Article Text

Abstract
Objective To evaluate the association between pasta meal intake and long-term risk of developing diabetes or atherosclerotic cardiovascular disease (ASCVD, including coronary heart disease (CHD) and stroke) in postmenopausal women.
Design Prospective cohort study.
Setting Women’s Health Initiative (WHI) in the USA.
Participants 84 555 postmenopausal women aged 50–79 in 1994, who were free of diabetes, ASCVD and cancer at baseline who were not in the dietary modification trial of the WHI, completed a validated food frequency questionnaire, and were evaluated for incident diabetes and ASCVD outcomes during the follow-up until 2010.
Main outcome measure Diabetes and ASCVD.
Results Cox proportional hazards models were used to estimate the association (HR) between quartiles of pasta meal consumption (residuals after adjusting for total energy) and the risk of incidence diabetes, CHD, stroke or ASCVD, accounting for potential confounding factors, with testing for linear trend. We then statistically evaluated the effect of substituting white bread or fried potato for pasta meal on disease risk. When comparing the highest to the lowest quartiles of residual pasta meal intake, we observed significantly reduced risk of ASCVD (HR=0.89, 95% CI 0.83 to 0.96, p trend=0.002), stroke (HR=0.84, 95% CI 0.75 to 0.93, p trend=0.001), CHD (HR=0.91, 95% CI 0.83 to 1.00, p trend=0.058) and no significant alteration in diabetes risk (HR=1.02, 95% CI 0.96 to 1.07, p trend=0.328). Replacing white bread or fried potato with pasta meal was statistically associated with decreased risk of stroke and ASCVD.
Conclusions Pasta meal intake did not have adverse effects on long-term diabetes risk and may be associated with significant reduced risk of stroke and ASCVD. The potential benefit of substituting pasta meal for other commonly consumed starchy foods on cardiometabolic outcomes warrants further investigation in additional high-quality and large prospective studies of diverse populations.
- diabetes mellitus
- nutrition assessment
Data availability statement
Data will make avaviable subject to distrubtion policiy of the Women's Health Initiative (WHI) research program and the National Institute of Health (NIH).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What this paper adds
The present study has found that higher pasta meal intake may be significantly associated with reduced long-term risk of stroke and atherosclerotic cardiovascular disease in postmenopausal women.
Substituting pasta for an equal amount of fried potato or white bread could potentially be associated with lower risk of stroke and atherosclerotic cardiovascular disease.
Introduction
Among major sources of dietary carbohydrates, pasta has long been a staple food in diverse human cultures around the world. Interest in the health effects of pasta on the human body has steadily increased since the 1980s during a series of clinical studies of patients with diabetes showing that blood glucose response was remarkably reduced after ingesting spaghetti compared with white bread,1–4 potato2–5 or rice.5 Many characteristics of pasta have been studied in relation to its glycaemic response. Notably, the structure (ie, viscosity, particle size and shape) of pasta appears to be more important in determining its glycaemic response than the types of cereal used in its production.6–8 It has also been found that consumption of pasta meal produced a lower postprandial insulin response than consumption of white bread in healthy subjects.6 Given the same amount, pasta appears to have lower glycaemic index (GI) as well as glycaemic load (GL) compared with other major sources of carbohydrates.4
The International Carbohydrate Quality Consortium reached consensus in 2015 that there was convincing evidence that low GI/GL diets reduce the risk of type 2 diabetes and coronary heart disease (CHD), and GI represents another characteristic of carbohydrate foods apart from fibre and whole grain content.9 Dietary GL and GI have been linked to numerous cardiometabolic conditions10–14 and risk factors.15–18 Low-GI foods have been consistently associated with better glucose control in patients with diabetes.19 Since pasta has been shown to produce lower glycaemic response, it is then natural to hypothesise that consumption of pasta meal may have beneficial effects on the long-term risk of diabetes and atherosclerotic cardiovascular diseases (ASCVD, including CHD and stroke), given the same total carbohydrate consumption. However, few long-term studies have prospectively and directly investigated long-term average intake of pasta and the risk of developing diabetes, CHD, stroke and ASCVD. In the current study, we also aim to evaluate whether substituting other types of carbohydrate-dense food with pasta was associated with altered risk. To our knowledge, no other large-scale, long-term prospective cohort studies have specifically evaluated these relationships.
Methods
Study population
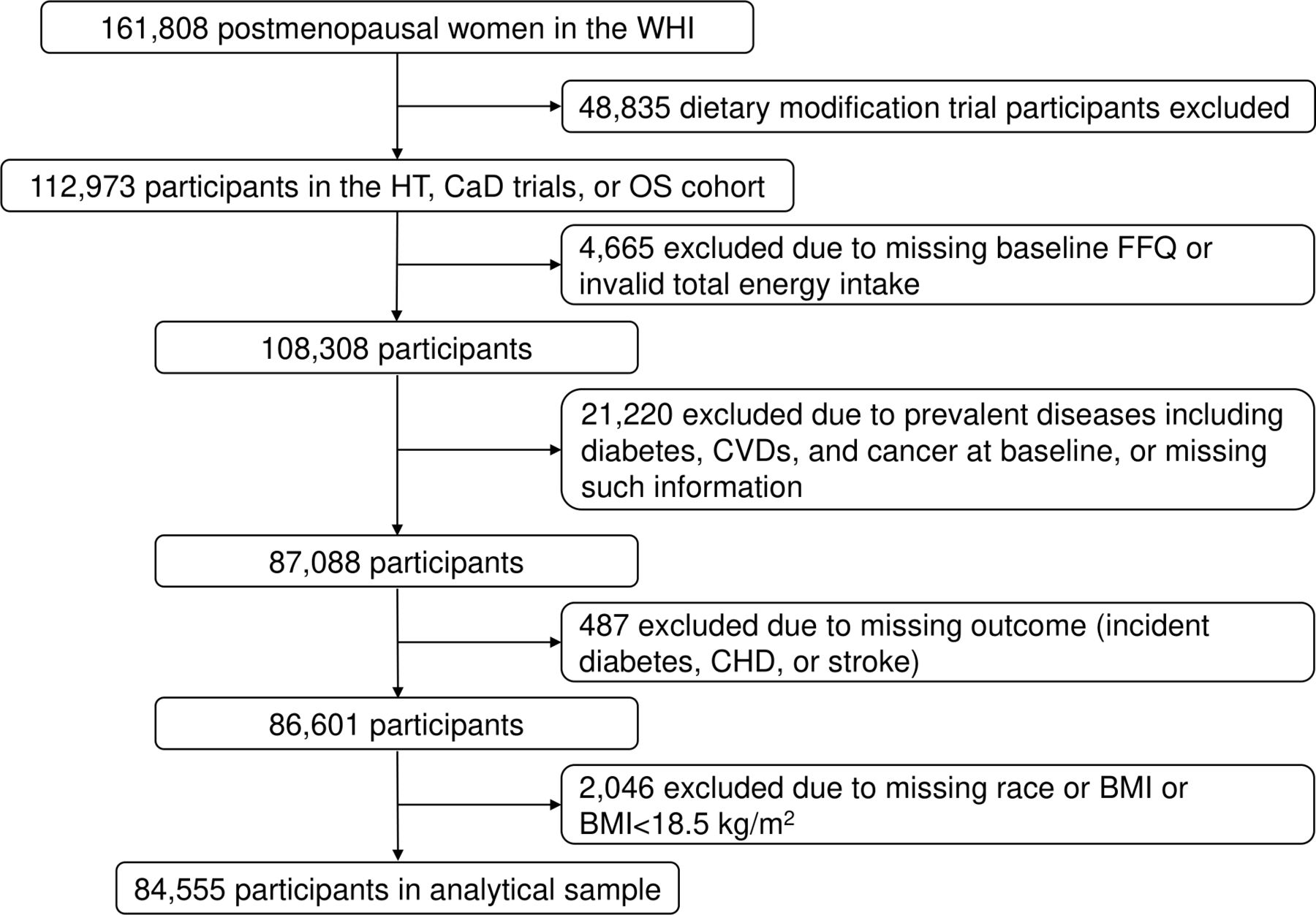
The Women’s Health Initiative (WHI) recruited a total of 161 808 postmenopausal women aged 50–79 years at 40 clinical centres across the USA between 1993 and 1998, including a cohort of 93 676 women in a prospective observational study (OS) and 68 132 women in one or more of the following three clinical trials (CTs): the hormone therapy (HT) trial, the calcium and vitamin D (CaD) trial and the dietary modification (DM) trial. We analysed baseline data from participants of the OS, and the HT and CaD trials of the WHI, for whom valid information was obtained from a validated 122-item food frequency questionnaire (FFQ).20 Participants of the DM trial were excluded due to potential major alterations in dietary behaviour after baseline. Additional exclusion criteria included: implausible total energy intake (<600 or >5000 kcal/day); prevalent diseases including diabetes, cardiovascular disease (CVD) and cancer that may alter dietary behaviours; measurements not available for outcomes of interest (incident diabetes, CHD or stroke); measurements not available for important covariates such as race and body mass index (BMI); and being underweight (BMI <18.5 kg/m2) which may reflect underlying medical conditions (figure 1).
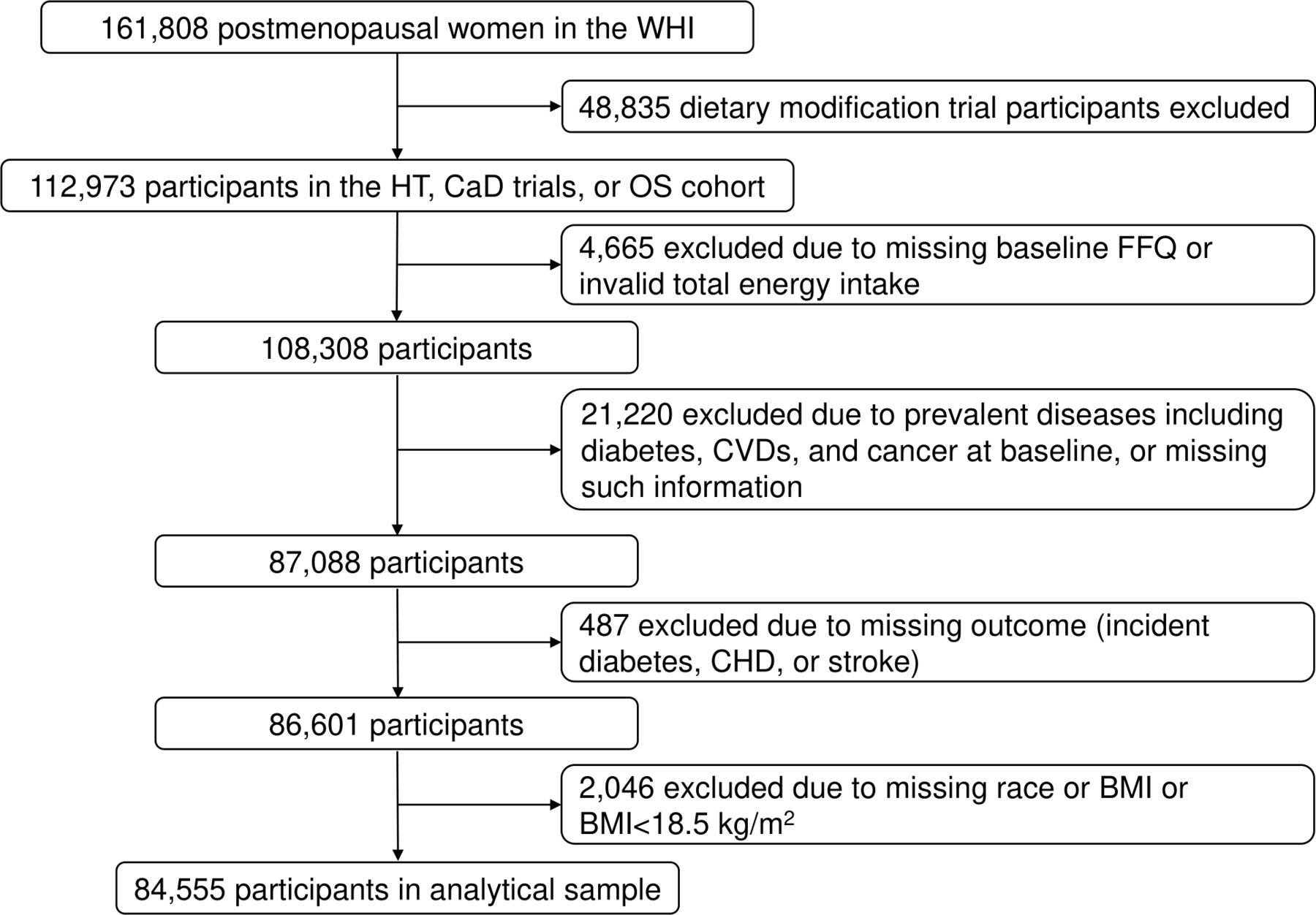
Analytical sample flow chart. BMI, body mass index; CaD, calcium and vitamin D; CHD, coronary heart disease; CVD, cardiovascular disease; FFQ, food frequency questionnaire; HT, hormone therapy; OS, observational study; WHI, Women’s Health Initiative.
Measurement of outcomes
Incident diabetes was assessed via questionnaires at enrolment and each annual visit. Participants were asked if ‘a doctor prescribed for the first time any of the following pills or treatments: pills for diabetes or insulin shots for diabetes’ since their last medical update. Those who responded ‘yes’ were considered having been diagnosed with diabetes. Since these were all postmenopausal women, newly diagnosed diabetes cases were most likely type 2 diabetes cases, which have been shown to have a high validity.21 22 Women who self-reported diabetes at baseline were excluded from the current analysis.
Incident CHD was defined as the first occurrence of clinical myocardial infarction (MI), definite silent MI, or a death due to definite or possible CHD. Clinical MI and death were adjudicated for CT and OS participants during the core WHI study (until 2005) and Extension Study I (Ext1, until 2010).
Incident stroke was defined as the first occurrence of stroke or death due to cerebrovascular event. Stroke was adjudicated for CT and OS participants through Ext1. We further examined the concept of incident ASCVD as an outcome, which encompassed incident cases of CHD and stroke as defined above, according to the 2013 American College of Cardiology/American Heart Association Guideline on the Assessment of Cardiovascular Risk.23
Measurement of pasta meal
Using a validated semiquantitative FFQ,20 24 participants reported on the baseline FFQ how often they consumed each of the following forms of pasta during the past 3 months: macaroni and cheese/lasagna/noodles with a cream sauce, spaghetti or other noodles with meat sauce and spaghetti or other noodles with tomato sauce (and no meat), in frequency of medium servings (one cup). Nine frequency options were given, including: ‘never or less than 1 per month’, ‘1 per month’, ‘2–3 per month’, ‘1 per week’, ‘2 per week’, ‘3–4 per week’, ‘5–6 per week’, ‘1 per day’ and ‘2+ per day’. Participants also had the choices of ‘small’, ‘medium’ and ‘large’ for portion size per serving. The midpoint of the nine categories was used to compute the semicontinuous variables for these three forms of pasta meals, in number of medium servings per day. The sum of the three was used as a measure of total pasta meal intake. The residual method was then used where total pasta meal intake was first regressed on total energy intake, and the residuals added with mean total pasta meal intake were taken as a measure of pasta meal intake uncorrelated with total energy intake.25
In addition to residual total pasta meal intake, we also constructed two measures of pasta meal intake analogous to energy density standardisation: (1) the ratio of pasta to dietary GL was computed by dividing total pasta meal intake with total dietary GL and then multiplied by 100; (2) the ratio of pasta to total energy intake was computed by dividing total pasta meal intake with dietary total energy intake and then multiplied by 1000. The respective scaling was done to obtain physiologically interpretable measurements. These two ratio measures were analysed in multivariable models in parallel with residual total pasta meal intake.
Statistical analysis
Baseline characteristics of participants included in the current analysis were described according to quartiles of residual total pasta meal intake. Means and SDs were generated as descriptive statistics for continuous variables, while frequencies and percentages were generated for categorical variables. Differences across pasta meal intake quartiles were tested by analysis of variance for continuous variables and by χ2 test for categorical variables.
Cox proportional hazards models were used to evaluate the association between residual total pasta meal intake and the risk of diabetes, CHD, stroke and ASCVD in terms of HRs and associated 95% CIs, with study baseline as the origin of analysis and time to event or time to censoring as defined hereafter. For each disease condition of interest (diabetes/CHD/stroke/ASCVD), follow-up durations were calculated as the interval between baseline and the earliest of any of the following: (1) date of annual medical history update when new disease was reported, (2) date of last data collection from the main study if the participant did not enter the Extension Study, (3) date of last data collection from the Extension Study, or (4) date of reported death.
Residual pasta meal intake was analysed both in quartiles and as continuous variables. We also tested for linear trend after assigning the median of each quartile to the participants. The proportional hazards assumption was tested following standard procedures.26 We adjusted for the following potential confounding factors in model 1: study group indicator (OS/HT/CaD), age (continuous), race/ethnicity (Caucasian, African-American, Hispanic, Asian/Pacific Islander or other) and region (Northeast, South, Midwest or West of the US). In model 2, we additionally adjusted for BMI (continuous, computed from weight and height measured by trained study staff), total energy intake and per cent energy intake from carbohydrates. In model 3 and the final model, we further adjusted for cigarette smoking (never, past or current), alcohol consumption (continuous), physical activity (in metabolic equivalent hours/week, continuous), and Healthy Eating Index (HEI 2005,27 continuous), and the respective family history of each outcome (diabetes, CHD, stroke or ASCVD). These potential confounding factors were chosen a priori based on current understanding of scientific literature and whether they could influence our exposure and outcomes of interest. Pasta to GL ratio and pasta to total energy ratio were analysed in similar procedures as the residual total pasta meal intake, in both continuous form and quartiles, and then tested for linear trend. We also evaluated the results adjusting for potential dietary confounders, including daily intake of fibre, total sugar, added sugar, non-whole grain, whole grain, frequency of eating a serving of vegetables and other major components in typical pasta meals (intake of total cheese and total tomato in medium servings per day).
As a sensitivity analysis, we included only pasta meals with spaghetti as the main carbohydrates source, as macaroni and cheese had been observed to have higher GI,7 analysed similarly to residual total pasta meal intake. In a second sensitivity analysis, we used age as the timescale in the Cox proportional hazards model instead of time to event. We also statistically tested for the substitutional effects of replacing pasta meal for the same amount of white bread or fried potato, measured with the same FFQ. To model such effects, if we take white bread as example, first the residual variable for white bread was created using the residual method; then residual total pasta meal intake and the sum of residual pasta and residual white bread were both included in model 3, so that the effect estimates for the residual pasta variable represented the estimated log(HR) for replacing one medium serving of white bread or fried potato by pasta, respectively, since the interpretation of the effect of the residual pasta variable was conditional on holding other covariates constant.28 All statistical analyses were conducted using R V.3.6.3.29
Results
A total of 84 555 participants of the WHI-OS, HT and CaD were included in the final analytical sample. Among these women, the median intake of pasta meal was 0.15 servings per day, or equivalently 1.04 servings per week, with the IQR from 0.08 to 0.26 servings per day (equivalently 0.54–1.84 servings per week). This group of participants were on average 63.3 years old (SD=7.3), had an average BMI of 27.3 kg/m2 (SD=5.6), an average total energy intake of 1576.2 kcal/day (SD=598.8) and an average total carbohydrates intake of 203.7 g/day (SD=78.0), which translated into an average of 52.4% energy from carbohydrates (SD=9.6). Eighty-five per cent of them were white and 6.8% were smokers at study baseline. Thirty per cent had a family history of diabetes, while 51.8% had a family history of CHD, 36.1% had a family of history of stroke and 65.2% had a family history of ASCVD.
Those in the higher quartiles of residual total pasta meal intake were on average younger, more likely to be white, less likely to be never smokers and more likely to have family history of diabetes and CHD, but not stroke or ASCVD. In terms of dietary intakes, women in the lowest and highest quartiles of residual pasta meal intake had on average higher total energy intake and GL, and higher intake of total carbohydrates, total sugar, added sugar intake, fibre and both whole and non-whole grains. Those in the lowest quartiles of residual total pasta meal intake had relatively higher alcohol intake, but lower per cent energy from carbohydrates and dietary quality as measured by HEI 2005. Physical activity levels and GI were relatively similar in magnitude across quartiles (table 1).
Baseline characteristics of WHI participants in analytical sample by quartiles of energy-adjusted total pasta meal intake (n=84 555)
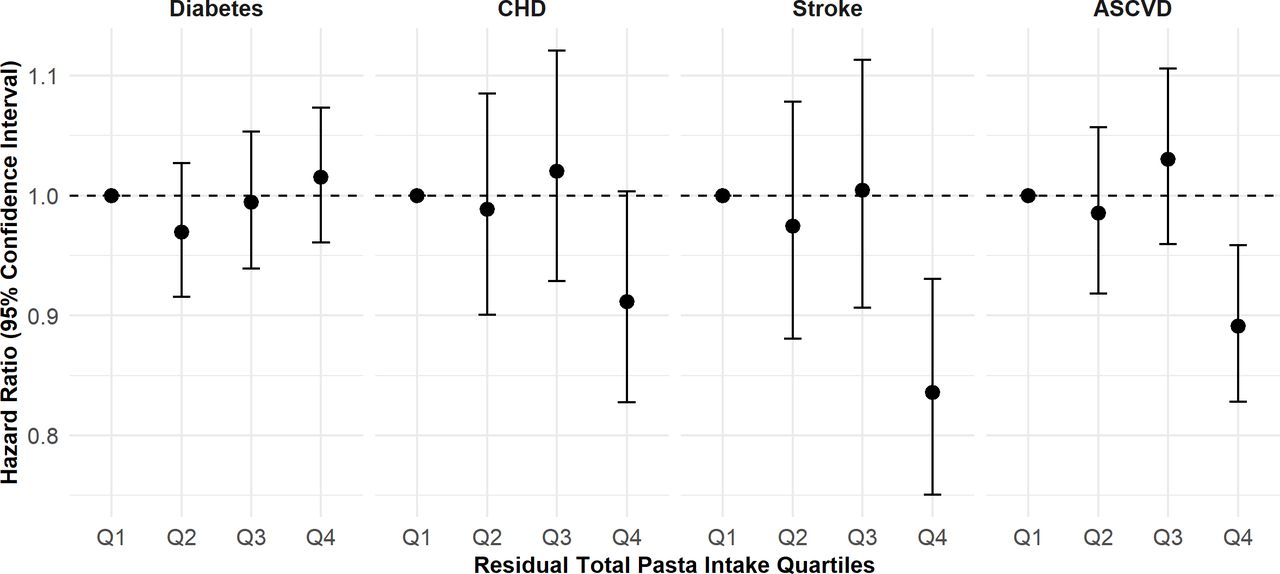
Results from the Cox proportional hazards models were summarised as follows by outcomes of interest. Residual total pasta meal intake across quartiles was not associated with risk of diabetes for postmenopausal women, after adjusting for age, race, region, study indicators, BMI, total energy intake, per cent energy from carbohydrates, smoking status, alcohol consumption, physical activity, HEI 2005 and family history of diabetes (model 3). Models 1–3 had similar results (table 2). Specifically, from model 3 (figure 2), compared with those in the lowest quartile of residual pasta meal intake, women in the second, third and highest intake quartiles had essentially no change in risk for incident diabetes (HR=0.97, 95% CI 0.92 to 1.03; HR=1.00, 95% CI 0.94 to 1.05; HR=1.02, 95% CI 0.96 to 1.07, respectively), and the linear trend was also not significant (p value for trend=0.328). Results were largely similar when examining quartiles of pasta to GL ratio or pasta to energy ratio.

{kind=link}
{kind=link}
Estimates of relative risk and 95% CIs of outcomes of interest according to quartiles of pasta meal intake from model 3 (adjusted for age, race, region, study indicators, body mass index (BMI), total energy intake, per cent energy from carbohydrates, smoking status, alcohol consumption, physical activity, Healthy Eating Index (HEI) 2005 and family history of the respective disease outcome). ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease.
Estimates of relative risk and 95% CIs of diabetes according to quartiles of pasta meal intake
For the CHD outcome, overall increased intake of pasta meal appeared to be associated with a decreased risk of developing CHD, especially when comparing women in the highest against the lowest quartile of residual total pasta meal intake (table 3). Specifically from model 3 (figure 2), compared with women in the lowest quartile of residual pasta meal intake, those in the second and third quartiles had no change in the risk of developing CHD (HR=0.99, 95% CI 0.90 to 1.09 and HR=1.02, 95% CI 0.93 to 1.12, respectively), while women in the highest intake quartile had an estimated 9% reduction in risk (HR=0.91, 95% CI 0.83 to 1.00), while holding constant age, race, region, study indicators, BMI, total energy intake, per cent energy from carbohydrates, smoking status, alcohol consumption, physical activity, HEI 2005 and family history of CHD; with borderline significant linear trend (p value for trend=0.058). Results were largely similar across models 1–3 as well as when examining quartiles of pasta to GL ratio or pasta to energy ratio.
Estimates of relative risk and 95% CIs of CHD according to quartiles of pasta meal intake
Women within the highest intake quartile of pasta meal had a significantly reduced risk of developing stroke compared with those in the lowest intake quartile of pasta (HR=0.84, 95% CI 0.75 to 0.93), while those in the second and third quartiles had virtually no change in risk (HR=0.97, 95% CI 0.88 to 1.08 and HR=1.00, 95% CI 0.91 to 1.11, respectively) (table 4, figure 2). Testing for linear trend showed a significant inverse association (p value for trend=0.001), and results were highly consistent across models 1–3 as well as when examining quartiles of pasta to GL ratio or pasta to energy ratio.
Estimates of relative risk and 95% CIs of stroke according to quartiles of pasta meal intake
With ASCVD being a composite outcome of CHD and stroke, participants within the highest intake quartile of residual total pasta meal had an estimated 11% decreased risk of developing ASCVD (HR=0.89, 95% CI 0.83 to 0.96) compared with those in the lowest intake quartile in model 3, while those in the second and third quartiles had no change in risk (HR=0.99, 95% CI 0.92 to 1.06 and HR=1.03, 95% CI 0.96 to 1.11, respectively), with age, race, region, study indicators, BMI, total energy intake, per cent energy from carbohydrates, smoking status, alcohol consumption, physical activity, HEI 2005 and family history of ASCVD being constant (table 5, figure 2). Significant inverse trends were also observed, with p value for trend=0.002. Results were again highly consistent across models 1–3 as well as when examining quartiles of pasta to GL ratio or pasta to energy ratio.
Estimates of relative risk and 95% CIs of ASCVD according to quartiles of pasta meal intake
We also estimated the effects of one medium serving/day increase in pasta meal intake variables on each disease of interest by entering the continuous variables of pasta meal intake into the models as exposure instead of quartiles. These analyses had similar results to the counterparts with quartiles as exposure, but the effect sizes seemed generally larger in magnitude (online supplemental table 1). Results were also robust to adjustment for additional potential dietary confounders (online supplemental table 2).
Supplemental material
When restricting to only spaghetti meals, the results were consistent with what we observed from the primary analyses (model 3) for each of the outcomes, in terms of effect estimates, CIs, as well as p value from trend analysis (online supplemental table 3). When using age as the timescale in the Cox proportional hazards model instead of time to event, there were also no substantial changes in model estimates compared with those regarding residual total pasta meal intake in tables 2–5 (online supplemental table 4). When statistically modelling the substitution effects, replacing fried potato with pasta meal was associated with a significant decreased risk of stroke (HR=0.57, 95% CI 0.36 to 0.89) and ASCVD (HR=0.68, 95% CI 0.50 to 0.93), as well as a reduction in the risk of diabetes (HR=0.78, 95% CI 0.64 to 0.95), while there was a suggestive reduction in the risk of CHD (HR=0.84, 95% CI 0.55 to 1.28). Statistically substituting pasta meal for white bread was also associated with a significant reduction in the risk of stroke (HR=0.73, 95% CI 0.59 to 0.92), and a borderline significant reduction in the risk of ASCVD (HR=0.88, 95% CI 0.76 to 1.01), while the risk was unchanged for diabetes or CHD (table 6).
Estimates of relative risk and 95% CIs for specific diseases of interest by statistically substituting one medium serving of pasta meal for other starch-dense foods from model 3*
Discussion
In this prospective analysis of 84 555 postmenopausal women enrolled in the WHI followed until 2010, we observed a significant association between higher intakes of pasta meal and long-term risk of developing stroke and ASCVD, and a suggestive association between higher intakes of pasta meal and long-term risk of developing CHD, while no significant relation was observed between pasta meal intake and risk of developing diabetes. When we statistically estimated the substitutional effects of replacing other types of common starchy foods with pasta meal, we also found that substituting pasta for fried potato or white bread could potentially be associated with lower risk of stroke and ASCVD, and again a suggestive association was observed between substituting pasta meal for fried potato and lowered risk of CHD.
To our knowledge, our finding of the inverse relations between pasta meal intake and risk of stroke and ASCVD was the first time that such associations were reported. Measurements of body weight and adiposity are recognised as important risk factors for cardiometabolic diseases, and we considered our findings in the context of previous evidence relating pasta meal intake to these measurements. A cross-sectional analysis in two Italian cohorts, the Moli-sani study and the Italian Nutrition and Health Survey, which included over 20 000 participants, demonstrated that higher pasta meal intake was associated with better adherence to Mediterranean diet,30 a dietary pattern with demonstrated cardiovascular benefit.31 32 The authors also found that higher pasta meal intake was associated with lower BMI, waist circumference, waist to hip ratio and lower prevalence of being overweight and obese, which was independent of adherence to Mediterranean diet and total energy intake. Similar cross-sectional associations between higher pasta meal intake and lower BMI were observed in US adults as part of the International Study of Macronutrients/Micronutrients and Blood Pressure study.33 From another analysis of the same study where 17 population samples in four countries (China, Japan, UK, USA) were included, it was also found that individuals with low risk of developing CVD, as classified by favourable profile of CVD risk factors, reported higher intake of pasta meal, among other food items such as fruits, vegetables and fish. Interestingly, in studies of empirically derived dietary patterns, pasta has sometimes been classified into unhealthful patterns,34 35 or represented on both healthful and unhealthful patterns,36 possibly due to correlations in intake level with certain groups of healthful or unhealthful food items. Therefore, the potential benefit of consuming pasta should be considered in the context of an overall healthy dietary pattern, for instance, the Mediterranean diet.
Dietary GI and GL have been positively linked with the risk of a number of cardiometabolic diseases, including metabolic syndrome,10 type 2 diabetes,11–13 37 38 CHD,14 39–41 stroke42 43 and risk factors including triglycerides,15 16 high-density lipoprotein cholesterol,15–17 low-density lipoprotein cholesterol16 and high-sensitivity C-reactive protein.18 In patients with diabetes, low-GI foods have been consistently associated with better glucose control in the blood.19 We consider the low-GI nature of pasta a major reason why we observed inverse associations with risk of stroke and ASCVD, given the assumption that pasta was the primary component of the pasta meals that we included in assessing the exposure, which remained unchanged when pasta meal intake was standardised by total energy intake or GL, and the benefit remained when statistically replacing white bread or fried potato, both with high GI, with pasta. Moreover, previous systematic reviews assessing the effect of pasta on body weight and biochemical intermediaries indicated that pasta meal intake did not adversely affect adiposity and reduced body weight and BMI, although a large amount of unexplained heterogeneities were found among previous studies.44 In the TOSCA.IT study, glucose control, BMI, low-density lipoprotein cholesterol, triglycerides and the prevalence of obesity were not significantly different across the quartiles of pasta meal intake in people with type 2 diabetes.45 Taken together, available evidence indicates that greater intake of pasta meal may have a beneficial effect on cardiometabolic risk profile particularly in affecting ASCVD risk. In the context of unchanged total carbohydrate intake and total energy intake, pasta meal intake appeared not to be associated with type 2 diabetes risk.
Ours was the first prospective study to report potential inverse associations between pasta meal intake and long-term incident cardiometabolic disease risk in a well-characterised national cohort of postmenopausal women with high-quality follow-up. However, several limitations should be considered when interpreting the results. Total intake of pasta meal in this study was measured by summing the semiquantitative intake frequencies of pasta meals which had other commonly used ingredients such as cheese or tomato. Since the data were collected via FFQ, we could not obtain information on the proportion of pasta content within a specific pasta meal, and how much the additional ingredients of the meal may influence its association with cardiometabolic outcomes. To the extent possible, we accounted for other aspects of participants’ diet by adjusting for their overall quality of dietary intake. Additional adjustment for total intake of cheese or tomato also did not substantially change the results. The source of production or the types of pasta consumed (eg, regular or whole grain or legume based, or the type of flour used in manufacturing) may lead to different GI or GL. We attempted a sensitivity analysis excluding types of pasta meal with potentially different GL such as macaroni and cheese, and the results were similar to those in the primary analysis. Finally, the findings presented here stemmed from a cohort of postmenopausal women and the overall consumption of pasta meal was relatively low (average of 1 serving/week), which may have partially influenced the observed lack of association with diabetes risk, and further analysis within cohorts of men or both sex with higher levels of consumption should be conducted to evaluate the prospective associations between pasta meal intake and risk of cardiometabolic disease. Further work to confirm these observations is warranted in additional high-quality prospective cohort studies of diverse populations.
In conclusion, in this large and prospective cohort of postmenopausal women followed for up to 20 years, pasta meal intake did not have any adverse effects on risk of diabetes and may be associated with significant reduced risk of stroke and ASCVD. Substituting pasta meal for other commonly consumed starchy foods such as fried potato or white bread may possibly represent a feasible and easy-to-implement method of DM to improve cardiometabolic outcomes.
Data availability statement
Data will make avaviable subject to distrubtion policiy of the Women's Health Initiative (WHI) research program and the National Institute of Health (NIH).
Ethics statements
Ethics approval
Ethical approval of all protocols was obtained from the institutional review boards (IRBs) of all participating institutions (40 clinical site IRBs, the coordinating centre IRB and ethical review at the National Institutes of Health). Please refer to the following website for more information: https://www.whi.org/about/SitePages/StudyOrganization.aspx.
Acknowledgments
We would like to acknowledge all WHI investigators and participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MH and KL contributed equally.
Correction notice The article has been corrected since it was published online. The affiliations of the authors were incorrect which have been updated.
Contributors MH analysed the data, drafted and revised the manuscript. KL and JL assisted in data analysis and manuscript revision. MA, WCW and SL critically reviewed the analyses and revised the manuscript. SL obtained funding for the work, oversaw the entire process of study design, data analysis, manuscript drafting and revisions. All authors read, edited and approved the final manuscript, and have taken due care to ensure its integrity. MH, KL, JL, MA, WCW and SL participated in the study design; searched the literature; collected, analysed and interpreted the data; and wrote the manuscript.
Funding MH and SL were partly supported by fund donated to Brown University by Barilla. The Women’s Health Initiative (WHI) programme was funded by the National Heart, Lung and Blood Institute (NHLBI), the National Institutes of Health and the US Department of Health and Human Services through contracts HHSN268201100046C, HHSN268201100001C, HHSN268201100002C, HSN268201100003C, HHSN268201100004C and HHSN271201100004C. R01DK125403
Disclaimer The funding sources had no role in study design, data collection, data analysis, data interpretation or the writing of this report, and in the decision to submit the manuscript for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.