Article Text

Abstract
Background Poor mental well-being is a major issue for young people and is likely to have long-term negative consequences. The contribution of nutrition is underexplored. We, therefore, investigated the association between dietary choices and mental well-being among schoolchildren.
Methods Data from 7570 secondary school and 1253 primary school children in the Norfolk Children and Young People Health and Well-being Survey, open to all Norfolk schools during October 2017, were analysed. Multivariable linear regression was used to measure the association between nutritional factors and mental well-being assessed by the Warwick-Edinburgh Mental Well-being Scale for secondary school pupils, or the Stirling Children’s Well-being Scale for primary school pupils. We adjusted all analyses for important covariates including demographic, health variables, living/home situation and adverse experience variables.
Results In secondary school analyses, a strong association between nutritional variables and well-being scores was apparent. Higher combined fruit and vegetable consumption was significantly associated with higher well-being: well-being scores were 3.73 (95% CI 2.94 to 4.53) units higher in those consuming five or more fruits and vegetables (p<0.001; n=1905) compared with none (n=739). The type of breakfast or lunch consumed was also associated with significant differences in well-being score. Compared with children consuming a conventional type of breakfast (n=5288), those not eating any breakfast had mean well-being scores 2.73 (95% CI 2.11 to 3.35) units lower (p<0.001; n=1129) and those consuming only an energy drink had well-being scores 3.14 (95% CI 1.20 to 5.09) units lower (p=0.002; n=91). Likewise, children not eating any lunch had well-being scores 2.95 (95% CI 2.22 to 3.68) units lower (p<0.001; 860) than those consuming a packed lunch (n=3744). In primary school analyses, the type of breakfast or lunch was associated with significant differences in well-being scores in a similar way to those seen in secondary school data, although no significant association with fruit and vegetable intake was evident.
Conclusion These findings suggest that public health strategies to optimise the mental well-being of children should include promotion of good nutrition.
- dietary patterns
- mental health
- nutrition assessment
Data availability statement
Data are available on reasonable request. The data underlying this article were provided by Norfolk County Council under permission. Data will be shared on request to the corresponding author after consideration for permission by Norfolk County Council.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Nutrition is important for childhood growth and development, but little research has investigated nutrition in relation to mental well-being, therefore, the relationship between nutrition and well-being in children of school age is not known.
What this study adds
In this study nutritional intake was associated with mental well-being scores in both primary and secondary school children.
Higher fruit and vegetable consumption was significantly associated with better mental well-being in secondary pupils. Also, the type of breakfast and lunch consumed, by both primary and secondary pupils, was significantly associated with well-being.
In a class of 30 secondary school children, 4 had nothing to eat or drink before starting classes in the morning, and 3 had nothing to eat or drink before starting classes in the afternoon.
The difference in mental well-being between children who consumed the most fruits and vegetables compared with the lowest was of a similar scale to those children experiencing daily, or almost daily, arguing or violence at home.
The associations found between nutrition and mental well-being in our study mean that strategies to improve nutrition in schoolchildren need to be investigated and implemented.
Introduction
The mental well-being of individuals of all ages is a significant public health issue, and population surveys suggest that the prevalence of low mental well-being in children and young people is rising.1 Potential reasons for this increase include social and economic changes resulting in children living with their parents for long and delaying development of autonomy,2 the pressures of social media,3 and stresses of modern school culture.4 There is a growing recognition of the importance of mental health and well-being in early life, in particular with evidence of the strong association of adolescent mental health problems persisting into adulthood and leading to poorer life outcomes and achievement.5 6 Understanding and addressing the situation is not a simple task as childhood mental well-being is complex and is governed by a wide range of factors, including biological and genetic factors, demographic factors and modifiable lifestyle factors.7 Nutrition, a modifiable factor at both an individual and societal level, is an important influence on health throughout the life course, is intricately involved in development and normal functioning of the body, and thus has the potential to affect both physical health and mental well-being.8
Well-being can be defined as ‘the state of being or doing well in life’.9 Mental well-being, a term which is often used interchangeably with ‘positive mental health’, refers to ‘a state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’.10 It is recognised as having major consequences for health and social outcomes,11 and considering that more than 50% of all mental health disorders emerge before the age of 14 years,12 maintaining the mental well-being of children is paramount. Mental well-being encompasses a number of different psychological aspects including hedonic well-being, which involves an individual’s experience of happiness and life satisfaction, and eudemonic well-being which involves psychological functioning and self-realisation including the meaning and purpose of one’s life.13 The relationship of diet and nutrition with mental health and well-being in either children or adults is not fully understood, although the relevance of diet quality to physical health in relation to non-communicable disease morbidity and mortality is well established.14 Previous observational research has shown that a diet containing high levels of saturated fat, refined carbohydrates and processed food products, is associated with poorer mental health in children and adolescents,15 while higher well-being is reported by adults with greater fruit and vegetable intake16 and this is also evident in longitudinal data where adults improving their fruit and vegetable intakes experienced a concomitant increase in well-being.17 In addition, randomised controlled trial evidence in adults exists to show that a Mediterranean dietary pattern (high in vegetables, fruits and unsaturated fats) supplemented with fish oil can reduce symptoms of depression.18 There is also some rationale for the concept of a causal relationship between nutrition and mental well-being due to a number of direct effects on biological processes including oxidative processes, inflammation and immunity, and brain signalling molecules,19–22 which may affect the way an individual feels and perceives their well-being. However, despite this rationale evidence on the specific relationship between nutrition and mental well-being in children and young people is currently inconsistent and underexplored.15
On this basis, our study aimed to determine whether the self-reported dietary choices of schoolchildren participating in The Norfolk Children and Young People’s Health and Well-being Survey were associated with their self-reported mental well-being. The survey was commissioned by the Public Health department of Norfolk County Council and the Norfolk Safeguarding Children Board to gather information on health behaviours in primary and secondary school children in order to inform public health service provision.23 It includes age appropriate and validated measures of mental well-being, as well as information nutrition including fruit and vegetable intake and breakfast and lunch types, and thus provides a unique opportunity to examine the association of nutrition with mental well-being in both primary and secondary school pupils.
Materials and methods
Data collection
Data were collected by a health and behaviour survey (The Norfolk Children and Young People Health and Well-being Survey 2017) from over 50 schools in Norfolk, UK, by the Schools and Students Health Education Unit. The survey was commissioned by Norfolk County Council Public Health and the Norfolk Safeguarding Children Board. The target population was all school children in Norfolk. The survey was offered to all educational establishments for children in years 5– 13 inclusive (including further education (FE) colleges, special schools, independent schools and pupil referral units). Results were received from 30 primary schools and 26 secondary schools and FE colleges. In total 10 853 pupils completed the survey (this was 9% of Norfolk primary school children in the target year groups, 22% of secondary pupils and approximately 6% of young people in years 12 and 13). The survey was open for a 4-week period in October 2017. It was completed online by pupils in a classroom setting (a paper option was given but all schools chose to complete the survey online). Two versions of the survey were used: one developed for primary school children over the age of 8 years; and the other for secondary school pupils. Age-appropriate questions were used to collect data on demographics, health and well-being, nutrition, living/home situation, and adverse childhood experiences. Mental well-being was assessed by age-appropriate validated measures: the Warwick-Edinburgh Mental Well-being Scale (WEMWBS)11 for secondary -school pupils or the Stirling Children’s Well-being Scale (SCWS)24 for primary school pupils. WEMWBS assesses eudemonic and hedonic well-being as well as psychological functioning and subjective well-being.11 WEMWBS is scored by participants indicating how often on a 5-point Likert scale from 1 ‘none of the time’ to 5 ‘all of the time’ that they feel like each of 14 statements addressing feeling and functioning aspects of mental well-being; the scores of each statement are summed to give a total score with a range of 14–70. SCWS consists of 12 statements covering areas of well-being including: optimism, cheerfulness and relaxation; satisfying interpersonal relationships; clear thinking and competence; it is scored using a Likert scale in the same way as WEMWBS and has a total score range of 12–60. Higher scores on both scales indicate greater mental well-being.
Study population and variables
Secondary school pupils
Valid mental well-being scores were available for 8511 individuals (82.5% of the total 10 315 listed in the survey dataset). Data were available to analyse well-being scores together with the variables listed below for 7570 individuals (88.9% of those with well-being data, and 73.4% of the total). Data collected by the survey included the WEMWBS well-being score (the outcome variable), nutrition variables (exposures) and other covariates relevant to well-being. Nutrition variables included fruit and vegetable consumption, type of breakfast consumed and type of lunch consumed. These represent different aspects of nutrition which are useful to investigate to inform public health strategies. Nutrition-related covariates: alcohol consumption, free school meal status and weight satisfaction. Demographic covariates: age group, gender, sexuality, ethnicity, deprivation quintile (Index of Multiple Deprivation25). Health covariates: disability status, long-term illness status, smoking status, vaping status, drug use. Living/home situation covariates: living situation, whether they have their own bedroom, whether they have their own bed, number of hours they provide care to others, parental smoking status. Adverse experience covariates: whether they feel safe at school, whether they feel safe at home, whether they have been bullied, whether they have bullied others, whether they witness arguing at home, whether they witness violence at home. All questions had a number of possible answers which could be chosen. For example, data on what children consumed for lunch was captured by the following question: ‘What did you do for lunch yesterday? If you weren’t at school/college yesterday, think about the last time you were in school/college all day.’ Students were asked to choose one of the following options: ‘School/college food, ate a packed lunch from home, bought lunch from a takeaway or shop, went home for lunch, did not have any lunch.’ Guidance was provided where appropriate to help students to answer the questions accurately. For example, fruit and vegetable intake was captured by the question: ‘How many portions of fruit and vegetables did you eat yesterday.’ Students were able to choose an option from 0 to 8. They were also given the following guidance: ‘To help you decide, all of these examples count as ONE portion: ONE portion=80 g=any of these…1 apple, banana, pear, orange or other similar sized fruit, 3 heaped tablespoons of vegetables (raw, cooked, frozen or tinned), 1 cupful of grapes, cherries or berries, 1 glass (150 mL) of fruit juice (however much you drink, fruit juice counts as one portion a day), 1 dessert bowl of salad. N.B. Potatoes don't count when thinking about 5-a-day.’ All secondary school pupil variables used and the categories defining them are shown in table 1.
Characteristics of the secondary school group (n=7570)
Primary school pupils
Valid mental well-being scores were available for 1413 (90% of the total 1570 individuals listed in the survey dataset). After data cleaning, we had complete data available to analyse well-being scores together with the variables listed below for 1253 individuals (88.7% of those with well-being data and 79.8% of the total). Primary school pupil data available from the survey included the same variables as the secondary school dataset with the omission of the following variables due to their inappropriate use for younger children: sexuality, deprivation quintile, smoking status, vaping status, drug use, alcohol consumption, whether they feel safe at school, whether they feel safe at home, whether they witness arguing at home, and whether they witness violence at home. All primary school pupil variables used and the categories defining them are shown in table 2.
Characteristics of the primary school group (n=1253)
Statistical analyses
Associations between mental well-being scores and specific variables were first explored by conducting unadjusted bivariate tabulations. We then created a multivariable model for well-being (as a continuous variable) which adjusted for any variables identified as significant in the bivariate analyses with a p<0.05 threshold level. All comparisons have been made against a reference category for each variable, identified by (ref) in the tables. Due to collinearity which would exist in a multivariable model we generated combined variables for ‘disability’ and ‘long-term illness’ and ‘arguing’ and ‘violence’ at home. We also removed ‘own bedroom’, due to overlap with ‘own bed’, and simplified the categories for other variables to reduce complexity of interpretation and increase the number of children in individual categories, and hence the statistical power of comparisons. Variables that have been recoded include: the nutrition variables, fruit and vegetable consumption, type of breakfast consumed and type of lunch consumed; and other covariates, sexuality, ethnicity, deprivation, alcohol consumption and free school meal status, weight satisfaction, living situation and care provision. For example, fruit and vegetable consumption was recoded from nine categories (0, 1, 2, 3, 4, 5, 6, 7 or 8 units) to four categories (0, 1 or 2, 3 or 4, or 5 or more). We have used complete case analysis where we excluded individuals with missing data for any of the variables included in the full regression model.
Results
Selected characteristics of the two groups, secondary school and primary school, are shown in tables 1 and 2, respectively. The mean mental well-being score, according to WEMWBS, was 46.6 (SD 10.9) in secondary school children and, according to SCWS, was 46.0 (SD 8.4) in primary school children. In terms of nutrition, only 25.2% of secondary school children and 28.5% of primary school children in this survey reported consuming the recommended 5-a-day fruits and vegetables, with 9.8% and 9.1%, respectively, consuming no fruits or vegetables. Also noteworthy is the proportion of children consuming only a non-energy drink or nothing for breakfast (21.1% secondary and 11.7% primary), and the proportion of secondary school children consuming no lunch (11.4%).
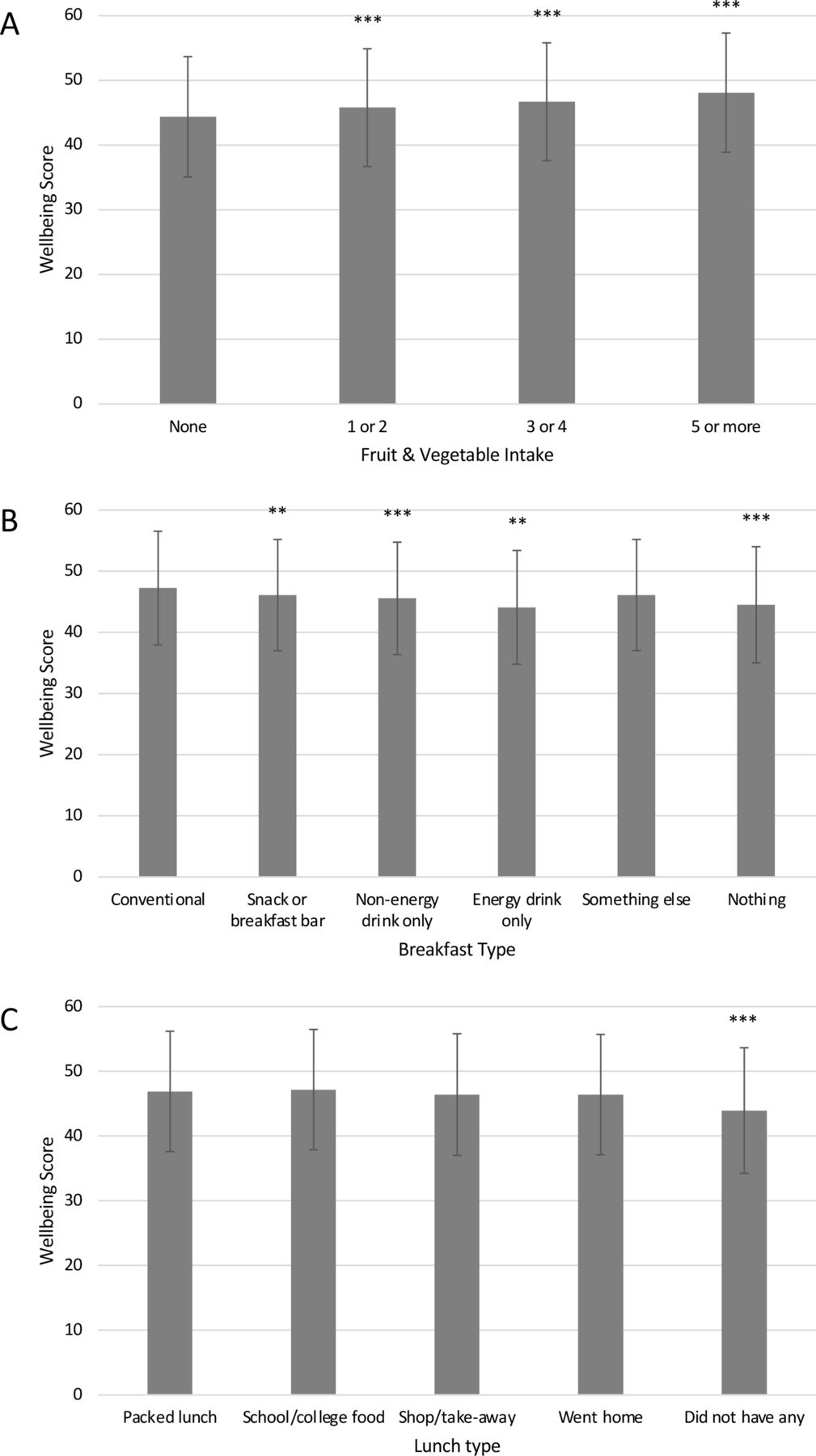
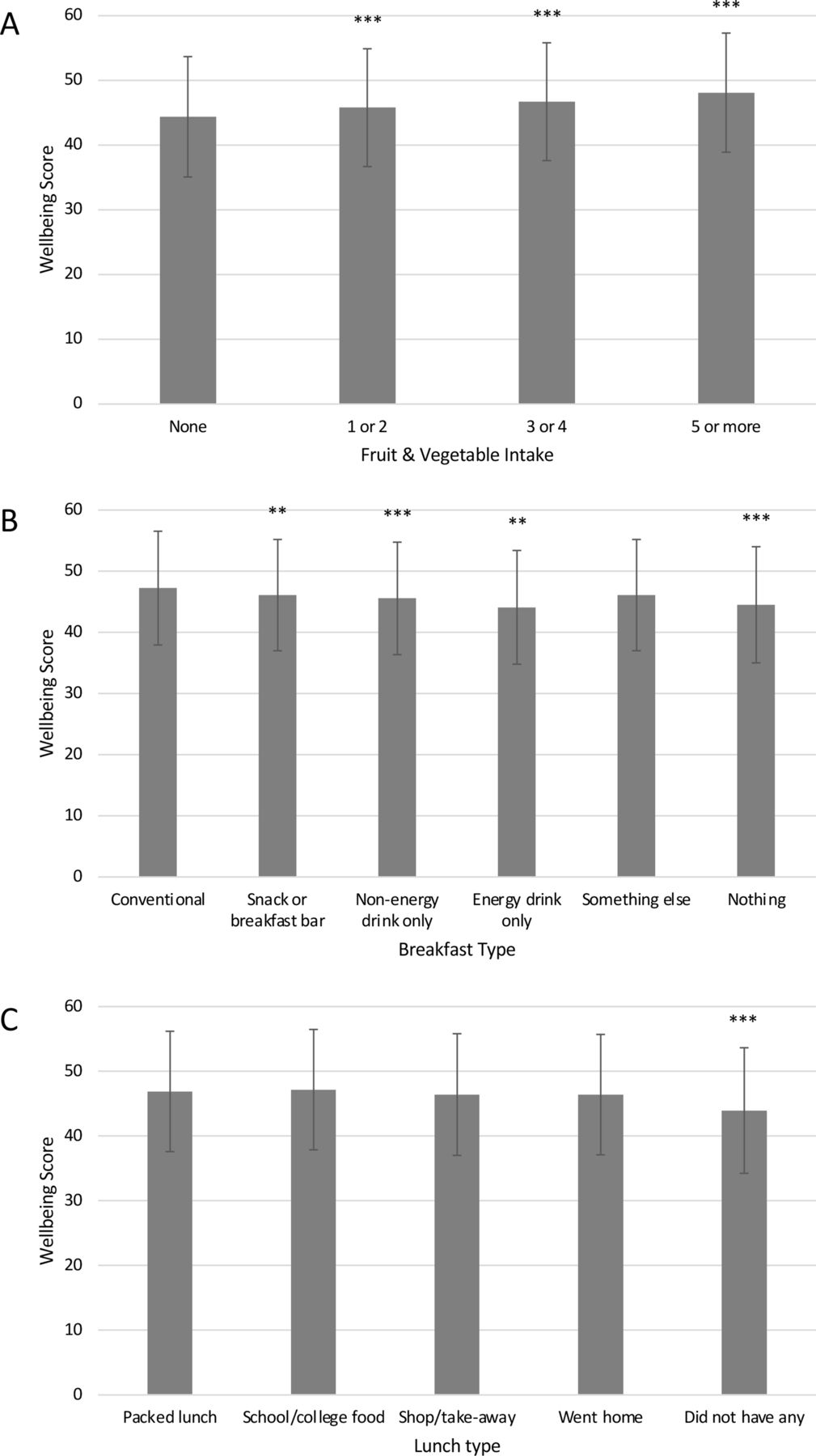
In multivariable analysis of secondary school data, our model had an R2=0.318 and thus explained approximately 32% of the variance in total mental well-being score. In this model, mental well-being scores were significantly associated with nutrition related variables (fruit and vegetable intake, breakfast type, lunch type, alcohol intake and weight satisfaction), demographic variables (age group, gender, sexuality, ethnic group), health variables (disability or long-term illness, vaping and drug use), living/home situation variables (feeling safe at school and feeling safe at home) and adverse experience variables (been bullied, bullied other and witnessed argument/violence at home) (see table 3). As the focus of this study, the significant associations of fruit and vegetable intake, breakfast type and lunch type, with mental well-being scores are highlighted in figure 1 and described here. Higher combined fruit and vegetable consumption was significantly associated with higher mental well-being (see figure 1A). Compared with those consuming no fruits or vegetables (n=739): Consuming one or two portions was associated with well-being 1.42 units higher (p<0.001, n=1986); consuming three or four portions was associated with well-being 2.34 units higher (p<0.001, n=2940); and consuming five or more portions was associated with well-being 3.73 units higher (p<0.001, n=1905). Type of breakfast was also significantly associated with well-being (see figure 1B). Compared with those consuming a conventional type breakfast (eg, toast, porridge, cereal, yoghurt, fruit, cooked) (n=5288): Consuming only a snack or breakfast bar was associated with well-being 1.15 units lower (p=0.009, n=484); consuming only a non-energy drink was associated with well-being 1.68 units lower (p<0.001, n=469); consuming only an energy drink was associated with well-being 3.14 units lower (p=0.002, n=91); and not eating any breakfast was associated with well-being 2.73 units lower (p<0.001, n=1129). Similarly, lunch consumption was also significantly associated with well-being (see figure 1C). Compared with those consuming a packed lunch (n=3744): Not eating any lunch was associated with well-being 2.95 units lower (p<0.001, n=860).
{kind=link}
Fully adjusted1 mean well-being scores (WEMWBS) of secondary school pupils according to (A) fruit and vegetable intake, (B) breakfast type and (C) lunch type. 1Adjusted for fruit and vegetable intake, breakfast type, lunch type, free school meal status, alcohol intake, weight satisfaction, age group, gender, sexuality, ethnic group, deprivation, disability or long-term illness, smoking, vaping, drug use, parental living situation, own bed, hours spent caring, parental smoking, feels safe at home, feels safe at school, been bullied, bullied others, argue/violence at home. Data are plotted as mean±SD. **P<0.01, ***p<0.001, versus reference group according to ANCOVA. ANCOVA, analysis of covariance; WEMWBS, Warwick-Edinburgh Mental Well-being Scale.
Multivariable model for well-being and nutrition in secondary school children (n=7570)
In primary school multivariable analyses, our model had an R2=0.236, and associations between nutritional variables and mental well-being scores were also apparent (see table 4). Compared with those consuming a conventional type breakfast (n=1083): Consuming only a snack was associated with well-being 5.50 units lower (p=0.001, n=27); consuming only an drink was associated with well-being 2.67 units lower (p=0.036, n=37); and not eating any breakfast was associated with well-being 3.62 units lower (p<0.001, n=90). Compared with those consuming a packed lunch (n=840): Eating school food was associated with well-being 1.27 units lower (p<0.010, n=371); and having no lunch was associated with well-being 6.08 units lower (p=0.006, n=12), although this figure should be interpreted with caution due to the low number of children in this group.
Multivariable model for well-being and nutrition in primary school children (n=1253)
Discussion
The importance of good quality nutrition for childhood growth and development is well established. Our study adds to this prior evidence the finding that nutrition is also highly relevant to childhood mental well-being. As a potentially modifiable factor, both at an individual and societal level, nutrition may therefore represent an important public health target for strategies to address childhood mental well-being. Our data of Norfolk children show associations between nutritional variables and mental well-being scores exist in both primary and secondary school pupils. Higher combined fruit and vegetable consumption was significantly associated with higher mental well-being in secondary school pupils, and the type of breakfast and lunch consumed by both primary and secondary school pupils was also significantly associated with well-being. A number of particularly relevant observations can be derived from our results. First, fruit and vegetable consumption by secondary school pupils showed a linear pattern of association with mental well-being scores, such that those consuming five or more portions had higher well-being than those consuming three or four, who in turn had higher well-being than those consuming one or two. Second, consumption of energy drinks by secondary school children as a substitute for breakfast was associated with particularly low mental well-being scores, even lower than for those children consuming no breakfast at all. Third, the associations of nutritional variables with mental well-being are already apparent in the younger children which is a concern. Using multivariable regression analysis to model nutrition exposures with adjustments for important known demographic and environmental influences, including adverse experiences, provides us some confidence that these associations are real, but does not fully remove the possibility that they are a result of other factors at play.
Our approach has enabled us to determine the relative importance of the different nutritional exposures (fruit and vegetable consumption, and breakfast and lunch meal choices). Moreover, the magnitude of the differences in mental well-being scores between the different nutrition categories identified in this study are notable, particularly in comparison to other influences on childhood well-being such as the 2.95 units lower well-being of those secondary school children witnessing arguing or violence at home every day or almost every day. Thus the effect size of nutritional variables, for example, the 3.73 units higher well-being seen in secondary school children consuming five or more portions of fruits and vegetables per day, compared with those consuming none, really serves to highlight the importance of nutrition and supports the UK public health advice for the whole population to eat ‘5-a-day’ fruits and vegetables.26 Although the proportion of children eating 5-a-day in this survey is relatively high in comparison to national data,27 the majority of children (more than 7 in 10 in both primary and secondary school groups) are not meeting the 5-a-day target and approximately 1 in 10 children reported no fruit and vegetables intake. Uptake of the 5-a-day message is known to vary with socioeconomic status, and difficulties exist in some groups of the population in accessing these foods, so there remainsscope for improvement which needs to be addressed at a national policy level. According to our data, in a class of 30 secondary school pupils, approximately 21 will have consumed a conventional-type breakfast, and at least four will have had nothing to eat or drink before starting classes in the morning. Similarly, at least three pupils will go into afternoon classes without eating any lunch. This is of concern, and likely to affect not only academic performance at school (there is evidence that breakfast is particularly important for cognitive function in children),28 but also growth and development if the nutritional deficit is not rectified.
The biological and psychological mechanisms of well-being are complex and incompletely understood. While our study specifically focused on investigating links between nutritional factors and mental well-being in young people, our additional findings also corroborate previous studies showing other factors including behavioural and demographic factors to be important.29 30 Many of these represent logical associations, for example, adverse experiences or difficult living situations are associated with lower well-being scores, and although the direction of causality is not necessarily proven, the relationships are predictable. The effect of nutrition and dietary choice by contrast is less patent, but nevertheless there is some plausible potential biological basis for the association of better diet quality with mental well-being. At a fundamental level, sufficient nutrition is required to provide the building blocks for the normal development and function of the body in both children and adults, including cell growth and replication, synthesis of DNA, neurotransmitter and hormone metabolism, and particularly critical to children, optimal nutrition is of importance for brain development.31 Indeed, in early childhood the development of the brain proceeds with greater speed than the rest of the body, making it particularly at risk of nutritional deficiency acting as a rate limiter.32 In adults we know, from a recent systematic review of research, that fruit and vegetable intake is positively associated with broad aspects of mental health,33 and other studies have shown specific nutritional deficiencies to be associated with mental health issues, including the association of insufficient dietary intake of magnesium, folate, and zinc, with depression,34 and long-chain n-3 fatty acids with anxiety.35 Dietary intake also has direct effects on a number of biological process including oxidative processes, inflammation and immunity, and brain signalling molecules: An unhealthy diet is associated with increased inflammation36 which is pertinent as systemic inflammation is often higher in patients with depression19; and high-fat, high-sugar diets affect proteins critical to brain development, including brain-derived neurotrophic factor,20 concentrations of which have been shown to correlate with severity of symptoms in patients with depression.21 22
This study is, to our knowledge, the first to specifically investigate the association between fruit and vegetable intakes, breakfast and lunch choices, and validated assessment of mental well-being in UK schoolchildren. Our findings corroborate and build on findings from previous research in the UK,29 and Australia,37 which have shown unhealthy eating behaviours to be associated with poorer well-being29 and health related quality of life37 in adolescents. We acknowledge the limitations of the cross-sectional nature of this study and the survey methodology, in particular the lack of detailed nutritional information and the reliance on self-reported data from children. Nevertheless, our study has several strengths. These include the wide uptake of the survey by schools in Norfolk, thus providing a large representative sample of the population, and the use of validated measures of well-being for both secondary (WEMWBS11) and primary school children (SCWS24). Reporting fruit and vegetable consumption relies on a certain degree of understanding of what constitutes a portion. Since all nutritional data were self-reported and were not validated, for example, against nutrient biomarkers, it is possible that there is some inaccuracy in the dietary data reported. Inadequate understanding of portions by the younger primary school children may partly explain the lack of association seen between fruit and vegetable consumption and well-being in this group, while better understanding in the older secondary school children allowed the association to be evident. The demographic adjustment of the primary school data is also likely to be less robust, due to lack of availability of deprivation data. Not all questions asked of the older pupils were included in the primary school version of the survey; an a priori decision made by a multidisciplinary team at Norfolk County Council during the survey design process, which we acknowledge is a limitation in our analyses. The diet of an individual represents a complex mixture of foods and nutrients consumed together, and therefore, although somewhat simplistic, our categorisation of different types of breakfast and lunch provides meaningful data in addition to analysis of specific fruit and vegetable intakes.This is particularly useful in surveying children where reporting accuracy may limit the reliability of more detailed dietary data collection. Indeed, the inclusion of primary school data which corroborates the findings of associations between nutrition and well-being in older children, is a particular strength of this study.
Conclusions
These findings provide important information to advance our understanding of the nutritional and other factors involved in childhood mental well-being. Public health strategies and school policies should be developed to ensure that good quality nutrition is available to all children both before and during school in order to optimise mental well-being and empower children to fulfil their full potential.
Data availability statement
Data are available on reasonable request. The data underlying this article were provided by Norfolk County Council under permission. Data will be shared on request to the corresponding author after consideration for permission by Norfolk County Council.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank all the schools that signed up to the study, the pupils for their participation, and NCC public health staff for their work planning and implementing the survey.
References
Supplementary materials
Press release
Footnotes
Contributors RH, BR and AW developed the research question, before agreeing a research strategy in conjunction with ABC and CG. RH analysed the data and drafted the manuscript and following peer review carried out additional analyses and made amendments with input from ABC, CG and AW. All authors contributed to data interpretation, review of the manuscript and its approval.
Funding The survey was commissioned by Norfolk County Council Public Health and the Norfolk Safeguarding Children Board, and the UEA Health and Social Care Partners provided funding to support RH’s work on this project at UEA.
Competing interests BR, CG and SJLS are employed by Norfolk County Council who commissioned the survey.
Provenance and peer review Not commissioned; externally peer reviewed by Dr. Emmanuel Baah, University of North Carolina System.