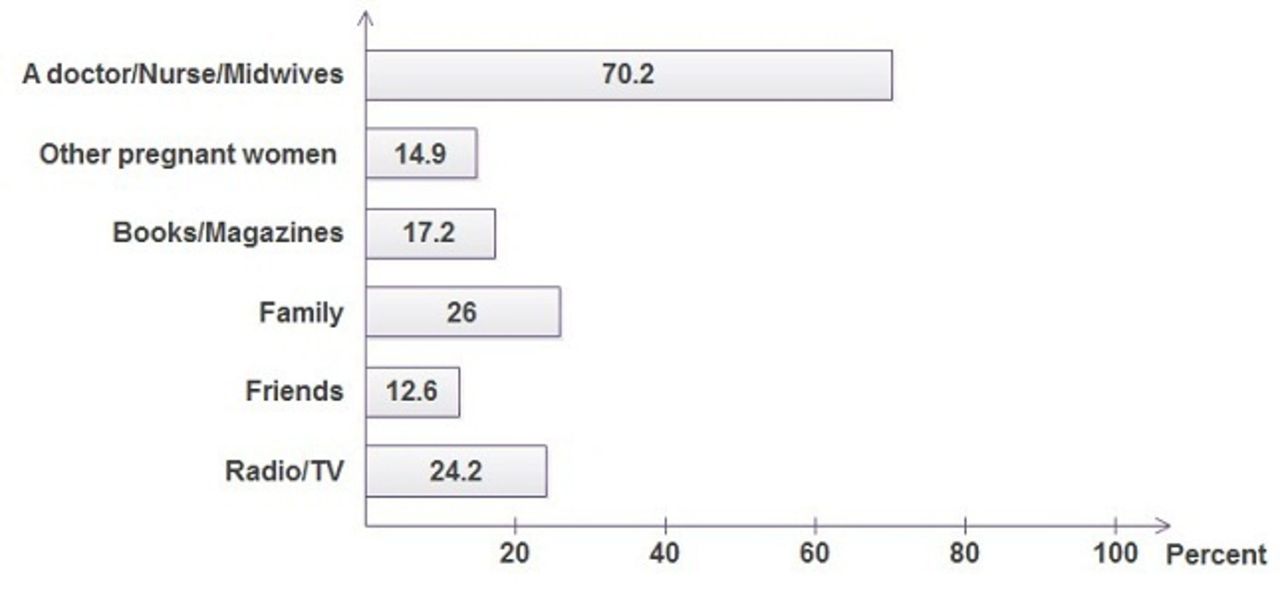
In this study as indicated in figure 1, 177 (82.3%) received nutritional counselling and for 70.2% of those who did so, a doctor, nurse and midwife were the source of information. The least mentioned source of information was friends (12.6%). From those who claimed to have received nutrition counselling, 122 (55.8%) confirmed that they got enough information from their sources to enable them to make decisions concerning their nutritional status. Less than half (n=78, 36.3%) thought the information they received was inadequate. The minority was not sure if the information they received was adequate or not.

{kind=link}
Percentage distribution for the sources of information on nutritional counselling.
Knowledge on appropriate nutrition during pregnancy among pregnant women
The result showed in table 4 illustrates the proportion of women who correctly responded to the knowledge questions regarding nutrition during pregnancy. More than three-fourths of the pregnant women (78.6%) had the perception of having to eat a variety of food throughout pregnancy, while 11.5% believed that they should avoid certain food items. Spicy food (3.3%) and meat (1.4%) were the most common food items thought to be avoided. After intervention, none of the respondents had the idea that a pregnant woman should eat only what she craves or avoid certain food items. This was still true 6 weeks later.
Pair-wise comparison of scores of knowledge of nutrition during pregnancy at pre-intervention, immediately after and 6-week follow-up (n=215)
Correct knowledge on eating an additional one meal increased from 131 (60.9%) to 212 (98.6%) in the immediate assessment, and to 213 (99.1%) 6 weeks later. The number of respondents who voted for frequent feeding during pregnancy increased from 89 (41.4%) to 215 (100%) in the immediate interview though it declined to 208 (96.7%) after 6 weeks.
Use of iodised salt during pregnancy was known by 188 (87.4%) of the participants and after intervention it was known by all. Only 86 (40%) of the study participants correctly answered the duration of iron supplementation but a higher proportion of respondents (97.7%, 94%) correctly did so at the consecutive follow-ups. Of the study participants, 207 (96.3%) and 195 (90.7%) knew maternal undernutrition would bring fetal and maternal complications, respectively. As far as the result is concerned in the immediate and 6 weeks later, it got elevated to 100% in both components. Knowledge regarding necessity of supplementation because of inadequacy of nutrients in foods increased from 184 (85.6%) at the pre-intervention time to 214 (99.5%) at the immediate post-intervention and again to 214 (99.5%) in the 6 weeks’ time. Effect of maternal undernutrition on fetal weight was correctly known by 195 (90.7%) at the pre-intervention assessment and was correctly known by all at both consecutive times.
Regarding the main food group source questions offered to the respondents, only 15.8% and 40.5% correctly listed millet and fruits as sources of carbohydrate. This was elevated to 75.3% and 64.2%, respectively, in the immediate assessment. The majority (70.7%, 95.8% and 92.6%) of the respondents correctly described legumes as a source of carbohydrate in the pre-intervention, immediate post-intervention and 6 weeks later, respectively. The same food items were described as sources of proteins by only a quarter of the respondents but after the intervention it rose to 73% and declined to 67.9% in the 6 weeks’ time. Meat and fish (82%, 96.7% and 95.8%) were the most familiar food items mentioned as sources of proteins at all times of assessment. Sunflower (17.2%), soya bean (3.7%), and maize, cereals and adri (8.4%) were the least familiar food sources of fats. Fatty meat, milk and cheese were only missed by 22.3% of the respondents as a source of fat prior to the intervention but only 3.7%, 2.3% got it wrong in the consecutive assessments. Fruits and vegetables were known by 87% and 74% of the participants as food sources of vitamins in the pre-intervention time. Their values were elevated to 99.1%, 98.6% in the immediate assessment and to 98.6%, 97.2% 6 weeks later, respectively.
Fenugreek was mentioned as a good source of iron by only 24.7% of the study participants while the other sources, meat (42.8%), fish (44.7%), egg yolk (45.6%), green vegetables (40.0%), legumes (36.3%) and fruits (28.4%) were known to a greater extent by the participants in the pre-intervention assessment. The earlier mentioned source became more popular after the educational intervention (89.8%).
Effect of educational intervention on knowledge of nutrition during pregnancy
The average knowledge scores at pre-intervention, immediate after intervention, and 6 weeks later were 29.01/47 (SE=0.35), 42.73/47 (SE=0.24) and 40.94/47 (SE=0.26), respectively, as shown in table 5. Mauchly’s sphericity result has shown that variance of the difference of scores for any two conditions is not violated (p<0.0001). Moreover, Wilk’s lambda revealed that there was significant effect for time (Wilk’s lambda=value, p<0.0001). Using the commonly used guideline of Cohen, the partial eta squared suggested that there was a very large effect size. The overall trend of the knowledge regarding nutrition during pregnancy at the three time points was quadratic.
Effectiveness of the intervention by demographic variables on knowledge (n=215)
Post hoc comparisons using Bonferroni test in table 6 indicated that the average knowledge score at pre-intervention, immediately after intervention and 6-week follow-up was significantly different. On average, the score increased by 13.72 (SE=0.30) from before the intervention to immediate after intervention. However, the score declined significantly from immediate after intervention to 6-week follow-up by 1.79 (SE=0.22). Although there was significant decrease in score from immediate after to 6-week follow-up, knowledge at 6-week follow-up was still significantly greater than that of pre-intervention (p<0.0001).
Percentage distribution of correct practice of nutrition during pregnancy among pregnant women (n=215)
Effectiveness of the intervention on knowledge by demographic variables
Factorial mixed ANOVA (table 7) was conducted to assess the impact of the educational intervention on the scores of knowledge across three time periods by age, gravidity, parity, gestational age, marital status, woman’s and husband’s educational status, occupation and number of ANC visits. There was no significant interaction between the above-listed characteristics and change in knowledge except with gravidity (Wilk’s lambda=0.957, p=0.01). The educational intervention has shown more positive impact on increasing the scores regarding knowledge of appropriate nutrition during pregnancy for primigravida mothers than for the multigravida mothers.
Reasons reported for avoiding certain food items (n=215)
Practice of appropriate nutrition during pregnancy among pregnant women
Higher proportion of pregnant women changed their practice of pregnancy-related diet in adding an extra meal (from 69.3% to 97.2%), eating two servings of green leafy vegetables (from 56.7% to 81.4%) at 6 weeks later as compared with the pre-intervention time (table 8). The majority were in line with consuming two to three servings of meat, fish, nuts or legumes per day at the pre-intervention (64.2%) and 6 weeks later (80.9%) assessments, respectively. Similarly, the proportion of pregnant women eating two to three servings of dairy (milk, eggs, yoghurt and cheese) per day at pre-intervention and 6 weeks’ time assessment were 58.1% and 86%, respectively. Almost all (98.1%) reported using iodised salt for cooking in their current pregnancy, this figure later increased to 100% 6 weeks later.
Effect of educational intervention on appropriate practice of nutrition during pregnancy (n=215)
When pregnant women were asked about the food items they consumed in the last 24 hours, more than half (66.5%) of them had bread in their breakfast and for 76.3% of them, injera (injera is a sour flatbread used in Ethiopian and Eritrean cuisine that is thicker than a crepe but thinner than a pancake and has a delightfully sour taste) was included in their diet. Less than half (32.6%) had meat for lunch.
The majority (87.4%) of pregnant women started eating four times and above after the education. A slight increase was observed in the practice of serving meals alone due to intervention (from 18.1% to 22.3%), the rest were still sharing their plate with their family members. Fifty-seven (26.5%) pregnant women were skipping meals but after intervention the number decreased to 2.3%. Dinner was the commonly skipped meal at both pre-intervention and 6 weeks later (12.6% vs 1.4%).
The adherence of pregnant women to iron supplement tablets decreased from 86.5% at pre-intervention to 84.7% after the intervention. Reasons as per their response for not adhering to iron supplements were poor supply (31.8%), side effects (36.4%) and inability to remember (31.8%). None of the participants were smokers, 204 (94.9%) reported avoiding alcohol and 153 (71.2%) decreased their coffee consumption during their current pregnancy. Even more (n=202, 94%) decreased their coffee consumption after the intervention.
Fifty-eight (27%) participants have avoided one or more food types in their current pregnancy but after intervention only 15 (7%) had the same practice. The most frequently avoided foods were meat (14% vs 1.9%), grains (6% vs 2.3%), dairy products (7.4% vs 0.9%), spicy foods (4.2% vs 1.9%), vegetables (1.9% vs 0%), fruits (1.9 vs 0.5%) and eggs (0.5 vs 0%). The provided reasons for avoiding food items are listed in table 9. Personal dislike associated with nausea and vomiting during pregnancy was the most common reason that forbade women from consuming certain food items (25.1%). People telling them that the food may cause fetal abnormality or fatty baby with consequent difficulty during delivery were other reasons reported by similar number of respondents (1.9%). During the post-education assessment, the sole reason for avoiding food was personal aversion (7%).
Effectiveness of the intervention by demographic variables on practice (n=215)
Effect of educational intervention on appropriate practice of nutrition during pregnancy
As indicated in table 10, the practice score at 6-week follow-up (M=13.13 out of 16, SE=0.09) was significantly higher than that of pre-intervention (M=12.55 out of 16, SE=0.16). The average difference of score was 0.58 (95% CI: 0.29 to 0.87).
Effect of Educational intervention on appropriate practice of nutrition during pregnancy (n=215)
Effectiveness of the intervention on appropriate dietary practice during pregnancy by demographic variables
Factorial mixed ANOVA (table 11) was conducted to assess the impact of the educational intervention on the scores of practice across two time periods by age, gravidity, parity, gestational age, marital status, woman’s and husband’s educational status, occupation and number of ANC visits. There was no significant interaction between the categories of demographic characteristics listed above and change in practice.
Effectiveness of the intervention by demographic variables on practice (n=215).
Discussion
Basically, the purpose of health education is to eliminate undesirable behaviours and replace them with appropriate and productive behaviour leading to healthy life. This study sought to answer the question of whether training given to pregnant women had an effect on bringing a positive change in their knowledge and appropriate dietary practice.
The knowledge score of pregnant women in this study significantly increased from 29.01/47 at pre-intervention to 42.73/47 in the immediate after intervention which later decreased to 40.94/47 6 weeks later. This was comparable with a similar Ethiopian study as the proportion of pregnant women with good knowledge of nutrition during pregnancy increased from 53.9% to 97%.5 Similar quasi-experimental Iranian study also revealed that the awareness level of pregnant women about healthy nutrition significantly increased from 3% before intervention to 31% after the nutritional education intervention,.2 It also agrees with a study done in India which found an overall nutritional knowledge improvement from a mean of 22 in the pre-test to 32.7 at post-test.17 These similarities show the effectiveness of NE in improving knowledge of pregnant women. In addition to that, the GATHER counselling skills incorporated in the training given to health professionals might have helped improve the communication between the professionals and their pregnant patients thereby significantly increasing the percentage of women who had an ample opportunity to discuss healthy eating at their ANC visits. The change in the level of knowledge in this study did not show any significant interaction with the sociodemographic characteristics except with gravidity, the same was true in an Iranian study where the change was independent of age or literacy levels.2 This result is a sign that there was a gap in knowledge across most categories of background characteristics. This fact makes preparing a one and only teaching module easier as the prepared module can be equally effective for pregnant women of various background characteristics.
Assessing the preferred source of information among pregnant women was necessary as it helps in devising recommendations. In this study, 70.2% of the pregnant women turned to a doctor/nurse/midwife for information. This was similar to other studies such as an Australian study where 67.4% of the NE was provided by midwives.18 In another Knowledge, Attitude and Practice Survey, the main sources of information were doctors.19 These results were unlike other studies such as a recent Ethiopian study where the result was not in favour of health professionals as the best source of information.5 The same was also evidenced in a Polish study where half of the pregnant women mentioned own experience as source of information.20
This study documented a 64.8% of pregnant women who knew maternal undernutrition would bring fetal complications. This result was higher than East Wollega’s result where 34.8% of respondents had the same idea.1 A cross-sectional study in India found an even lower proportion of mothers (27.4%) with this knowledge. The pregnant women in this study who were living in an urban area had a better access to information and lesser wrong cultural influences. This difference in the study setting could be the reason for the discrepancy in the results. However, this result was lower than the Ethiopian study in which 82.5% of pregnant women knew about fetal complications of undernutrition.5 This difference could be an impact of the differences in the cultural and spiritual influences of the areas.
In this study, 90.7% of the study participants were fully aware of the effect of maternal undernutrition on fetal weight. This was similar to an Ethiopian study where a major proportion (82.8%) knew that maternal undernutrition results in LBW and stillbirth.5 It also agreed with the Lagos State study where the majority (66.8%) of the respondents agreed that inadequate and inappropriate nutrition can determine body weight of the baby.9
In this study, 60.9% of the pregnant women were familiar with the fact that pregnant women need to eat more than their non-pregnant state. This was more or less comparable with an Ethiopian study where the result was 270 (66.5%).5 Both these results were lower than Pakistani mothers who did believe so (84%). Moreover, in another study as many as 70% of the respondents had the knowledge that they should eat differently from non-pregnant women.19 In addition to that, in a study in Shashemene district, Ethiopia, more than three-fourths (82.4%) believed in the importance of eating balanced diet during pregnancy.13 This was discordant with that of University of Yaoundé’s result where the majority (52%) of the study respondents thought that a mother should eat according to her appetite.3
In this study, more than half of pregnant women were knowledgeable about many food sources of iron. This was higher than the 31.8% pregnant women in an Ethiopian study with adequate knowledge on food source of iron,5 but it was in consonant with an Indian study where 61.3% of the pregnant women had a satisfactory knowledge on food source of iron.17 In a 2012 study by Mohannad et al, the overall knowledge regarding iron-rich foods was also low.19 Contrary to these comparative study’s finding was reported in a Tanzanian study where 94.8% of the study population had moderate knowledge regarding sources of iron-rich foods.21 This study has also shown that necessity of supplementation because of inadequacy of nutrients in foods was correctly addressed by 85.6% of pregnant women. A similar study demonstrated a lower proportion of mothers (67.7%) with the same understanding regarding supplementation during pregnancy.5 This study also shows that only 40% of the study participants correctly answered the duration of iron supplementation though their proportion due to intervention increased to 97.7%. The same effect was seen in a study conducted on the same topic which was 35.5% prior to intervention and later increased to 92.1%.
The mean overall scores of practice of pregnant women were found to be 12.55/16 (78.44/100) and 13.13/16 (82.06/100) in the pre-intervention and 6 weeks’ later assessment, respectively. This score was higher than is obtained in an Ethiopian study where the score was 6.2/11 (56.36/100).5 The high practice score in this study is an expected response to their higher level of knowledge. Another possible reason could be that the 6- week assessment was done post a major Christian holiday (Geez New Year) where a variety of food items are served. Regardless of the quantity of change, an interventional study also showed a significant increase in quality and quantity of the diets consumed.17 A significant increase in the amount of almost all the food groups consumed in the post-NE as compared with non-NE and pre-NE group was also evidenced in a Dutch study. An Egyptian study in 2006 also pointed that the target women increased their consumption of foods and avoided secondhand smoke.22 A high proportion of pregnant women with good practice was also seen in Pakistan (65.5%). A study in Swaziland found a closer proportion with 51% good practice among pregnant women. In contrary to these findings in a study of University of Yaoundé, more than half (58%) of pregnant women ate according to their appetites which was according to their belief.3
In this study, 69.3% of the pregnant women have added at least one additional meal from non-pregnant diet, this was in accordance with an Ethiopian’s study result of 69.7%.5 Moreover, it was similar to an Indian study where there was a significant increase in the amount of almost all the food groups consumed in the post-NE as compared with non-NE and pre-NE group.17 This was the opposite of a study done in Wondo Genet where 75.2% of the pregnant women did not take any additional meal during pregnancy. A possible explanation for this result was involvement of women with a larger household size who had to share the food among them in the study.23 Similarly in a study in Shashemene district, Ethiopia, only 33.2% made changes to their normal eating habit.13 In the same study, more than one-third (38.3%) of pregnant women practise fasting during pregnancy, in this study only one respondent reported fasting. The difference in the knowledge regarding the concepts as well as disparities in the economic level of the communities could have hugely influenced the outcome of the studies.
In a southern Ethiopian study, the habit of skipping meals was observed to a higher extent than was evidenced in this study. About 43.8% commonly skipped lunch and 24.2% reported that they skipped breakfast.23 In this study, the most commonly skipped meal was dinner. A probable reason for this is that in the comparable study the proportion of respondents with a large family size and in their earlier gestation with associated nausea and vomiting which could have made consuming food early in the morning difficult was high.
In general, 58.1% were in line with consuming two to three servings of dairy per day, 56.7% were in line with consuming two servings of green vegetables; one serving of a yellow vegetable per day. This was a bit higher than an Ethiopian study’s result where 42.4% were in line with dairy products, and 46.1% in line with green vegetable servings,5 but similar to a study in the USA where 42.7% and 58.9% of respondents had a habit of daily drinking of milk and eating fresh vegetables, respectively. In an Indian study, most (90%) reported consuming green leafy vegetables and fruits only once or twice a week due to economic constraints.17 In addition to that, more than three-fourths (76.5%) of study participants reported to consume cereal-based crops and about three-fourths (74.5%) reported consuming legumes in the preceding 24 hours in a study at Wondo Genet district.23 It is obvious that diet of different communities is not the same and so one cannot expect pregnant women to consume similar items in similar proportion.
The proportion of women who correctly started to practise serving meals, which is serving alone slightly increased from 18.1% in the pre-intervention time to 22.3% post-education. This lack of big difference may be due to the fact that nutrition knowledge alone may not be sufficient to initiate behavioural application of healthy diets. More importantly, the highly socialised culture of the country where you get to be served with all your family members cannot be just undone.
The adherence to iron supplements before the intervention in this study was 86.5%. This in comparison was higher than Zelalem et al’s (2017) result which was 69%, a study in North Western Zone of Tigray (37.2%), America (63.7%), Italy (45.3%), India (62%) and Pakistan (56%). It is true that the adherence of pregnant women towards iron supplements decreased after intervention. A probable reason for this is that the pregnant women coming for their first ANC visit, though had not started taking the iron supplement, were considered as having the correct practice. When they were started on the supplements, the probability of them to not adhere to the supplements started to appear for various reasons. The most commonly reported reason for not using iron supplements in the above studies was their side effects and perception that supplements have no benefits. In this study, the commonly reported reasons were gastrointestinal side effects, forgetfulness and poor access to the supplement. Other reasons not reported in this study, which is of course reassuring, include unappealing taste, fear of difficult delivery and surprisingly in an Indian study respondents believed that supplements cause miscarriage and may cause their children to have a dark complexion; and because dark complexions are considered undesirable, some women discontinue the use of the supplement. The intervention strategy, free supplementation and health providers with adequate knowledge regarding the supplements being the primary source of information could be the cause for higher percentage of pregnant women with correct practice.
Fifty-eight participants have avoided one or more food types in their current pregnancy in this study but after intervention only 15 had the same practice. In an Ethiopian study, 27.3% were avoiding certain food types and this decreased to 16.5% after intervention.5 A study in Shashamane found that half (49.8%) of the pregnant women in the area were avoiding one or more foods.13 About 20.9% of the pregnant mothers in Wondo Genet also restricted their food intake. This was also noted among 16% of Nigerian pregnant women. The disagreement in the results clearly indicates that feeding practices differ from culture to culture and society to society. Not only that, but food habits are also mainly determined by the availability of indigenous food supply, sociocultural and educational orientation of food processing and preparation methods, and the difference of these characteristics in the study participants could have had a hand in bringing difference in the results.
In this study, personal dislike associated with nausea and vomiting during pregnancy was the most common reason that forbade women from consuming certain food items. People telling them that the food may cause fetal abnormality or fatty baby with consequent difficulty during delivery was reported by similar number of respondents (1.9%). Higher proportion (9.9%) restricted their food intake in Akaki city in Ethiopia for the latter-mentioned reason.5 Cultural values and food taboos due to health, cultural or spiritual reasons exempted mothers from eating meat in a University of Yaoundé’s study.3 The same reason was also reported in a Shashamane study.13 A lower proportion in this area as compared with the other studies could be due to difference in beliefs and educational level of women.
From the above, it would appear that pregnancy is an influential ‘teachable moment’ to promote healthy nutrition. It is true that some results of this study did not align with other comparable studies’ results and the researchers to their best have tried to explain these discrepancies by highlighting the differences in the culture, beliefs and background characteristics of the study respondents. Differences in gravity of food cravings and aversions were possibly in response to beliefs about what should be consumed alongside physiological changes in pregnancy; thus, requiring dietary counselling and support to be started early in pregnancy.
It is also evident that all nutritional advice is not followed. This may be due to lack of interest in making a change in one’s diet, or certain perceived or encountered barriers that may prevent people from eating healthier diets such as the lack of money (cost), lack of time (too busy with work) or taste. Further research may then be required to address these issues.
However, even these findings are grounded on a relatively weak evidence base that is characterised by studies with design or analysis limitation. Additional well-designed research is needed to quantify the capacity for and cost-effectiveness of NE provided during pregnancy that targets improved nutrition of the pregnant mother to improve maternal, neonatal and child health outcomes and inform the development of best practices. Those better researches could also determine the additional benefit and cost-effectiveness of adding nutritional support, for example, food or micronutrient supplements.
The following limitations need to be considered while interpreting the findings of the study. The possible effect of other sources like TV, books, magazines and radio broadcasting on the change in the knowledge and practice of pregnant women towards nutrition could not be controlled. Face-to-face interview may lead to social desirability bias which may in turn bring higher proportion of correct practice among pregnant women on the follow-up questioning (as the practice is self-reported). Having said that, there could have been better ways of confirming whether pregnant women were using iodised salt or not such as doing a dye test. The self-reporting mechanism of responding also led to recall bias which could have led to information bias.
Conclusion
This study has shown that the current intervention generally was effective in accomplishing improved knowledge and practice level of pregnant women. The simple NE messages given to pregnant women using holistic approach of targeting all the major determinants in a sustained manner played a huge role in increasing their knowledge regarding nutrition during pregnancy. Knowledge regarding duration of iron supplementation was very low in this study. At the same time, minor knowledge gap was seen in the sources of main food groups among pregnant women. The provided NE also helped the pregnant women to improve dietary intake during pregnancy, although their adherence to iron supplements was decreased. Skipping meals and avoiding certain food items were also evident in this study. A reassuring concept is that food taboos and cultural factors were never the reasons that prevented women from consuming the food items. The educational intervention has shown more positive impact on increasing the scores regarding knowledge of appropriate nutrition during pregnancy for primigravida mothers than for multigravida mothers, while the improvement in the dietary practice had no interaction with their sociodemographic characteristics. To sum up, attenuation of maternal and infant malnutrition may not be remote if pregnant women are well educated and counselled about nutrition during pregnancy.
Supplemental material
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
Ethical clearance and support letter for the study were obtained from the ethical and scientific committee of Asmara College of Health Sciences, then the researchers visited the head of the branch of MOH of Zoba Maekel for further permission. Moreover, the head nurses and medical directors of each study site were approached with full explanation of the general purpose and nature of the study. Informed written and signed consent was taken from the participants after the purpose of the study was thoroughly explained to them beforehand. Above all, the participants’ information was handled with great confidentiality. Pregnant women were also informed that their participation was voluntary and that they could withdraw from the study at any time during the research.
Acknowledgments
The authors would like to thank the participants who took part in this study, the National Board of Higher Education (NBHE) for funding the research and for all who contributed one way or another to the successful completion of the project.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LGT designed the study, coordinated recruitment of participants and education of participants, prepared teaching materials, and wrote all drafts and the final manuscript. SAB designed the study, coordinated recruitment of participants and education of participants, and participated in writing the manuscript. HGA coordinated recruitment of participants and education of participants, and wrote all drafts and the final manuscript. GG assured quality of data collection, and wrote all drafts and the final manuscript. ZT coordinated recruitment of participants, designed the study, modified the questionnaire, coordinated education of participants, and wrote all drafts and the final manuscript. EH assured quality of data collection, led data analysis, wrote the manuscript, and wrote all drafts and the final manuscript. All authors read and approved the final manuscript.
Funding This research was supported by the National Board of Higher Education. The award grant number is 25/08/18.
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed by Dr Emmanuel Baah, University of North Carolina System.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.