Article Text

Abstract
Background This study investigated the cost-effectiveness of vitamin D3 supplementation in older adults in Ireland, with year-round vitamin D deficiency (serum 25-hydroxyvitamin D concentration <30 nmol/L) (13% of Irish adults), from the perspective of the Health Service Executive.
Methods Three age groups were investigated: (1) ≥50 years, (2) ≥60 years and (3) ≥70 years. Based on the clinical literature, vitamin D3 supplementation may: (1) decrease all-cause mortality by 7% and (2) reduce hip fractures by 16% and non-hip fractures by 20%. A discount rate of 4% was applied to life years and quality-adjusted life years (QALYs) gained, and healthcare costs. The annual healthcare costs per patient used in the model are based on the average annual health resource use over the 5-year time horizon of the model.
Results The cost/QALY estimates in all three age groups are below the usually acceptable cost-effectiveness threshold of €20 000/QALY. The most cost-effective and least costly intervention was in adults ≥70 years. For this age group, the average annual costs and outcomes would be approximately €5.6 million, 1044 QALYs gained, with a cost/QALY of approximately €5400. The results are most sensitive to the mortality risk reduction following vitamin D3 supplementation.
Conclusion The cost-effectiveness of vitamin D3 supplementation is most robust in adults ≥70 years. Clinical uncertainty in the magnitude of the benefits of vitamin D3 supplementation could be further addressed by means of: (1) performing a clinical research study or (2) conducting a pilot/regional study, prior to reaching a decision to invest in a nationwide programme.
- nutrient deficiencies
- nutrition assessment
- nutritional treatment
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are provided in the manuscript or the manuscript references; otherwise, 'not applicable'.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is a growing interest in the cost-effectiveness of vitamin D to prevent disease. This study investigated the cost-effectiveness of vitamin D3 supplementation in older adults in Ireland, where previous research has demonstrated year-round vitamin D deficiency (25(OH)D concentration <30 nmol/L) in 13% of the adult population.
WHAT THIS STUDY ADDS
The cost-effectiveness of vitamin D3 supplementation is most robust in adults ≥70 years.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
The results of this study warrant further investigation, for example, within a GP (general medical practitioner)-monitored, vitamin D3 supplementation programme for elderly adults. Also, the results should be pertinent to the relevant decision makers, including the Irish Department of Health.
Introduction
Clinical vitamin D deficiency (serum 25-hydroxyvitamin D (25(OH)D) concentration below <30 nmol/L) increases the risk of excess mortality and disease.1 Vitamin D3 supplementation is likely to be clinically beneficial in deficiency1 but have little or no benefit for those who are replete in the vitamin. Vitamin D deficiency, as measured by serum 25(OH)D, is particularly high among older Irish adults.2
There is a growing interest in the cost-effectiveness of vitamin D to prevent disease. While several previous studies were mainly conducted in the elderly for fall and/or fractures (eg, refs 3 4), more recently, a study estimated the costs and savings for preventing cancer deaths by vitamin D supplementation of the population aged ≥50 years in Germany.5 The results of this study supported the use of vitamin D3 supplementation among older adults as a potential cost saving approach to reduce cancer mortality.5
The objective of this study is to investigate the cost-effectiveness of vitamin D3 supplementation in older adults in Ireland, with year-round vitamin D deficiency (25(OH)D concentration <30 nmol/L) (13% of adults2), from the perspective of the Health Service Executive (HSE).
Methods
Deaths and fractures avoided
The methodology used builds on that used by Niedermaier et al.5 The methodology applied to Ireland uses Central Statistics Office Irish Life Table No. 17, for males and females, for the period 2015–2017.6 The data for male and females from the Life Table were combined using Irish population statistics for 20167 and applying the method of weighted averaging. The annual mortality probability and the expected life expectancy were determined for all ages. A 4% annual discount rate8 was applied in order to calculate the discounted life expectancy. The ‘at risk’ population of interest (i.e., those with year-round vitamin D deficiency) is estimated to be 13% of the Irish population.2 This population cohort was estimated by applying 13% to the Irish population statistics for 2016 for all ages. The population data were summarised into 5-year age groups, beginning at age 50 years. The final age group was for those ≥85 years (with a mean age assumed to be 90 years, when required). For any given 5-year age group, the expected annual number of deaths is equal to the number of people in the age group multiplied by the annual mortality probability for the midpoint age of the group.
Based on the clinical literature, vitamin D3 supplementation may: (1) decrease all-cause mortality by 7%,9 of which 4.2% (of the 7%) is a reduction in cancer mortality and (2) reduce hip fractures by 16% (and related excess mortality)10 and non-hip/less severe fractures by approximately 20%.11 12 In the base-case analysis, the reduction in all-cause mortality was implemented in the model by applying a 7% reduction to the expected number of deaths occurring in each 5-year age group. This point-estimate reduction in all-cause mortality was varied over the range 1%–10% in the univariate sensitivity analysis.
The number of hip fractures in 2019 and their distribution by age were obtained from the Hip Fracture database.13 The number of non-hip fractures in 2014 was estimated from the total number of fractures and the number of hip fractures reported in the literature.14 The number of non-hip fractures was assumed to have the same relative age distribution, as was found for hip fractures. It was conservatively assumed that only 13% of people who have a fracture would have year-round vitamin D deficiency and be included in the ‘at risk’ population of interest.2 The reductions in hip fractures (16%, and the associated estimated 1-year mortality of 22% following a hip fracture15) and non-hip fractures (approximately 20%) were included in the base-case analysis and varied in the univariate sensitivity analysis.
The results obtained from the model were investigated for three age cohorts: (1) ≥50 years, (2) ≥60 years, and (3) ≥70 years.
Discounted life years and discounted quality-adjusted life years (QALYs) gained
The number of discounted life years gained for any given age group is equal to the number of deaths avoided multiplied by the associated discounted life expectancy. The number of discounted QALYs gained for any given age group is equal to number of discounted life years gained multiplied by the age-related utility value for the midpoint of the age group.
EQ-5D (a standardised measure of health-related quality of life) index population norms for the UK16 were used for age-related utility values. The following age-related utility equation was used for ages ≥50 years (which had a coefficient of determination (R2) of approximately 99%).

The disutility estimate used for hip fracture was 0.20 and for non-hip fracture was 0.09.4 These disutility estimates were applied for 1 year to estimate fracture-related QALYs gained, that is, number of fractures avoided per annum multiplied by the relevant fracture disutility.
Comparator and time horizon
The comparator is the current standard of care, which is being compared against a systematic public health programme: (1) to identify year-round vitamin D deficient adults (≥50 years), by means of serum 25(OH)D measurement, and (2) to treat such adults with vitamin D3 supplementation, under GP supervision, to render the patients vitamin D replete and to maintain their vitamin D adequacy over time.
A 5-year time horizon was employed in the sense that it was assumed that it would take 5-years for the public health programme to have identified the eligible vitamin D deficient patients and for them to have been treated for their vitamin D deficiency and to be maintained in a vitamin D replete state.
Healthcare resource use and costs
For each age group, it was assumed that the average annual healthcare cost would be the cost of treating all the eligible patients plus the cost of patient identification (ie, a serum 25(OH)D measurement in order to identify the ‘at risk’ population), with the latter ‘set-up’ cost averaged over 5 years. Thus, only those patients who are GP assessed to be year-round vitamin D deficient are subsequently treated with vitamin D3 supplementation and monitored. Vitamin D deficiency was assumed to be treated with vitamin D3 4000 IU daily for up to 10 weeks, followed by 800 IU daily thereafter. Healthcare costs included in the analysis are: serum 25(OH)D measurement, the average cost of a GP visit and drug acquisition costs of vitamin D3 supplements. Over the 5-year period, costs were discounted at 4% per annum after the first year.
The cost off-sets included in the analysis were end-of-life invasive cancer costs avoided and the costs of fractures (hip and non-hip/less severe fractures) avoided. The reduction in all-cause mortality was implemented in the model by applying a 7% reduction to the expected number of deaths occurring in each 5-year age group. This 7% reduction in all-cause mortality could be ‘partitioned’ into a 4.2% reduction in cancer mortality and a 2.8% reduction in non-cancer mortality.9 Thus, approximately 61% of the reduction in mortality was due to the reduction in cancer mortality. Invasive cancers constitute approximately 55% of all cancers.17 Thus, approx. 33% of the reduction in mortality was due to the reduction in invasive cancer mortality. Conservatively, for deaths avoided, end-of-life costs of invasive cancers avoided were the only cost off-sets included in the analysis.
Average UK end-of-life cancer costs18 were applied to Irish invasive cancer deaths, using the method of purchasing power parity (PPP), with inflation of healthcare costs to €(2020) values. Additional healthcare cost off-sets included in the analysis were due to the healthcare costs of hip and non-hip fractures avoided. The unit costs of all healthcare resource use items included in the model are summarised in table 1.
Healthcare resource use items and associated unit costs
Univariate and multivariate sensitivity analyses
The univariate sensitivity analyses and multivariate sensitivity analysis performed are summarised in table 2.
Parameterisation of the univariate and multivariate sensitivity analyses undertaken
All results of the data analysis given below were obtained using Microsoft Excel 2019, 32-bit version.
Results
Base-case results
The base-case cost-effectiveness results are summarised in table 3. The cost/QALY estimates in all three age groups are below the usually acceptable cost-effectiveness threshold of €20 000/QALY in Ireland. The most cost-effective and least costly intervention was in adults ≥70 years of age. While a public health primary prevention programme in adults ≥70 years of age would produce fewer QALYs, it would be sufficiently less costly to result in the lowest (best) cost/QALY.
Base-case cost-effectiveness of vitamin D3 supplementation in older adults with vitamin D deficiency plus results of univariate and multivariate sensitivity analyses
All additional base-case results will be focused on those obtained in adults ≥70 years of age.
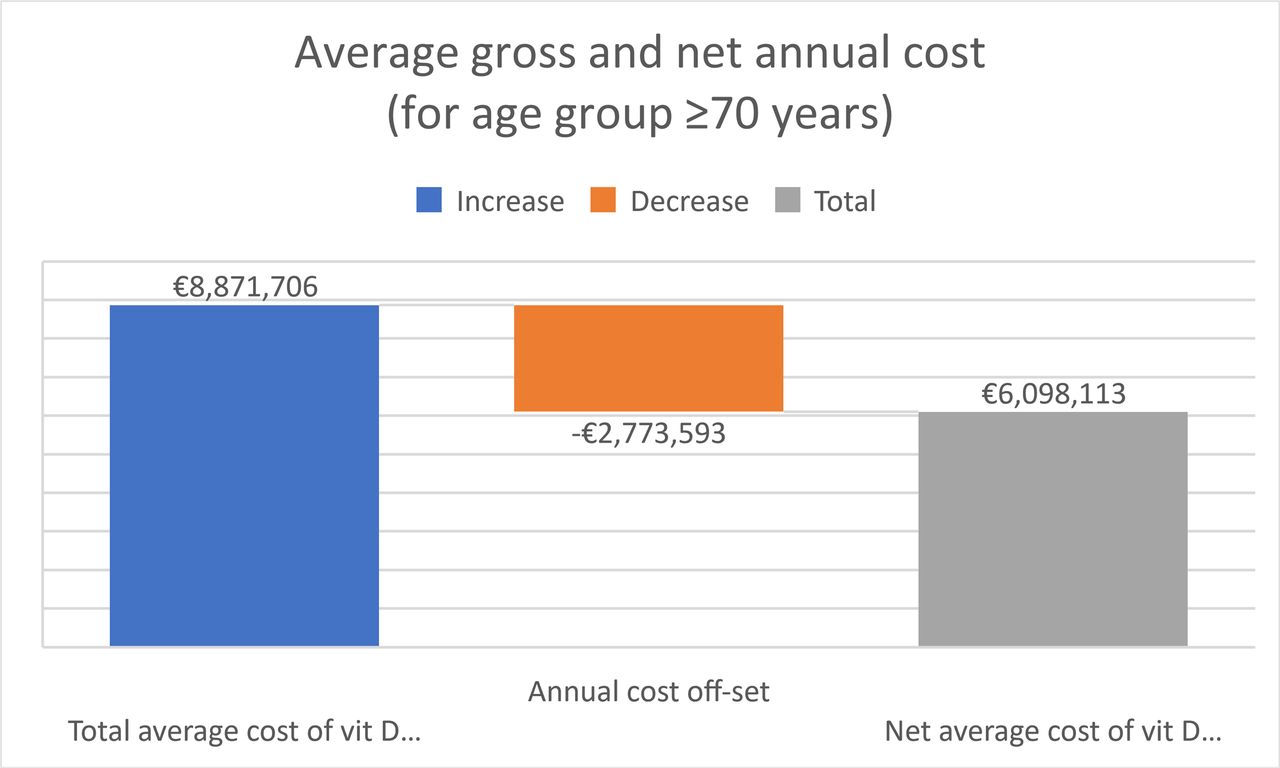
The annual healthcare cost offsets reduce the average annual costs from a total of approximately €8.4 million to approximately €5.6 million per annum for treating older adults ≥70 years, who are year-round vitamin D deficient, with vitamin D3 supplementation (figure 1).

Waterfall plot of base-case average annual total, cost off-set and net healthcare costs in older adults ≥70 years.
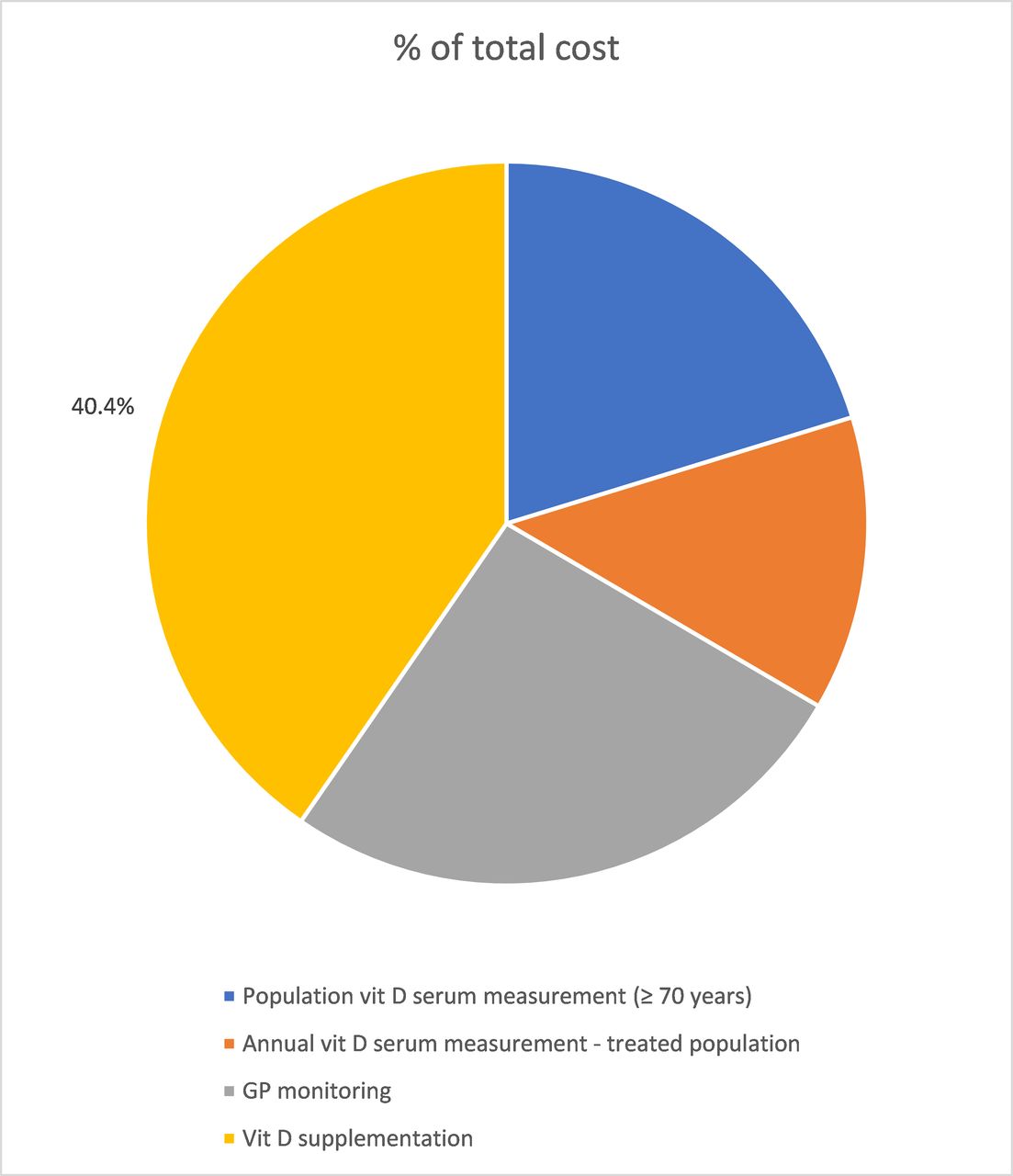
Vitamin D3 supplementation drug acquisition costs are the biggest cost component, being approximately 40% of the total €8.4 million annual healthcare costs (excluding cost offsets) (figure 2). Approximately 84% of the annual healthcare cost off-sets are the healthcare costs of fractures avoided, with the remaining approximate 16% of the annual healthcare cost off-sets due to end-of-life care costs avoided from a reduction in invasive cancer deaths.

Composition of the base-case average annual total annual costs (excluding cost off-sets) in older adults ≥70 years.
Results of the sensitivity analyses
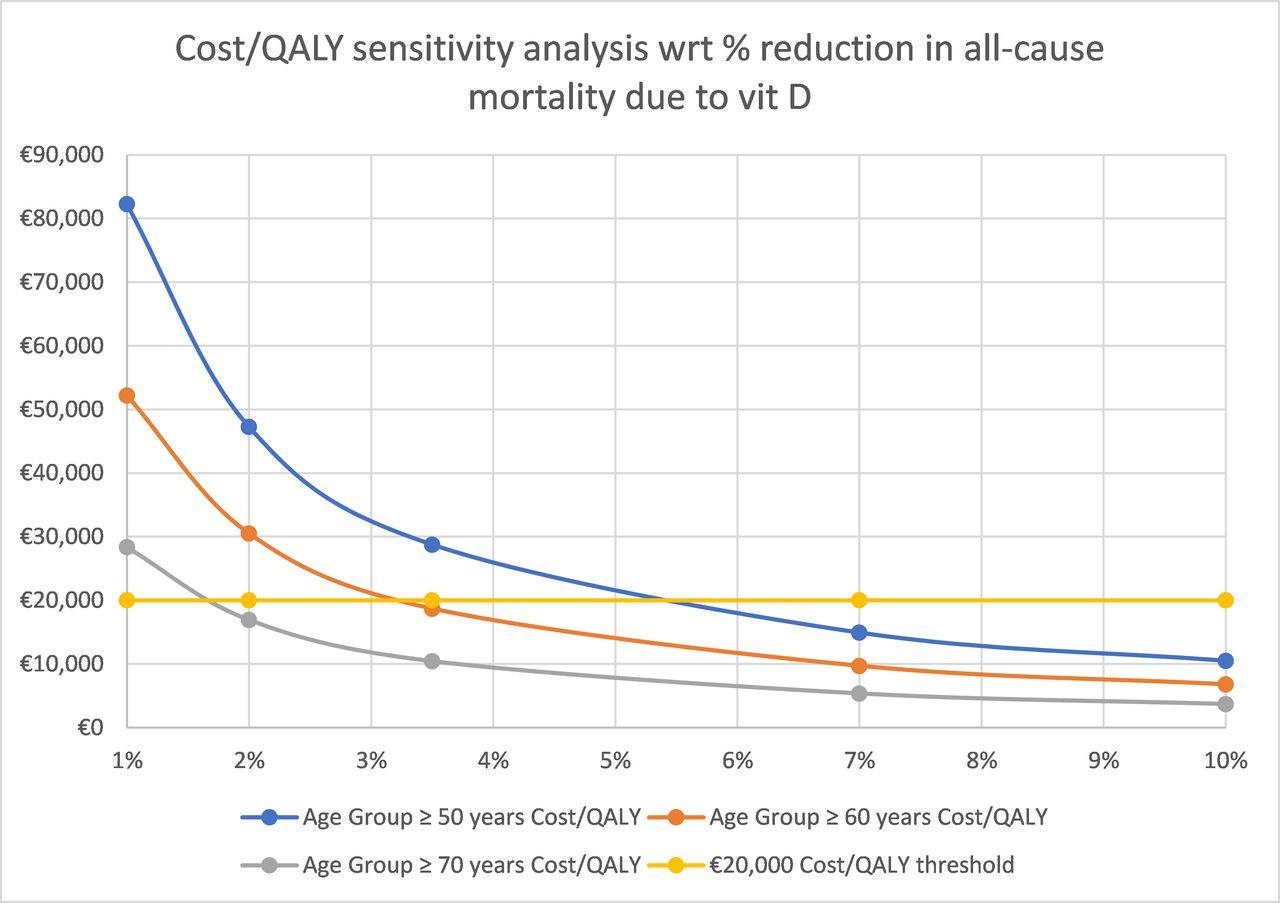
In a univariate analysis, the impact on the cost/QALY of varying the % reduction in all-cause mortality from treating older adults, who are year-round vitamin D deficient, with vitamin D3 supplementation is given in figure 3. As can be seen, for elderly adults ≥70 years of age, even if the reduction in all-cause mortality due to vitamin D3 supplementation was reduced to 2% (7% in the basecase), the cost/QALY in this age group would still be less than €20 000 per QALY gained. A similar threshold analysis can be performed for the other age groups by visible inspection of figure 3.

Univariate sensitivity analysis: impact on the cost/QALY of varying the % reduction in all-cause mortality from treating those older adults, who are year-round vitamin D deficient, with vitamin D3 supplementation (base-case=7% reduction in all-cause mortality). QALY, quality-adjusted life years.
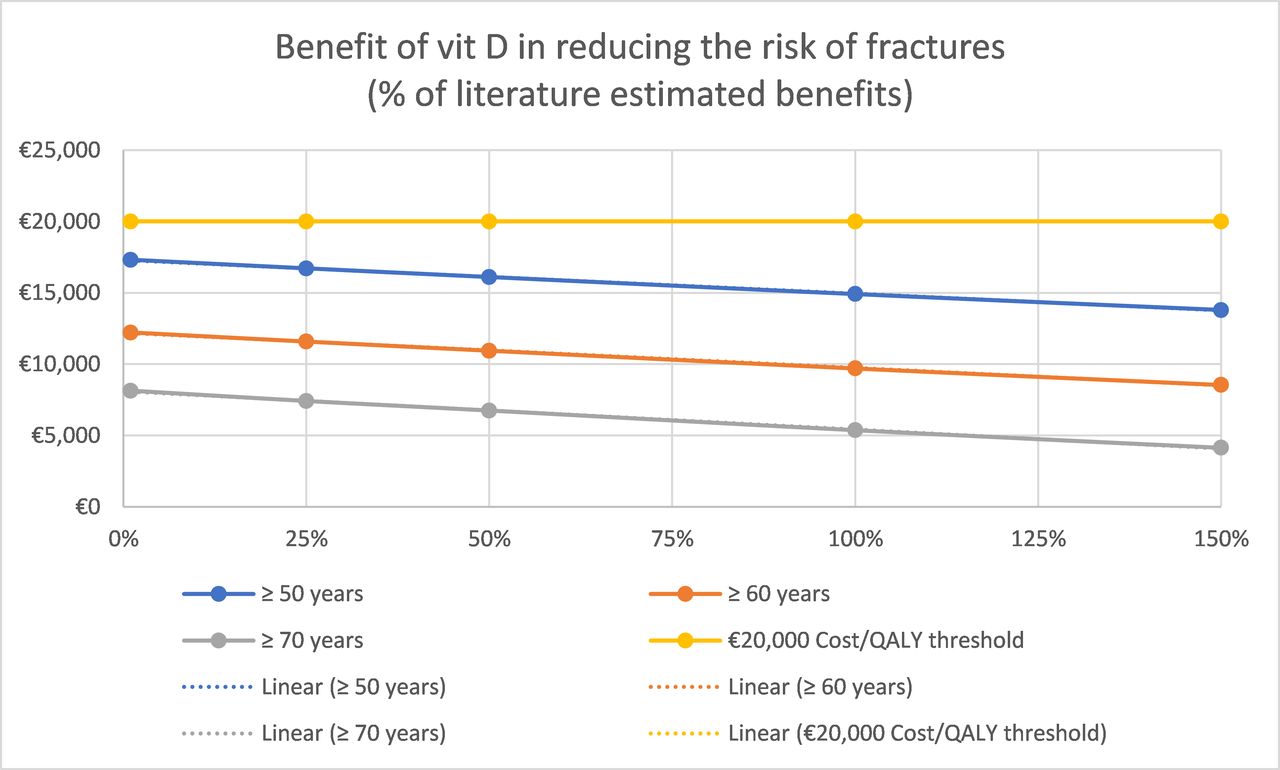
The impact on the cost/QALY of varying the risk reduction of fractures (hip and non-hip/less severe fractures) from treating older adults, who are year-round vitamin D deficient, with vitamin D3 supplementation was investigated in another univariate analysis. In all cases explored, the cost/QALY remain less than €20 000 per QALY gained for each of the three age groups (figure 4).

Univariate sensitivity analysis: impact on the cost/QALY of varying the risk reduction of fractures (hip and non-hip) from the published literature as a result of treating older adults, who are year-round vitamin D deficient, with vitamin D3 supplementation (ie, the risk reduction estimates were varied over the range 1%–150% of the literature estimates used in the base-case). QALY, quality-adjusted life years.
The impact on the cost/QALY of varying the discount rate per annum (4% in the basecase) was investigated in another univariate analysis. In all cases explored, the cost/QALY remain less than €20 000 per QALY gained for all age groups (figure 5).
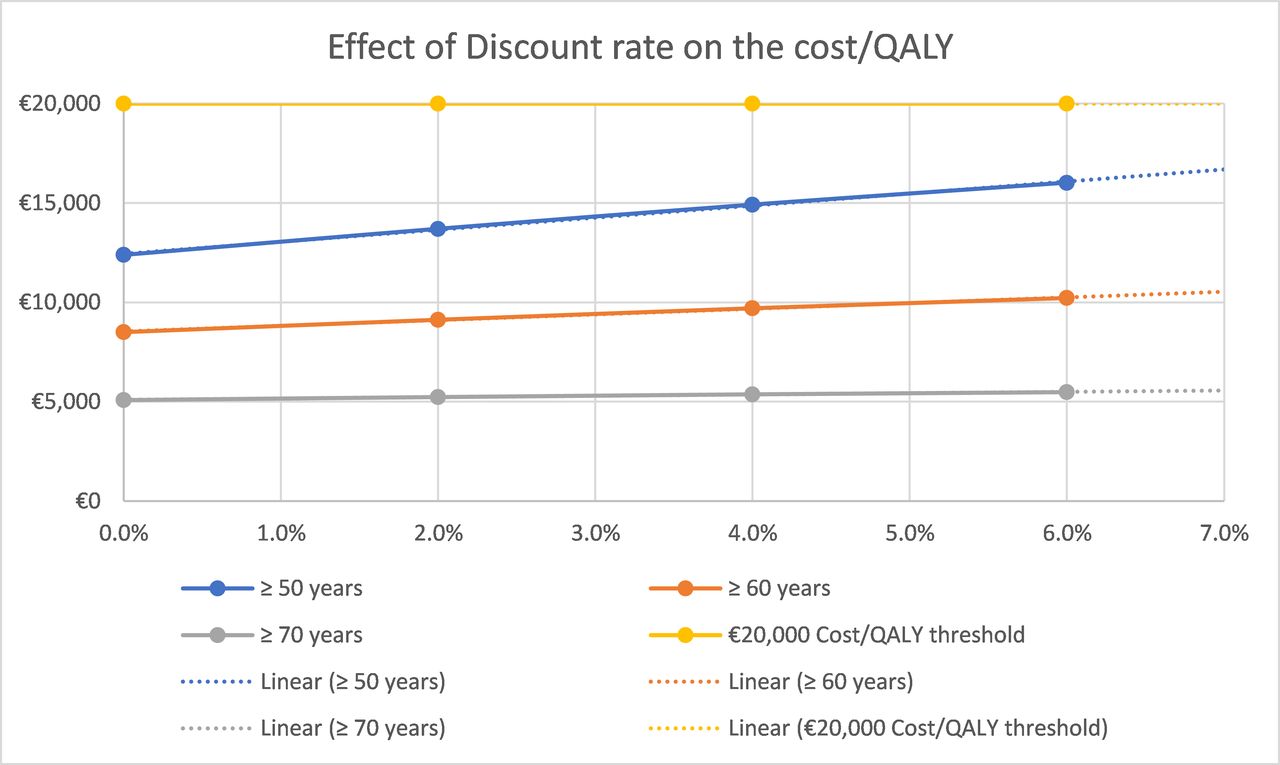
Univariate sensitivity analysis: impact on the cost/QALY of varying the discount rate for treating older adults, who are year-round vitamin D deficient, with vitamin D3 supplementation (base-case=4% discount rate per annum). QALY, quality-adjusted life year.
In terms of healthcare costs, the most uncertain are in relation to: (1) serum 25(OH)D measurement and (2) average end-of-life invasive cancer cost. By means of univariate sensitivity analyses:
The serum 25(OH)D measurement non-discounted cost was increased by 50% (compared with the basecase, from €21.50 to €32.25), which will tend to increase the cost per QALY results (table 3). While the cost per QALY results increased modestly for each age cohort compared with the basecase results, they remain below the €20 000/QALY threshold (table 3).
The average end-of-life invasive cancer cost was increased by 50% (compared with the basecase, from €6487 to €9731), as it was based on a 2005 reference.18 This cost off-set will tend to decrease the cost per QALY results (table 3).
The cost per QALY results were not very sensitive to large changes (50% increase) in either of these uncertain unit costs.
Potentially, some vitamin D deficient elderly adults may require additional serum 25(OH)D measurement, GP visit(s) per annum and/or additional course(s) of vitamin D3 supplementation to correct their vitamin D deficiency. To investigate this, a sensitivity analysis was conducted in which the average annual discounted cost of serum 25(OH)D measurement, GP visit, plus vitamin D3 supplementation acquisition cost (€120.59 in the basecase) was increased by 50% (to €180.88) (table 3). In this case, the cost per QALY results increased for each age cohort compared with the basecase results; however, for both the age groups: ≥60 years and ≥70 years, the cost per QALY were well below €20 000/QALY (table 3).
Results of a ‘pessimistic’ scenario
The parameterisation for a multivariate sensitivity analysis performed is summarised in table 2. In this case, the potential clinical benefits of vitamin D3 supplementation to vitamin D deficient elderly adults are decreased by 30% compared with the basecase, whereas the relevant healthcare costs are increased by 30%. This is regarded as a ‘pessimistic’ scenario.
In this ‘pessimistic’ scenario, the cost per QALY for the age group: ≥70 years remained well below €20 000/QALY, whereas this was no longer the case for the age group: ≥60 years, with the cost per QALY considerably above €20 000/QALY for the age group:≥50 years (table 3).
Results of a willingness to pay (WTP) threshold analysis
A WTP threshold analysis was performed to determine the minimum reduction in all-cause mortality required for vitamin D3 supplementation to be cost-effective (figure 6). At a WTP threshold of €15 000/QALY, a 7% reduction in all-cause mortality would be required for vitamin D3 supplementation to be cost-effective for the age group: ≥50 years, whereas the corresponding WTP threshold decreases to approximately €5000/QALY for the age group: ≥70 years. Also, should the reduction in all-cause mortality obtained with vitamin D3 supplementation be only 1.6% (as opposed to 7%), the cost/QALY would be €20 000 for the age group: ≥70 years. In comparison, the meta-analysis provided a lower 95% CI of approximately 2% (table 29) for the reduction in all-cause mortality obtained with vitamin D3 supplementation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Minimum % reduction in all-cause annual mortality, following vitamin D3 supplementation, required to meet the willingness to pay (WTP) threshold for each age group.
Discussion
Vitamin D3 supplementation is likely to be clinically beneficial only in deficiency1 or those who are not fully replete. Those most likely to gain maximum benefit from vitamin D3 supplementation are those with year-round vitamin D deficiency (25(OH)D concentration <30 nmol/L), which is estimated to be 13% of Irish adults.2 It is important to note that limited research has focused solely on the effects of vitamin D supplementation in those with vitamin D insufficiency at baseline; notwithstanding, a Cochrane meta-analysis has demonstrated that vitamin D supplementation, in patients with 25(OH)D concentrations <50 nmol/L, significantly reduced all-cause mortality.19 Furthermore, in a recent large (n=20 025) retrospective observational, nested case–control study in veterans with low 25(OH)D concentrations (<50 nmol/L), those who received vitamin D treatment, had a significantly lower risk of all-cause mortality.20
What has been evaluated in this paper is the healthcare costs and benefits of: (1) identifying year-round vitamin deficient adults (≥50 years), by means of serum 25(OH)D measurement, and (2) treating such adults with vitamin D3 supplementation, under GP supervision, to render the patients vitamin D replete and to maintain their vitamin D adequacy over time. It is envisaged that GP supervision could be performed through routine GP/patient interaction. However, it was also assumed that those patients identified as having year-round vitamin D deficiency would require, on average, one additional GP visit per annum, with a further additional GP visit in the year that the qualifying patient would enter the potential public health programme. It is further assumed that serum 25(OH)D measurement during the summer months is sufficient to identify those older adults with year-round vitamin D deficiency.
Although it is acknowledged that vitamin D plays a key role in calcium metabolism and homeostasis, no calcium supplements were included in the cost-effectiveness analysis, as it was assumed that adequate calcium intake by patients could be achieved through dietary advice provided as part of the GP visit. Comparing adults worldwide, Ireland ranks among the highest calcium intakes in the world via higher intake of dairy products.21 Therefore, a combined vitamin D and calcium supplement would not be expected to be required for the majority of the population.
Meta-analyses of studies investigating the relationship between vitamin D and bone fracture have limitations: including studies with short periods of patient follow-up, some measured in months, whereas only the most powerful pharmaceutical drugs have been shown to reduce hip fracture in such a short time-frame. Also, the distinction between supplementation with vitamin D and calcium in combination compared with vitamin D supplementation ‘alone’ is an artificial one in the context of this paper, as it is being proposed that patients would receive dietary advice from their GP to encourage adequate calcium intake by patients.
The cost-effectiveness modelling assumed that patient identification and treatment with vitamin D3 supplementation would take some years to be achieved. Also, the benefits of treating vitamin D deficiency would take time to be manifested in terms of clinical benefits. Therefore, it was assumed that a ‘steady-state’ would be achieved by the end of 5 years from initiation of the public health programme. For each age group, it was assumed that the average annual healthcare cost would be the cost of treating all the eligible patients plus the cost of patient identification, with the latter ‘set-up’ costs averaged over 5 years. It is unknown, however, whether this time frame would be sufficient to capture the potential benefits of vitamin D3 supplementation on reducing all-cause mortality or reducing the risk of fractures.
The cost/QALY estimates in all three age groups are below the usually acceptable cost-effectiveness threshold of €20 000/QALY in Ireland. The most cost-effective and least costly intervention was in adults ≥70 years of age. While a public health primary prevention programme in adults ≥70 years of age would produce fewer QALYs, it would be sufficiently less costly to result in the lowest (best) cost/QALY. Therefore, it is proposed that a GP-monitored, vitamin D3 supplementation public health programme be considered in adults ≥70 years of age in the first instance.
The cost-effectiveness results could potentially be improved if additional clinical benefits of vitamin D3 supplementation had been included in the model, for example, decreasing the incidence of respiratory tract infections and the adverse clinical consequences than can arise from such infections.22 In addition, a conservative approach was taken where applicable. For example, the cost off-sets due to cancer end-of-life care were limited to invasive cancer care costs only, with invasive cancers constituting approximately 55% of all cancers.17
The results of the cost-effectiveness analysis are most sensitive to the mortality risk reduction following vitamin D3 supplementation. For elderly adults ≥70 years of age, it was found that even if the reduction in all-cause mortality due to vitamin D3 supplementation was reduced to 2% (7% in the basecase), the cost/QALY in this age group would still be less than €20 000 per QALY gained. However, potentially the reduction in all-cause mortality due to vitamin D3 supplementation could be less than this.
Typically, the uncertainty in cost-effectiveness analysis can be assessed through probabilistic sensitivity analysis (PSA). A PSA was not performed in this study. However, the nature of the clinical evidence base for vitamin D3 supplementation may not be very suitable for clinical uncertainty to be assessed in such a manner. The clinical uncertainty might be better addressed by means of: (1) performing a clinical research study prior to reaching a decision to invest in a GP-monitored, vitamin D3 supplementation public health programme or (2) conducting a pilot/regional study prior to reaching a decision to invest in a nationwide programme.
Conclusion
The cost/QALY estimates of a GP-monitored, vitamin D3 supplementation public health programme in the three age groups: (1) ≥50 years, (2) ≥60 years and (3) ≥70 years are below the usually acceptable cost-effectiveness threshold of €20 000/QALY in Ireland. The cost-effectiveness of vitamin D3 supplementation is most robust in adults ≥70 years. The results of the cost-effectiveness analysis are most sensitive to the mortality risk reduction following vitamin D3 supplementation. It is proposed that a GP-monitored, vitamin D3 supplementation programme be considered in adults ≥70 years of age in the first instance.
Data availability statement
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. All relevant data are provided in the manuscript or the manuscript references; otherwise, 'not applicable'.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Twitter NICHE@NICHE_Ulsterand NNEdPro@nnedpro
Contributors All the authors contributed to the design, analysis and development of the submitted manuscript. LF Lacey is the author responsible for the overall content of the data analysis and the derived results presented in the the submitted manuscript
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.