Article Text

Abstract
Objectives Intermittent fasting boosts some host defence mechanisms while modulating the inflammatory response. Lower-frequency fasting is associated with greater survival and lower risk from COVID-19-related comorbidities. This study evaluated associations of periodic fasting with COVID-19 severity and, secondarily, initial infection by SARS-CoV-2.
Design Prospective longitudinal observational cohort study.
Setting Single-centre secondary care facility in Salt Lake City, Utah, USA with follow-up across a 24-hospital integrated healthcare system.
Participants Patients enrolled in the INSPIRE registry in 2013–2020 were studied for the primary outcome if they tested positive for SARS-CoV-2 during March 2020 to February 2021 (n=205) or, for the secondary outcome, if they had any SARS-CoV-2 test result (n=1524).
Interventions No treatment assignments were made; individuals reported their personal history of routine periodic fasting across their life span.
Main outcome measures A composite of mortality or hospitalisation was the primary outcome and evaluated by Cox regression through February 2021 with multivariable analyses considering 36 covariables. The secondary outcome was whether a patient tested positive for SARS-CoV-2.
Results Subjects engaging in periodic fasting (n=73, 35.6%) did so for 40.4±20.6 years (max: 81.9 years) prior to COVID-19 diagnosis. The composite outcome occurred in 11.0% of periodic fasters and 28.8% of non-fasters (p=0.013), with HR=0.61 (95% CI 0.42 to 0.90) favouring fasting. Multivariable analyses confirmed this association. Other predictors of hospitalisation/mortality were age, Hispanic ethnicity, prior MI, prior TIA and renal failure, with trends for race, smoking, hyperlipidaemia, coronary disease, diabetes, heart failure and anxiety, but not alcohol use. In secondary analysis, COVID-19 was diagnosed in 14.3% of fasters and 13.0% of non-fasters (p=0.51).
Conclusions Routine periodic fasting was associated with a lower risk of hospitalisation or mortality in patients with COVID-19. Fasting may be a complementary therapy to vaccination that could provide immune support and hyperinflammation control during and beyond the pandemic.
Trial registration Clinicaltrials.gov, NCT02450006 (the INSPIRE registry).
- COVID-19
Data availability statement
Data are available upon reasonable request. The data underlying this article cannot be shared publicly due to US privacy laws. Data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
During a period of energy restriction, fasting controls inflammation by dampening the cytokine cascade, it enhances autophagy, and it switches the metabolic source of energy from glucose to fats, including by increasing circulating free fatty acids such as linoleic acid.
The SARS-CoV-2 receptor binding domains bind linoleic acid in pockets that, when bound, reduce spike protein affinity for ACE 2.
Repeated fasting boosts basal levels of some parameters related to inflammation control and host defence against infections, including galectin-3, and it ameliorates insulin resistance and cardiovascular risks such that periodic fasting is associated with greater survival and lower risk of heart failure, coronary artery disease and type 2 diabetes.
WHAT THIS STUDY ADDS
This observational longitudinal cohort study found that routine low-frequency periodic fasting for an average of >40 years was associated with a lower risk of COVID-19, measured as a composite of hospitalisation or mortality after COVID-19 diagnosis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Intermittent fasting should be further evaluated for potential short-term and long-term preventive or therapeutic use as a complementary approach to vaccines and antiviral therapies for reducing COVID-19 severity.
Introduction
Fasting modifies energy utilisation by consuming glucose and glycogen, inducing gluconeogenesis, and subsequently activating ketogenesis.1–3 In the switch to ketosis during fasting, circulating levels of fatty acids, including linoleic acid, increase.2 3 ,4 Intriguingly, linoleic acid tightly binds to the spike protein of SARS-CoV-2, the cause of COVID-19.5 The attachment of linoleic acid to the spike reduces the affinity of SARS-CoV-2 for ACE2.5 An acute rise in linoleic acid while a person is fasting, thus, provides a direct mechanism for fasting to acutely reduce the severity of COVID-19.
In terms of chronic protection from severe outcomes of infection, the multifaceted protein galectin-3 was increased, independent of weight change, by low-frequency intermittent fasting in the 6-month Weekly One-Day Water-only Fasting Interventional (WONDERFUL) Trial.6 Galectin-3 modulates inflammation with proinflammatory actions during acute infection and anti-inflammatory functions when infection resolves.7 It minimises risk from chronic metabolic disorders (eg, diabetes),8 and is elevated in patients with diabetes and heart failure (HF),9 perhaps as a protective mechanism to reduce risk (eg, the antidiabetes medication canagliflozin also increased galectin-310). Importantly, galectin-3 directly binds to a wide variety of pathogens,7 activates the innate immune system,7 impacts respiratory infections,11 increases expression of human genes encoding proteins with antiviral capacities12 and inhibits viral replication.12 Given the wide array of pathogens affected by galectin-3,7 it may also limit SARS-CoV-2 infection. The chronic increase of galectin-3 by intermittent fasting may,6 thus, provide a mechanistic link in which long-term participation in fasting could reduce COVID-19 severity.
Previously, routine periodic fasting was associated with lower risk of coronary artery disease (CAD),13 lower risk of type 2 diabetes,14 and—in patients with a >42-year history of fasting—improved longitudinal outcomes including greater survival and lower risk of incident HF.15 These associations may result from various mechanisms not related to weight loss.6 15–18 Such risk reductions by fasting of diagnoses that exacerbate the severity of COVID-19 (eg, diabetes, CAD and HF19 20) may indirectly reduce COVID-19 severity, providing a possible third biological mechanism for fasting-induced protection from severe COVID-19 outcomes.
Due to these direct and indirect impacts of fasting on infectious disease outcomes, it is hypothesised that periodic fasting is associated with lower COVID-19 severity in people infected by SARS-CoV-2. The primary objective of this study was to test whether periodic fasting is associated with the severe COVID-19 outcomes of hospitalisation and mortality after subjects were infected by SARS-CoV-2 and diagnosed with COVID-19. A secondary objective was to test whether periodic fasting predicts the onset of COVID-19.
Methods
Enrolment and ethics
This prospective observational cohort study evaluated patients who previously underwent cardiac catheterisation and completed a sociobehavioral survey regarding periodic fasting behaviour, education, income, marital status, exercise, work, race, ethnicity, alcohol intake and sleep behaviours. The survey was previously published.15
No subject was randomised in this study, but instead the long-term databasing and longitudinal surveillance of the INSPIRE (INtermountain Healthcare Biological Samples Collection Project and Investigational REgistry) registry were used. Subjects provided consent to participate and the INSPIRE registry collected clinical data, survey information, biological samples and longitudinal outcomes of patients seen at Intermountain Medical Centre in Salt Lake City, Utah, USA. INSPIRE is detailed at clinicaltrials.gov (NCT02450006). This study of periodic fasting and COVID-19 outcomes evaluated INSPIRE data.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of this research study.
Population
Subjects included consenting patients who enrolled in the INSPIRE registry from 2013 to 2020 and completed the INSPIRE survey. They were adult women and men unrestricted with respect to age, sex, race or ethnicity who underwent cardiac catheterisation due to cardiac symptoms or clinical evaluation needs. Of the 8634 patients enrolled in the INSPIRE registry between 7 February 2013 and 16 March 2020 (see figure 1 for a flow chart of included and excluded patients; see online supplemental table S1 for basic characteristics of patients not included in this study), 5795 patients (67.1%) completed the INSPIRE Survey and had registry demographics, cardiac risk factors, comorbidities, angiographic findings and prospective longitudinal outcomes available. That population was cross-referenced with patients who were tested at Intermountain for SARS-CoV-2 by PCR. Of the 5795 subjects, 1682 (29.0%) were tested for COVID-19 between 16 March 2020 and 25 February 2021, including 1457 who tested negative and 225 who tested positive.
Supplemental material
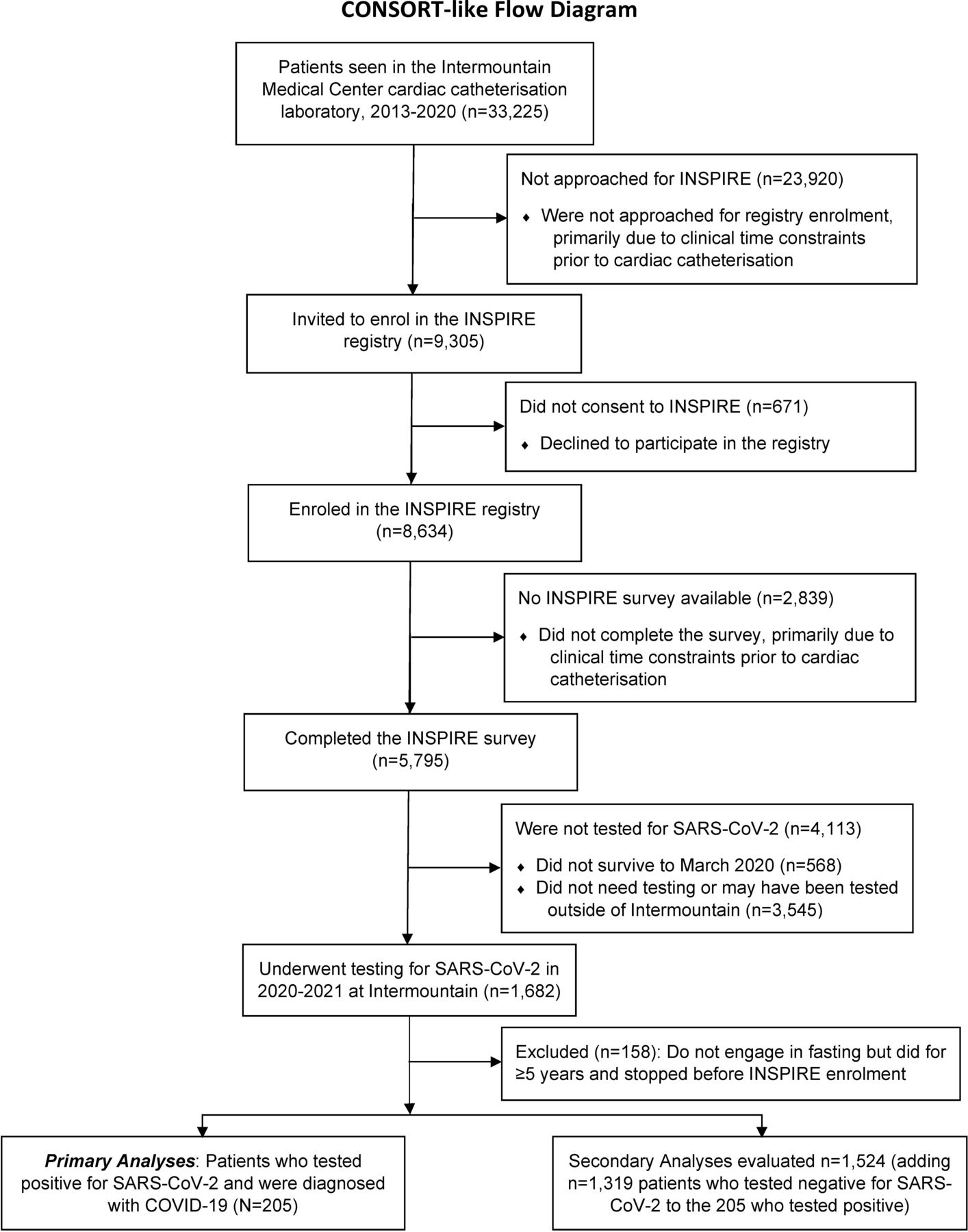
Enrolment and selection of individuals for this study. CONSORT, Consolidated Standards of Reporting Trials.
Study variables
Periodic fasting was defined based on two survey questions that inquired about whether patients engage in periodic fasting and, if they ever have, for how many years they engaged in routine fasting during their lifetime.15 Periodic fasting constituted routine fasting for 5 years or more, while not fasting included patients who never fasted routinely or who stopped their fasting routine prior to completing the survey. Patients who reported no periodic fasting but who had a prior history of fasting for ≥5 years (n=158) were excluded. Of the remaining 1524, n=205 tested positive for SARS-CoV-2 and constituted the primary study population, while n=1319 tested negative and were included only in secondary analyses. Generally, such periodic fasting occurs due to religious practices; in past studies 89%–92% of patients engaging in periodic fasting were members of the Church of Jesus Christ of Latter-day Saints (LDS, or Mormon) among whom fasting is often done once per month for about 24 hours.13 15 However, because in prior work ≈40% of LDS Church members reported that they engage in periodic fasting and religious preference did not confound the effect of fasting,13 15 and because the systematically shared health-related behaviours like not smoking and not drinking alcohol were measured in this study, religious preference per se was not evaluated here.
Data elements for race, ethnicity, income, education, marital status, employment status, physical exercise (eg, swimming, jogging, aerobics, football, tennis, gym workout), cycling, walking and alcohol use were also drawn from the INSPIRE Survey. Age, sex, body mass index, smoking (current or past), other cardiac risk factors, and comorbidities were extracted electronically from the INSPIRE database or the electronic health record at the time of COVID-19 diagnosis. Coronary anatomy was reported by the attending cardiologist from angiographic findings at the time of the INSPIRE Survey.
Outcomes
Study end points of all-cause mortality and hospitalisation for COVID-19 were evaluated as a single composite end point, with the time to hospitalisation used in the event that both outcomes occurred. Mortal status was obtained from the Social Security death master file, Utah death certificates and Intermountain electronic health records, which allowed for complete follow-up for mortality. Hospitalisation for COVID-19 was queried electronically from encounters in the Intermountain electronic data warehouse that provides a centralised database of all hospitalisation information for the 24 Intermountain hospitals in Utah and south-eastern Idaho. Because Intermountain provides the healthcare services to approximately two-thirds of people in that catchment region, >90% of hospitalisation events are captured by this method (and the small proportion of patients who may visit a hospital external to the integrated health system likely do not do so due to periodic fasting status).15 Mortality and hospitalisation outcomes were followed to 25 February 2021.
Statistical analysis
Baseline characteristics were evaluated between subjects who reported periodic fasting behaviour and those who reported being non-fasters, with statistical tests comparing differences by the Student’s t-test or the χ2 test, as appropriate. Statistical analyses were conducted with SPSS V.26.0 (IBM SPSS, Armonk, New York, USA). Statistical significance was defined as values of p≤0.05.
Cox regression was used to compute HRs and 95% CIs for the association of periodic fasting with the composite hospitalisation/mortality end point. The Wald approximation to the χ2 test was used to assess statistical significance in survival analyses. Kaplan-Meier survival curves were also drawn to graphically demonstrate the survival associations.
Multivariable Cox modelling evaluated periodic fasting with adjustments for 36 covariables (see table 1 for all covariables). Cox regressions were performed for each covariable and bivariable models entered periodic fasting with a single covariable. Because of the number of hospitalisation and mortality events observed (46 events), Cox analyses were limited to a maximum of four variables per model. Variables with three or four variables entered periodic fasting and age along with one or two others to assess significance and confounding. A confounding effect of a covariable was defined as a change of >10% of the β-coefficient of periodic fasting in Cox regression.
Baseline characteristics of patients who were diagnosed with COVID-19
Results
Baseline characteristics of n=205 patients diagnosed with COVID-19 are presented in table 1 (see below for details of the 1524 tested for COVID-19). Subjects engaging in periodic fasting (35.6%) did so for 40.4±20.6 years (max: 81.9 years), with 36.7±20.4 of those years being prior to enrolment in the INSPIRE registry and 3.7±2.9 years being between enrolment and when the subjects tested positive for SARS-CoV-2.
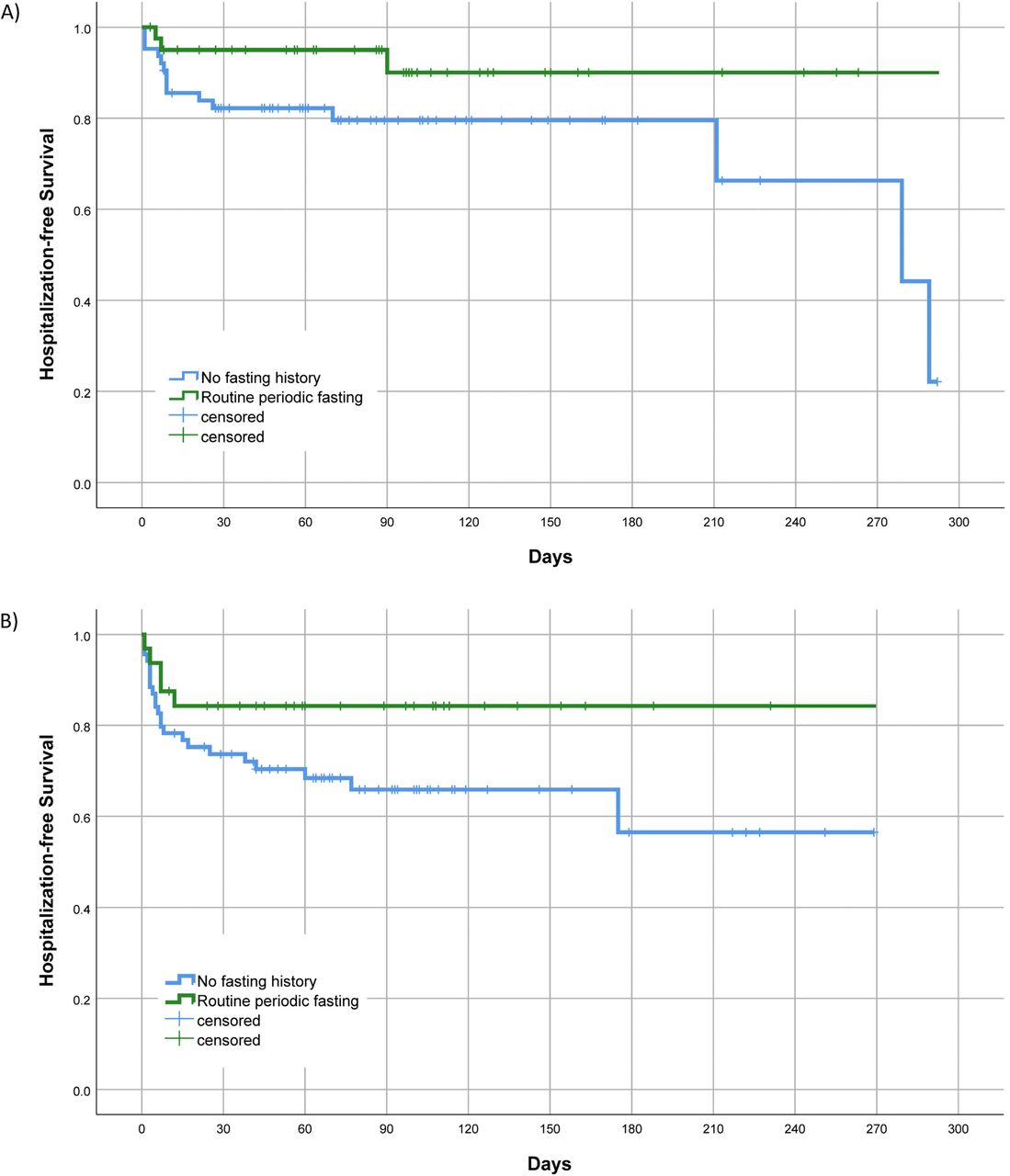
In the n=205 patients with COVID-19, 11.0% of fasters and 28.8% of non-fasters had hospitalisation/mortality (figure 2). This constituted a total of 46 composite study events, or 40 hospitalisations without death, 4 hospitalisations ending in death and 2 deaths without hospitalisation. The association of periodic fasting with the composite end point had HR=0.61 (CI 0.42 to 0.90; p=0.013). Fasting remained significant in all multivariable analyses (table 2), with a range of HR=0.61–0.65 depending on the covariables that were entered (p=0.015–0.036). Results for periodic fasting were similar in subjects <65 years (figure 3A) and ≥65 years of age (figure 3B), although splitting the population into the two subgroups (n=104 and n=101, respectively) reduced the statistical significance in both age groups.

Kaplan-Meier survival curves showing the differential hospitalisation/mortality events of patients diagnosed with COVID-19 who routinely engaged in periodic fasting compared with those who did not engage in fasting (p=0.013, n=205).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves for hospitalisation/mortality of patients diagnosed with COVID-19 who engaged in periodic fasting compared with patients who did not, in strata defined by: (A) Age <65 years (p=0.07, n=104) and (B) Age ≥65 years (p=0.09, n=101).
HRs and 95% CIs for the association of periodic fasting with lower risk of hospitalisation/mortality in patients who were diagnosed with COVID-19
Covariables that were associated with the composite outcome in models that also entered periodic fasting included: age (HR=1.32 per decade, p=0.009; or, compared with age decade 40–49, age 70–79: HR=3.05, p=0.09, and age 80+: HR=3.79, p=0.043), Hispanic ethnicity (HR=3.31, p=0.023), hyperlipidaemia (HR=3.88, p=0.024) or smoking (HR=1.89, p=0.046). Comorbidities also predicted hospitalisation or mortality in two-variable models entering periodic fasting and one of these: history of CAD (HR=4.11, p=0.007), myocardial infarction (MI) history (HR=2.28, p=0.009), HF history (HR=1.90, p=0.050), diabetes history (HR=1.83, p=0.048), transient ischemic attack (TIA) history (HR=2.79, p=0.002) or renal failure history (HR=5.03, p=0.008). These covariable associations became less significant when age was added to models, with most of the covariables listed above having p>0.05 in three-variable models that also entered age and periodic fasting. In four-variable models entering periodic fasting, age, Hispanic ethnicity and one comorbidity, the only comorbidities retaining significance at p≤0.05 were MI history, TIA history and renal failure history (see table 2 footnotes for further information).
For the secondary analysis of positive (indicating infection by SARS-CoV-2) versus negative test results, the n=205 COVID-19-positive patients focused on in this paper were evaluated along with n=1319 patients who tested negative and had INSPIRE survey and other study data available. For the baseline characteristics of these patients, see online supplemental table S2. In this expanded population, subjects who routinely engaged in periodic fasting had a similar frequency (p=0.51) of positive test results (14.3% positive, or 73 of 512 subjects who engaged in periodic fasting) compared with subjects who were non-fasters (13.0% positive for SARS-CoV-2, or 132 of 1012 non-fasting subjects).
Discussion
In patients who previously enrolled in the INSPIRE registry and subsequently tested positive for SARS-CoV-2 in 2020 or early 2021 prior to widespread vaccination, subjects who reported engaging in routine periodic fasting for an average of >40 years had a lower risk of hospitalisation or mortality after COVID-19 onset. This result was found in younger and older individuals, was present regardless of race or ethnicity, and did not depend on other cardiac risk factors, comorbidities or behaviours. Periodic fasting did not, however, predict whether or not a subject would be infected by SARS-CoV-2.
The degree to which COVID-19 resulted in hospitalisation and mortality throughout the world varied substantially during the pandemic. This is due to many health, medical, biological and healthcare issues, as well as social and political challenges, that resulted in a complex patchwork of differences in risk of hospitalisation and mortality across populations. Some of the factors involved in that variation include a population’s age distribution, its racial and ethnic composition, cardiovascular risk factor prevalences, and the distribution of comorbidities.19 20 Various mitigating factors specific to populations may also have lowered the severity of COVID-19.
Prior to SARS-CoV-2 vaccines, Utah and Alaska were the only US states with a COVID-19 case fatality rate <1% (both were ≈0.5%).21 Alaska has the 49th largest state population and before December 2021 had ≈47th highest number of COVID-19 cases.21 Its low case fatality could be anticipated because it is a geographical isolate to which COVID-19 arrived relatively late. Alaska’s public health officials had time to prepare and execute an aggressive mitigation programme that delayed widespread infection. Further, Alaska has the lowest number of nursing home beds in the USA (at ≈700 beds, vs Utah’s ≈8500 beds).22 Utah has the 30th largest state population and before December 2021 had ≈28th highest case count,21 and shares some characteristics with Alaska that are relevant to COVID-19 severity: Utah has the lowest median age in the USA (Alaska has the second lowest) and is ranked as the state with the fourth lowest rate of coronary heart disease (Alaska is ranked eighth lowest).23 A low case fatality rate in Utah could also have occurred because the state has the lowest smoking rate in the USA, has a limited racial/ethnic diversity (39th highest proportion of minorities), and had various healthcare system efforts that may have limited the severity of cases. Finally, Utah has the lowest per capita ethanol consumption in the USA that may have limited the spread of COVID-19 at bars and other social locales, but a connection of alcohol to COVID-19 severity is unconfirmed.
Given those characteristics of the Utah population, when survival analyses adjusted here for age, smoking, alcohol, race, ethnicity, CAD history, MI history, HF history and other factors, periodic fasting remained an independent predictor of a lower risk of hospitalisation or mortality. Because >60% of Utah residents are members of the LDS Church, routine periodic fasting is a common practice in the state. In this and previous studies at Intermountain, 27%–36% of all patients reported routinely engaging in periodic fasting,13–15 and had done so for more than four decades on average (with age averaging >60 years).15 Although these data suggest that only about a third of the Utah population engages routinely in periodic fasting, this is substantially higher than in other US states and may have contributed to the low COVID-19 case fatality rate for the state.
Periodic fasting was previously reported to be associated with lower mortality and lower HF incidence in a cohort of almost 2000 patients.15 A trend towards lower MI incidence was also found in that study.15 Further, periodic fasting was associated with a lower risk of CAD and a lower risk of diabetes in cross-sectional studies.13 14 In the present study, in addition to the association of periodic fasting with a lower risk of hospitalisation or mortality, various factors including many comorbidities were associated with a greater risk of hospitalisation or mortality. These findings support published predictors of COVID-19 severity,19 20 and extend the list by adding routine fasting as a predictor of lower COVID-19 severity.
Previously in a study of 24-hour water-only intermittent fasting, fatty acids including linoleic acid were increased during fasting.4 Linoleic acid locks the spike protein of SARS-CoV-2 in a conformation that is not conducive to the effective binding to ACE2.5 Elevated linoleic acid during fasting may, thus, lessen the number of infected cells or the number of SARS-CoV-2 virions in cells and thereby decrease the severity of COVID-19. Ketogenic diets that cause a switch of energy source from glucose to fatty acids/ketones should also provide this benefit. This provides one mechanism in which fasting may directly enhance immune function related to COVID-19 mitigation, while other more general immune-related mechanisms exist.
A loss of appetite is a typical response to infection, which may indicate that the human body has intrinsic mechanisms for initiating fasting in order to activate the immune system, as proposed by an animal study.24 While that finding requires testing in humans, other evidence supports the activation of general immune responses and autophagy by fasting.25 26 Interestingly, small human studies reveal that intermittent fasting blunts CD4+ T cell responsiveness during fasting by upregulating insulin-like growth factor binding protein 1 and FOXO4/FK506-binding protein 5,27 28 and that fasting generally suppresses the production of proinflammatory cytokines.25 Often in severe COVID-19 the human immune system over-reacts to SARS-CoV-2 infection and the consequent hyperinflammation can result in respiratory failure.29 Fasting during an active infection could, thus, bolster the immune response through pathways not involved in the standard inflammatory response to infection while minimising severe inflammatory outbursts. It may also counteract the inhibition of autophagy that is caused by SARS-CoV-2.30 31 Immunomodulation by fasting and its effects on autophagy with respect to COVID-19 require further study.
Very frequent intermittent fasting such as alternate-day fasting or uninterrupted multiple-day fasting is challenging. Even lower frequency or shorter duration fasting (eg, 16-hour time-restricted eating18 or 24-hour once-per-week fasting32) over a long period of time (ie, years/decades) may prevent chronic disease onset or reduce the severity of existing chronic diseases13–15 and, thus, prepare the body to prevent severe COVID-19 outcomes.26 This may occur as fasting prevents or treats morbidities13–15 32 33 that increase the risk of severe COVID-19 outcomes, such as CAD, MI, HF and diabetes.19 20 A variety of mechanisms may be involved in the long-term prevention and treatment of those diseases (which mechanisms are beyond the scope of this study),4 6 16–18 26 30–37 and, as a preventive health practice, periodic fasting may indirectly prevent severe COVID-19 by its long-term impacts on those disease mechanisms and comorbidities.25 26 38
Finally, a periodic fasting lifestyle may condition the body by elevating basal levels of key physiological parameters in preparation for insults such as infection. A randomised human study of low-frequency (once-per-week) 24-hour water-only intermittent fasting showed that fasting increased basal galectin-3 level over a moderate term (6 months).6 Galectin-3 is integrally involved in host defence to infectious diseases.7 11 12 Further, galectin-3 stimulates anti-inflammatory effects by modulating nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and the NLR family pyrin domain containing 3 (NLRP3) inflammasome,8 which should inhibit the hyperinflammation associated with COVID-19. The routine practice of once-per-month fasting for >40 years that is reported here is lower-frequency fasting over a longer term and may have conditioned the body by elevating basal galectin-3 and optimising basal levels of other factors that aided in preventing severe complications of COVID-19. Further study is needed of how fasting may impact the human immune system.
This study is potentially limited by the observational nature in which subjects engaging in periodic fasting were not randomised to the behaviour. Incomplete adjustment for important confounders or failure to measure some confounders may have limited the ability to correctly assign risk to the variables under study. However, 36 covariables were evaluated and none of them substantially modified the association of periodic fasting with hospitalisation/mortality, including smoking and others that may share some covariation with periodic fasting in the study population. The enrolment of study participants at the time of angiography may have introduced selection biases that further limit the study; figure 1 and online supplemental table S1 provide information about enrolment characteristics.
Fasting history was self-reported after years of participation in the practice, which may have caused data to be imprecise due to recall bias; however, the vast majority of people who report fasting also report membership in the LDS Church (89%–92% in past evaluations13 15) and fast routinely for religious purposes, thus the average definition of periodic fasting here is a 24-hour fast once per month that was followed consistently for an average of 40.4 years (see Results). More than 60% of Utahns identify as members of the LDS Church; however, since fewer than half of LDS Church members report that they engage in periodic fasting,13 15 many of the other factors that may be systematically shared in the Utah population (eg, not smoking, not drinking alcohol, being married) were shared by both those who engaged in fasting and those who did not. Consequently, confounding from systematically shared religion-related characteristics is less of an issue for this study than may be commonly assumed. Additionally, adjustment for variables such as smoking, alcohol use, marital status and other factors corrected for shared health-related characteristics that could confound the association of periodic fasting with study outcomes.
The case fatality rate in the USA was around 3% prior to the advent of SARS-CoV-2 vaccines,21 and this study’s mortality rate was similar: 6 of 205 subjects (2.93%) died. This partly reflects that this population was a higher-risk group than the general population due to the prevalence of morbidities, older age and existence of cardiovascular conditions requiring medical care. Thus, the findings of this study may not generalise to the overall population and interpretation should be made with caution. Unfortunately, no data on common side effects of fasting such as muscle loss were available here and such potential side effects should be considered in future studies. As with all medical interventions, assessment of the risks and not just the benefits of intermittent fasting should be made when considering its use for health purposes, including for people with chronic diseases.39
Conclusions
Routine periodic fasting was associated with a lower risk of hospitalisation or mortality in patients with COVID-19. While fasting is not a panacea or a quick fix for health problems, low-frequency fasting improves cardiometabolic health even without significant weight loss,18 32 and multiple biological mechanisms4–8 11 12 24–28 30 31 33 and epidemiological results13–15 19 20 support the idea that consistent fasting may limit COVID-19 severity. Fasting may do so via acute but temporary physiological changes during energy deprivation and by persistent modification of basal physiological norms and reduction of chronic disease risks across repeated fasting episodes. The primary mechanisms may include hyperinflammation control and strengthening of some immunity pathways.
Sustainable intermittent fasting regimens deserve further investigation for potential short-term and long-term preventive or therapeutic use as a complementary therapy to vaccines to reduce COVID-19 severity, both during the pandemic and postpandemic since repeat vaccinations cannot be performed every few months indefinitely for the entire world and vaccine access is limited in many nations. Investigations of the effect of fasting on long COVID-19 should be included in new studies that are conducted.
Data availability statement
Data are available upon reasonable request. The data underlying this article cannot be shared publicly due to US privacy laws. Data are available upon reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Intermountain Healthcare Institutional Review Board. The INSPIRE registry was approved as IRB number 1024811 and the present study of periodic fasting in the INSPIRE registry as IRB number 1051223. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrBenjaminHorne
Contributors BDH as guarantor accepts full responsibility for the work and the conduct of the study, had full access to all study data, and controlled the decision to publish. Conception and design: BDH, JBM, JLA; acquisition, analysis, or interpretation of data: BDH, JBM, HTM, VTL, TLB, KUK, JLA; drafting of the manuscript: BDH, JLA; critical revision for important intellectual content: JBM, HTM, TLB, VTL, KUK; final approval of the submitted manuscript: BDH, JBM, HTM, TLB, VTL, KUK, JLA; agreement to be accountable for all aspects of the work: BDH, JBM, HTM, TLB, VTL, KUK, JLA. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This research was funded by a grant from the Intermountain Research and Medical Foundation through the philanthropy of the Dell Loy Hansen Heart Foundation (PI: BDH; grant #614).
Disclaimer The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: funding from the Intermountain Research and Medical Foundation through the philanthropy of the Dell Loy Hansen Heart Foundation for the submitted work; BDH has also received other research grants from the Intermountain Research and Medical Foundation for other fasting-related studies, but the authors have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; BDH is a member of the scientific advisory boards of Opsis Health and Lab Me Analytics outside of the submitted work; BDH received a grant from AstraZeneca for prepandemic clinical risk prediction in percutaneous coronary intervention outside the submitted work, and BDH, HTM and JLA are inventors of clinical decision tools that are licensed to CareCentra and Alluceo.
Provenance and peer review Not commissioned; externally peer reviewed by Mohamed Allaf, United Kingdom of Great Britain and Northern Ireland.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.