Article Text

Abstract
Background Malnutrition is a global emergency, creating an overlapping burden on individual, public and economic health. The double burden of malnutrition affects approximately 2.3 billion adults worldwide. Following 3 years of capacity building work in Kolkata, with assistance of local volunteers and organisations, we established an empowering nutrition education model in the form of a ‘mobile teaching kitchen (MTK)’ with the aim of creating culinary health educators from lay slum-dwelling women.
Aims To evaluate the piloting of a novel MTK nutrition education platform and its effects on the participants, alongside data collection feasibility.
Methods Over 6 months, marginalised (RG Kar and Chetla slums) women underwent nutrition training using the MTK supported by dietitians, doctors and volunteers. Preintervention and postintervention assessments of knowledge, attitudes and practices (KAP), as well as anthropometric and clinical nutritional status of both the women and their children were recorded. The education was delivered by a ‘See One, Do One, Teach One’ approach with a final assessment of teaching delivery performed in the final session.
Results Twelve women were trained in total, six from each slum. Statistically significant improvements were noted in sections of KAP, with improvements in nutrition knowledge (+4.8) and practices (+0.8). In addition, statistically significant positive changes were seen in ‘understanding of healthy nutrition for their children’ (p=0.02), ‘sources of protein rich food’ (p=0.02) and ‘not skipping meals if a child is ill’ (p≤0.001).
Conclusion The MTK as a public health intervention managed to educate, empower and upskill two groups of lay marginalised women into MTK Champions from the urban slums of Kolkata, India. Improvements in their nutrition KAP demonstrate just some of the effects of this programme. By the provision of healthy meals and nutritional messages, the MTK Champions are key drivers nudging improvements in nutrition and health related awareness with a ripple effect across the communities that they serve. There is potential to upscale and adapt this programme to other settings, or developing into a microenterprise model, that can help future MTK Champions earn a stable income.
- cognitive performance
- dietary patterns
- malnutrition
- nutrient deficiencies
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Mobile Teaching Kitchens can be used succesfully to educate underserved communities
The measurement of changes in nutrition knowledge, attitudes and practice provides a meaninful and feasible way to measure the impact of community nutrition education interventions.
The Mobile Teaching Kitchen intiative is a scalable model, able to deliver nutrition education to participants whilst also gathering data using action research methods.
Background
Malnutrition remains a major cause for concern globally, creating an intertwining and overlapping burden on individual, public and economic health. The simultaneous existence of undernutrition and overnutrition, known as the double burden of malnutrition, is estimated to affect approximately 2.3 billion adults worldwide, with 1.9 billion overweight or obese and 462 million underweight.1
In India, the double burden of malnutrition constitutes a public health emergency, prevalent across the socioeconomic gradient. Over 33% of childhood deaths are attributed to the most severe manifestations of undernutrition, while 33.8 million children are overweight.2 In Indian adults, overnutrition increases steadily, as undernutrition stagnates.3 According to the Indian National Family Health Survey in 2016, 22.9% of women and 20.2% of men had a body mass index (BMI) below normal (<18.5 kg/m2),4 whereas 17.1% of men and 18.6% of women had overweight/obesity (>25.0 kg/m2).5 In addition to gender, malnutrition also disproportionately affects individuals by location. A percentage of 26.7% of women in rural India were underweight compared with 15.5% of urban women, often speculated to be secondary to financial differences. Similar to undernutrition in urban and rural settings, there is a difference in the prevalence of overnutrition but observed in the opposite direction. Women living in urban areas (31.4%) are more likely to be overweight compared with rural counterparts (15.1%).3 A sophisticated understanding of the global burden of undernutrition and overnutrition is becoming more clearly demonstrated by The Lancet series on the ‘The Double Burden of Malnutrition’ linking the two seemingly opposing conditions. The series is pushing the boundaries of research in this area,5 particularly around the interplay of maternal nutritional states and future offspring risk of malnutrition.6
Malnutrition remains a key priority for organisations including the United Nations (UN)7 and WHO,8 both advocating for a coordinated global approach. However, a persistent challenge remains in supporting dietary change, highlighting the difficulty of translating scientific evidence into easily understood and high-quality health promotion messages.
One notable tool to tackle the issue of translating evidence into practice is the use of teaching kitchens, which have been effective in educating healthcare professionals on nutrition topics, in a number of settings. Cooking is used as a tool to transfer skills and knowledge to participants who then educate their patients and the public to improve their diet.9 10 This model has spread into the community for the public, leading to a collection of small trials, resulting in beneficial dietary modification. However, these studies largely occurred in the USA, Australia and Brazil, where a predominant focus has been on behavioural change in medium to high income countries or educational institutions but are yet to be extensively trialled in marginalised communities.11–16 Despite this, it has been shown that using a culinary education model, in a number of settings, leads to changes in nutrition attitudes and practices.17
In February 2018, NNEdPro Global Centre for Nutrition and Health (NNEdPro), alongside the Remedy Clinic Study Group (RCSG) and the Inner Wheel Club of Greater Calcutta (IWCGC), building on previously documented capacity building work,18 launched the ‘Bhavishya Shakti Mobile Teaching Kitchen’. This project served as an intervention where the project team, including local dietitians and physicians, trained local community volunteers in basic nutritional concepts who in turn then used a ‘mobile teaching kitchen (MTK)’ to educate and empower marginalised women in two Kolkata slums: Chetla and RG Kar.
This paper assesses the efficacy and feasibility of using this MTK (online supplemental appendix 1) as a model of training to transform a group ofuntrained women in urban slums into MTK Champions, who are now culinary health educators and advocates in their local communities, while also using the intervention as a data collection opportunity.
Supplemental material
Aims
Primary aim
Evaluate the feasibility of an MTK as a nutrition education tool to create culinary health educators.
Secondary aims
Assess the nutrition and health status of consenting marginalised participants and their children (through anthropometric and clinical assessments) before and after intervention, including demographics.
Improve dietary knowledge, attitude and practices following the educational intervention, analysed before and after the intervention using a knowledge, attitudes and practices (KAP) questionnaire.
Undertake a novel feasibility of assessment of mentalising skills and cognitive flexibility of marginalised participants, assessing its correlation with changes in nutrition KAP or teaching ability.
Determine whether peer transmission of learning is a feasible method of nutrition education.
Methods
Using a participatory action research approach,19 core nutritional issues for local marginalised populations were taught to participants who originated from two marginalised communities in Kolkata: RG Kar and Chetla slums.
Participant recruitment was organic, given competing life demands and difficulties associated with the environment in which the participants lived. Volunteers were selected from interested women (mothers) who received project information from local healthcare professionals known to them through previous research. There were no formal exclusion criteria, but participants were identified from those who were able to attend the training sessions in the two marginalised communities,.
The consent process involved informing all participants of the educational intervention, data collection techniques and that their findings may be published as research. Consent was obtained using locally translated consent forms and translators, and for children, consent was taken from the parent or legal guardian.
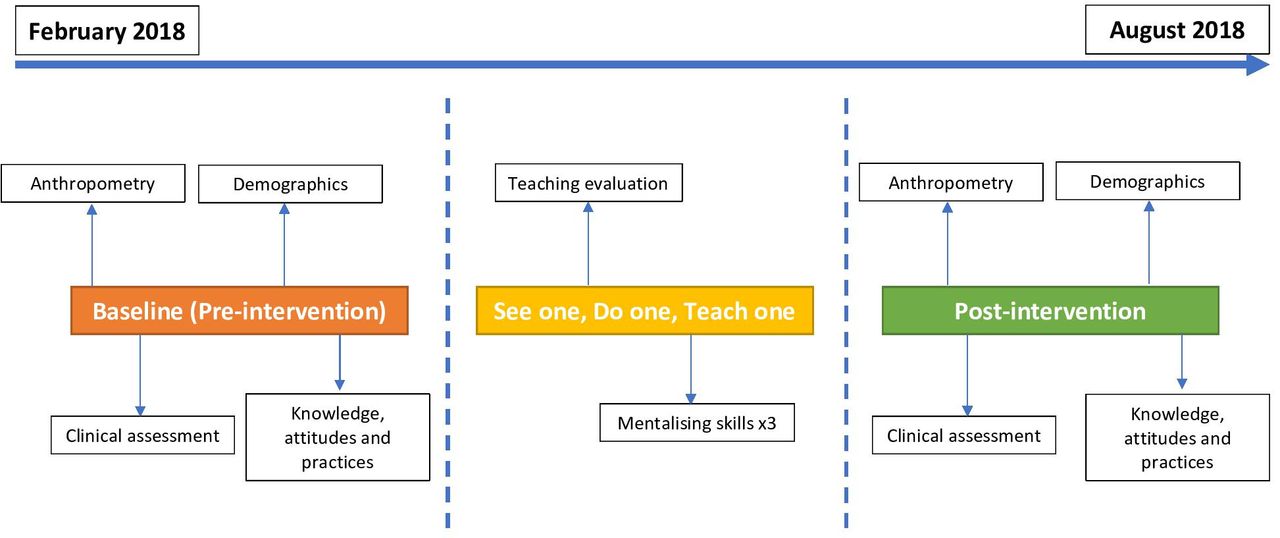
Prior to the educational intervention, a needs assessment was performed to identify participants and establish the logistics of the kitchen. The intervention was a training programme for the supporting volunteers, where they were taught how to train marginalised participants (MTK Champions) to cook and educate others using a predesigned template menu designed by local healthcare providers to address identified common nutritional deficiencies. Having been trained, the volunteers put their learning into practice, teaching the marginalised participants (MTK Champions) about the nutritional messages; this process is outlined in figure 1. Data were collected at baseline (preintervention) and postintervention, as well as during each educational session over a total period of approximately 6 months from February to August 2018 (figure 2).

Overview of the process of knowledge transmission from trained professionals through to the community.

Timeline of data collection and delivery of nutrition education (February–August 2018).
Step 1: baseline (preintervention) data collection (April 2018)
Researchers performed a number of baseline assessments, detailed further, to gain data preintervention using the local support groups, who could contact and arrange sessions, as well as translate to Bengali (the local language).
Demographics, anthropometry and clinical assessment
Age, gender, number of siblings and education level were collected for all MTK Champions and children by questionnaire. In addition, the number of children, occupation and income were collected. Both MTK Champions and their children underwent anthropometric assessment adapted from standardised techniques20; repeated measurements of height of barefoot participants standing straight-backed against the wall were obtained using a standard measuring tape, weight was measured wearing light clothing using digital scales and BMI was calculated. The same practitioner also measured the mid-upper arm circumference, taken at the midpoint between olecranon and acromion process. Local doctors then assessed participants for signs of micronutrient deficiency and undernourishment (table 1).
Clinical signs and their respective micronutrient associations
A general physical examination was performed as a basic health screen for the participants’ benefit, including respiratory, cardiovascular and gastrointestinal examination. This also provided a service to the local community as any previously unidentified abnormalities were referred to local healthcare services for appropriate investigations, treatment and follow-up. Forms for collecting information are shown in online supplemental appendices 2–4.
Supplemental material
Supplemental material
Supplemental material
Knowledge, attitudes and practices
Awareness of dietary practices were assessed using a KAP questionnaire, designed for local food preference before and after the intervention (online supplemental appendix 2). Given this questionnaire was designed for local diets and foodstuffs and was adapted from both the Indian Dietetic Association and Nutrition Society of India toolkits, it was not validated in its current form but contained validated questions. When answering, participants were instructed to describe their own diet rather than their family as a whole. The exemption to this was when asking women who were mothers to describe their children’s diets. Answers were reviewed to assess congruence with a positive response. In the knowledge section, however, responses were compared with a defined objectively correct answer. Marks for each section were converted into subsection scores for comparison of knowledge, attitudes and practices.
Step 2: See One, Do One, Teach One (SODOTO) workshops (April–May 2018)
The purpose of the teaching kitchen intervention was to engage with the local communities, deliver health and malnutrition screening sessions and teach participants to create nutritionally balanced, locally sourced, sustainable, hygienic, well-presented and affordable meals (as per a preset template menu; see nutritional breakdown in online supplemental appendix 5, analysed using Nutritics V.5.099). Furthermore, the concept aimed that participants would feel comfortable to teach their peers the menus and provide basic training in the core principles of nutrition around the meals.
Supplemental material
Volunteers with no formal nutritional training, from a local volunteer group IWCGC, were first trained in providing basic nutrition education by a local dietitian. These volunteers then passed their knowledge and training to seven initial MTK Champions from the two marginalised communities who became ‘trained champions’. Using the SODOTO methodology, these seven trained champions passed their knowledge onto a further group of participants (untrained champions) to evaluate the effectiveness of the transmission of knowledge (online supplemental appendices 6–8).
Supplemental material
Supplemental material
Supplemental material
To compensate for loss of earnings and encourage participation, the untrained champions were incentivised through food items including healthy food rations, as well as reimbursement for the ‘Do One’ and ‘Teach One’ sessions (maximum of Rs 1000 INR). Trained champions were paid Rs 500 INR per educational session (maximum of Rs 1500 INR) for their time and effort, including the previous education from volunteers, they also received food incentives.
In the ‘See One’ session, trained champions used the MTK to demonstrate to the untrained champions how to cook a nutritionally balanced, affordable, tasty and locally sourced meal. On the next ‘Do One’ visit, the untrained champions cooked the template on their own, with assistance where required. On their final ‘Teach One’ visit, the untrained champions taught a group from the local community who opportunistically assembled.
Throughout each session, participants were tested on mentalising skills and cognitive flexibility: a novel aspect of the proposed work. Mentalising skills are described as the ability to perceive and interpret human behaviour in terms of intentional mental states (eg, needs, desires, feelings, beliefs, goals, purposes and reasons). A lot of mentalising is not conscious, deliberate or reflective but rather intuitive and implicit.21 The mentalising skills assessments were performed using two validated tasks (online supplemental appendix 8) named ‘The unexpected transfer task’ and ‘Wisconsin card sorting test’. The ‘Unexpected transfer task’ was a test of theory of mind, which usually develops from years aged 4–5 years, but has not been tested in populations such as the marginalised communities identified. The ‘Wisconsin card sorting task’ is a measure of intellectual flexibility,22 tested through a card sorting game where the rules changed throughout the game. The aim was to see if understanding more about the benefits of food, and learning how to teach this to others, would improve the participants’ cognitive flexibility; there is no evidence to our knowledge in this area; hence, this exploration was pilot in nature.
Intellectual flexibility is shown through comparison of the different levels of perseverance error, non-perseverance error and total error. Perseverance error can be described as a participant making the same mistake more than once, showing a lack of flexibility. Whereas non-perseverance error occurs when a participant is trialling a different rule, in a method to identify the underlying rule through trial and error.22
In the ‘Teach One’ session, participants’ nutrition messaging was captured through three separate custom created teaching questionnaires per participant: both trained and untrained champions completed a self-assessment, followed by an assessment by a trained (IWCGC) volunteer. Untrained champions were further assessed by a trained champion peer (forms used are in online supplemental appendix 7). Possible scores were poor (one mark), average (two marks), good (three marks) and excellent (four marks) on each of the following categories: food handling and hygiene, cooking skills, understanding of the importance of a balanced diet, retention of knowledge, skills gained and ability to explain and teach others.
Step 3: postintervention data collection (August 2018)
Anthropometric measurements and clinical status assessment were repeated on the champions and children after the teaching kitchen intervention to allow for a longitudinal analysis of nutrition and health status. The KAP questionnaire was also performed again postintervention for comparison with baseline.
Data storage and analysis plan
Data were collected on paper surveys, stored securely in a local office and transcribed into electronic format. Comparison analyses were conducted of the baseline (preintervention) and postintervention anthropometric measures and nutrition KAP of the champions using the Mann-Whitney U test to account for interslum and longitudinal differences. Statistical analyses were completed on Microsoft Excel.
Results
Demographics
Twelve champions and 10 children were identified across the two slums. At baseline, the combined groups of champions had a mean (SD) age of 29.9 (8.6) years across both slums: 31.6 (9.7) years in Chetla and 26.4 (6.2) years in RG Kar. The children had a combined mean (SD) age of 5.8 (2.3) years across both slums: 6.0 (2.5) in Chetla and 5.6 (2.2) years in RG Kar.
All champions were domestic helpers (n=8) or housewives (n=6). In Chetla slum, the most common occupation was housewife (n=4), compared with RG Kar, which was evenly split.
The average income bracket selected across the slums was between Rs 2000 and 4999 INR per month; however, this varied between Chetla and RG Kar, with Chetla’s being Rs 2000–4999 INR (n=5) and RG Kar’s being less than Rs 2000 INR (n=4).
The majority of the champions were educated to primary level (up to class IV) (n=6). The maximum level was up to UK college standard (XII standard) or above (n=1), and the lowest level was no formal education (n=4). In Chetla, the most common level of education reached was primary level (n=4), whereas in RG Kar, the majority received no formal education (n=4). Full breakdown is demonstrated in table 2.
Demographic data for RG Kar and Chetla MTK Champions (n=12)
The children comprised four girls and six boys. In Chetla, a registered slum, all children attended formal education. However, in RG Kar, only two out of five children were attending formal learning.
Anthropometric measurements of champions
Table 3 demonstrates the anthropometric measurements in each slum at baseline (preintervention) and postintervention. Significant changes in anthropometry were not anticipated as the intervention primarily focused on micronutrient and protein deficiencies. At baseline, the champions from Chetla had statistically significantly higher BMI by 6.1 m/kg2 (p=0.03) compared with their RG Kar counterparts. This persisted postintervention (mean difference of 5.1 m/kg2, p=0.05). There was no statistically significant difference in mean height, weight or MUAC at baseline or postintervention.
Anthropometric measurements of all champions in RG Kar and Chetla slums (n=12)
Comparison of the combined mean across both slums at baseline versus postintervention showed no statistically significant changes for height (1.25 cm, p=0.54), weight (−0.6 kg, p=0.89), BMI (−0.7, p=0.89) or MUAC (−0.7 cm, p=0.56) postintervention, as was expected in this timeframe.
Anthropometric measurements of children
Baseline (preintervention) and postintervention height, weight, BMI and MUAC for Chetla and RG Kar children are shown in table 4. Due to small sample sizes, interslum comparisons were not possible to calculate. Comparison of combined mean measurements at baseline versus postintervention showed no statistically significant differences.
Anthropometric measurements of children in Chetla slum (n=4) and RG Kar slum (n=5), including mean measurements across both groups (n=9)
Clinical assessment of MTK Champions
In RG Kar slum, one of the MTK Champions had gingivitis at baseline, which resolved by the postintervention review, two champions had pallor at baseline and one developed pallor postintervention. In Chetla at baseline, all champions had pallor, two also had angular stomatitis. Postintervention, no clinical sign of micronutrient deficiency was identified in the Chetla champions. Overall, a total of 11 signs of micronutrient deficiency were identified at baseline, while postintervention, three (all pallor) were seen, as demonstrated in online supplemental appendix 9. The most prevalent clinical sign identified over the course of the study was pallor (66.7%).
Supplemental material
Knowledge, attitudes and practices
At baseline, the combined KAP subsections were as follows (mean (SD)): knowledge 11.7 (1.05), attitude 40.6 (0.74) and practice 23.4 (1.24). Following the intervention the scores were found to be change by +4.8 (knowledge), −3.8 (attitude) and +0.8 (practice). Individual questions were compared for the whole group at baseline and postintervention with the following questions found to be statistically significant, understanding of healthy nutrition for their children (question 1: change of 1.00 score, p=0.02), sources of protein rich food (question 3: change of 1.08 scores, p=0.02) and not skipping meals if a child is ill (question 13: change of −1.83 scores, p=<0.001). While no other statistically significant changes were seen, full breakdown can be seen in table 5.
Breakdown of knowledge, attitude and practice scores of Chetla and RG Kar slums (n=12)
Teaching assessment
Self-assessments were undertaken by all MTK Champions (n=12), and peer assessment was undertaken for those previously untrained, missing one participant (n=5). Trained volunteer assessment was performed for all MTK Champions (n=12); all results are shown in table 6.
Breakdown of self, peer and trained volunteer mean assessment scores of RG Kar, Chetla and combined slum results (n=12)
In a combined sample of the MTK Champions from both slums, participants who received primary education higher than level IV scored the highest overall in the ‘Teach One’ session with mean (SD) score of 2.6 (0.4) followed by those who received primary education, mean 2.36 (0.41). Participants with no formal education scored the least with a mean of 2.05 (0.19). This may suggest a relationship between the level of education and performance of the participants during the ‘Teach One’ step, as seen in figure 3.
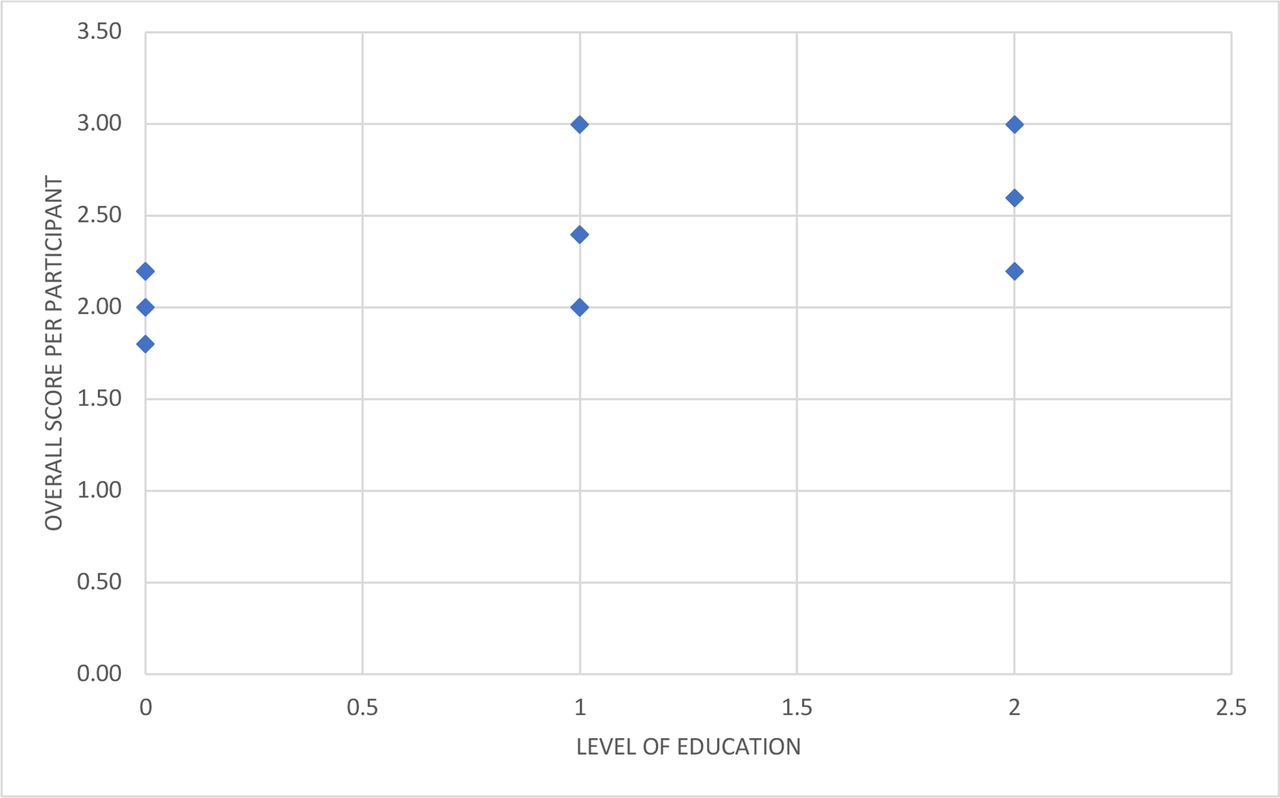
Level of education of RG Kar and Chetla women compared with their ‘Teach One’ response score.
Additionally, women who were housewives scored higher than those who were employed (mean (SD) 2.36 (0.17) and 2.29 (0.50), respectively). Women with low income (<2000/− per year) scored higher (2.4 (0.20)) than those who earned between 2000/− and 4999/ (2.27 (0.39)) and above 5000/− (2.33 (0.61)), although all these values vary minimally and currently lack any implications for selecting appropriate candidates (online supplemental appendix 10).
Supplemental material
Mentalising skills and cognitive flexibility
In the ‘unexpected transfer task’, almost all MTK Champions were able to answer the three questions correctly. However, in Chetla, one participant did not, despite multiple explanations of the test over three separate occasions. All MTK Champions in RG Kar were able to answer the three questions correctly.
Of the slums, one participant from Chetla slum only completed the test once, as well as another who only managed two of the three possible attempts. These have been included given the small sample size, as demonstrated in table 7.
Wisconsin card sorting test results for both slums (total n=12, two participants had incomplete results)
Discussion
We successfully piloted and evaluated an MTK providing nutrition education to members of two marginalised urban slum communities while assessing its feasibility using mixed methods data collection techniques. With help from local volunteers, this project was conducted on a modest budget with the estimated cost being Rs 491 800 INR (approximately £5122.34 GBP) over a 6-month period. This included all 6-monthly operational costs: procurement, storage, upkeep and driver for the MTK van, cooking ingredients and secretarial support. The one-time costs of procuring and refitting a secondhand mobile unit/van (approximately £12 000) are separate from the aforementioned operational costs estimate.
Our results suggest physical signs of micronutrient deficiencies were less common 6 months postintervention compared with baseline. This may be due to improved dietary patterns and/or differences in subjective physical assessment. However, firm conclusions around direct impact on micronutrient deficiencies cannot be drawn from this study design due to the potential confounders and small sample size; furthermore, the MTK model is geared at primary prevention of nutritional deficiencies rather than treatment, which requires individual-level clinical management. Measures of weight, height, MUAC and BMI were successfully performed thus implying anthropometric data collection is feasible as part of the MTK educational sessions. Not unexpectedly, there were no significant changes in these measures postintervention from baseline. However, there was an increase in the MTK Champions’ nutrition knowledge and practice scores following peer education, with key topics such as the importance of childhood nutrition and protein sources significantly increasing. This suggests the SODOTO approach is a viable educational tool in this context, aligning with a previous review that demonstrated improvements in KAP through culinary teaching methods.17 The small number of participants limits the extrapolation of the findings.
Much of the existing evidence assessing teaching kitchens as an educational tool are from university, institutional or higher socioeconomic community settings.9–16 There are examples of the use of teaching kitchens in lower socioeconomic settings, including Kenya23 and Ecuador.24 However, we believe this intervention is unique in that the ‘Bhavishya Shakti’ Teaching Kitchen model is the first of its kind to assess the use of MTKs in a socioeconomically deprived community through a peer educational model. Thus, allowing trained lay, local volunteers to educate in a range of different settings, including other marginalised communities or indeed the public. By including participants from two different marginalised communities, this is a more diverse population, comparing uptake in both a government registered (Chetla) and unregistered (RG Kar) community. As the intervention is relatively low cost, it could be trialled elsewhere, including adapting or replicating in higher socioeconomic areas or other low to middle socioeconomic regions, or indeed adapting to further urban or indeed rural settings.
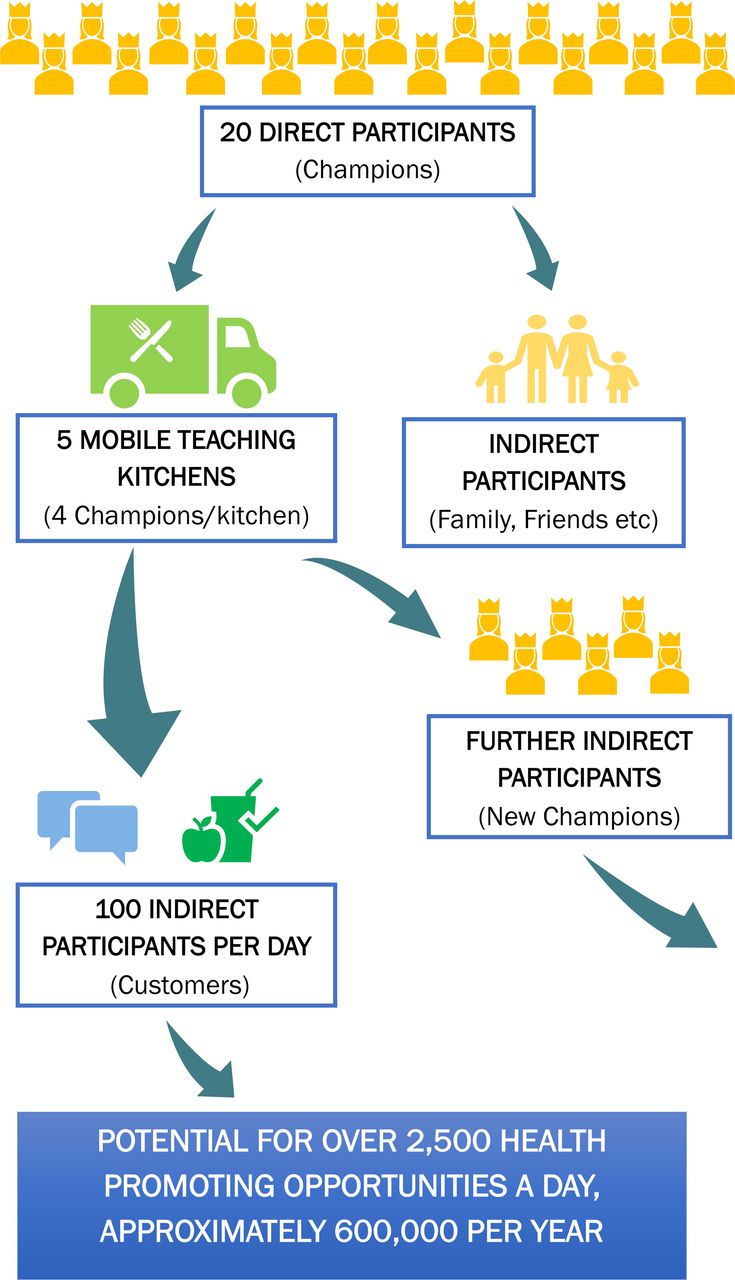
The potential impact of this educational model based on training a relatively small number of MTK Champions could be underestimated if it was to solely focus on the participants or indeed their immediate families and community as the beneficiaries. While they do receive nutrition advice, which can help them improve their families and their own health as well as those of their counterparts in the same slums, they are specifically empowered and supported to share this with wider members of the public across all echelons of society. Hence, the MTK intervention is designed as part of an inherently scalable microenterprise model: educating and empowering the MTK Champions with the competence and confidence to run an MTK, make and sell food and provide opportunistic nutrition education to customers and their peers. Figure 4 outlines the potential expansion of each MTK intervention within its community, demonstrating the potential number of people in a community that could be reached through a ‘train the trainers’ approach, far beyond the MTK Champions alone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimated multiplicative impact of translating the Mobile Teaching Kitchen Champions training into a microenterprise model.
Existing research into culinary education techniques highlight the following elements as being important for designing successful projects: encouraging self-efficacy, setting clear outcome expectations, knowledge, encouraging family and social support, minimising barriers and maximising opportunities, and ensuring sustained reinforcement.25 These key elements of social cognitive theory were explored in a feasibility methodology by the mentalising skills data collected during this project. Prioritising these in the recruitment (eg, by screening for empathy and intellectual flexibility) and training of future champions could help maximise the sustainability of future MTK projects.
There are important limitations to discuss. The small sample size significantly limits internal and external validity of the results, and while statistical tests of significance were performed, their extrapolation remains limited from a group of 12 participants. Furthermore, many of the clinical assessments, particularly examination for physical signs, are subjective and open to the effects of chance, confounding and bias. These could be avoided in future by using biochemical (ie, of blood and urine) tests of micronutrient levels rather than physical assessments as well as parallel study designs contemporaneous with the MTK but specifically geared to measure impact on individual-level nutritional status. Such tests could also more accurately quantify changes in clinical parameters due to dietary intervention. Anthropometric measurements are also prone to subjective inconsistencies or error, as demonstrated by the 3 cm discrepancy in the average Chetla adult height from baseline to postintervention. This highlights the importance of incorporating standardised training of research personnel when replicating this work, alongside nutrition education. Individual subjectivity is also a clear limitation of the KAP questionnaire, with another that it tests perception of knowledge rather than knowledge itself. Use of the KAP questionnaire may be more accurate when implemented according to Food and Agriculture Organisation (FAO) guidance,26 which should be a focus in future to standardise collected data.
Interestingly, broader positive impacts of this intervention were witnessed in the field but not represented in the measurements outlined in the results. Apart from the champions being trained to a level where they can deliver simple nutritional messages about the food they cook, the MTK can be a platform for selling healthy meals, thus improving the health and knowledge of their community and providing a new source of household income for the champions. This goes some way to addressing socioeconomic deprivation, which is a major driver of malnutrition, something the champions and their community were very supportive of. Furthermore, there were anecdotally reported psychosocial benefits for the champions, namely being empowered to fulfil new leadership and peer-educator roles within their communities. These added effects warrant further research in this, and future, programmes. Outputs of the project and are summarised on a dedicated microsite,27 including a successful adaptation and replication in rural India (Punjab), as well as the establishment of a cooperative society co-owned by the MTK Champions to support an ongoing microenterprise model.
Tackling malnutrition in gestational and early years is a strong determinant of nutritional resilience in future generations. The MTK model directly impacts the lives and livelihoods of participating communities and strengthens community resilience by facilitating knowledge around access to cheaper healthy diets and associated information on adopting them, thereby improving food and nutrition security. Alongside strengthening and sustaining the core model in India, plans are underway to adapt and pilot the MTK initiative globally. Through this adaptation, NNEdPro would develop a powerful scalable behaviour change tool for improved nutrition KAP that will empower marginalised communities (in developing and developed countries) to gain livelihoods while improving nutrition and health outcomes across society. In March 2021, at a practical level, launched the MTK Cookbook at the University of Cambridge Festival, with a live cook along led by an executive chef along with a registered dietitian, a registered nutritionist, a registered nurse and a licensed doctor demonstrating that the MTK recipes are low cost and relatively easy to prepare but are very nutrient rich and healthy. Furthermore, in April 2021, we also had the opportunity to present at policy level, alongside the UN Assistant Secretary General responsible for the Scaling Up Nutrition movement, as well as FAO leaders including the Deputy Director-General, on the applicability of the MTK model in the context of food supply and choices, nutrition and health as well as sustainability as part of the dialogue preceding and feeding into the UN Food Systems Summit. NNEdPro is poised and ready to adapt, pilot, spread and scale the MTK model over coming years to gain maximum impact from this innovation.
Conclusions
It is now estimated that malnutrition affects approximately 2.3 billion adults worldwide, including 462 million who are underweight and 1.9 billion who are overweight or obese. In addition to that, in the wake of COVID-19, deep fractures in food systems are exposed, and many more women and children have and will likely become food insecure and at increased risk of malnutrition worldwide. There is an urgent need for cost-effective, innovative and adaptable actions to tackle inequalities in food and health aggravated by COVID-19. This creates a need for interventions aiming to promote good nutrition and health among women and children but that also address food insecurity in broader society.
The Bhavishya Shakti MTK initiative is a public health centric intervention that aims to educate and empower participants from underserved communities, to become nutrition champions. Piloted and established in two marginalised communities of Kolkata, India, it successfully trained 12 lay participants into culinary nutrition educators for their community. Alongside this, it allowed collection of anthropometric data, clinical signs and KAP scores. The main outcomes of success were improvements in nutrition knowledge and practice scores postintervention. The intervention also serves as a microenterprise opportunity, and additional socioeconomic benefits were observed, namely generating novel sources of household income and new leadership and educator roles within the community.
By focusing on the provision of healthy meals and nutritional messages, the MTK Champions have been key drivers behind nudging improvements in nutrition and health related awareness with a ripple effect across the communities that they serve.
There is potential to adapt and upscale this kind of intervention to other settings globally, across all socioeconomic gradients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
Local ethical approval was gained through the local and independently constituted ‘Institutional ethics committee of Remedy Clinic Study Group, Kolkata, India’.
Acknowledgments
Matheus Abrantes (administrative and logistical support), Sanchita Banerjee (project officer provided logistical support), Chaitali Dutta (Inner Wheel logistical support), Kashmira Ghosh (Inner Wheel logistical support), Jørgen Torgerstuen Johnsen (logistical support and strategic oversight), Marjorie Lima do Vale (video summary of the project on webpage), Asim Manna (project intern, providing logistical support), Sucheta Mitra (applied for grants and produced related documents for the project), Mala Mukherjee (Inner Wheel logistical support), Sarmila Mukherjee (Inner Wheel logistical support), Sukanya Patwardhan (support in development stages of project), Kannan Raman (India network lead providing strategic oversight), Nikitah Rajput Ray (NNEdPro Junior ambassador, provided conceptual idea of the Mobile Teaching Kitchen Van), Dr Sabayasachi Ray (Strategic oversight, implementation and coordination of activities including the MTK), Chitra Ray (Inner Wheel strategic oversight), Ananya Ria Roy (media support), Elizabeth Richards (Inner Wheel logistical support), Helena Triguiero (reviewed the template menu composition). Acknowledged organisations: Inner Wheel club of Greater Calcutta, Remedy Clinic Study Group, Global Open Data for Agriculture and Nutrition, University of Cambridge, Ulster University, UK Research and Innovation and the British Dietetic Association.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lpb_1993, @harrydecarter, @domcro, @kaikargbo1, @sbhatCVD, @pdoug99, @dr_minha, @ProfSumantraRay
Contributors Project design: LB, HC, SBhar, SBhat, DC, PD, SM, AS, MR-R, IT and SR. Project conduct: LB, HC, SB, DC, MG, SM-N, SM, AS and SR. Data collection and analysis: LB, HC, DC, SK, MK, MR-R and SR. Paper write-up: LB, HC and SR. Paper review: DC, SK, MK, SBhat, DC, PD, SM-N, SM, MR-R, IT and SR.
Funding The project undertaken during the period of this research paper was supported by funds from the following two grants: (1) 2018: Global Challenges Research Fund Joint Award and (2) 2018: University of Cambridge Interdisciplinary Research Centre Project Incubation Award.
Competing interests None declared
Provenance and peer review Not commissioned; externally peer reviewed by Shailaja Fennell, UK; Marjorie R Lima Vale, NNEdPro Global Centre for Nutrition and Health.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.