Article Text

Abstract
Objective To investigate factors associated with COVID-19 severity in ambulatory individuals with type 2 diabetes mellitus (T2DM) and obesity treated with a medically supervised ketogenic diet (MSKD).
Research design and methods In this real-world, retrospective, exploratory analysis, multivariate modelling was used to assess clinical factors associated with hospitalisation for COVID-19 in a geographically diverse outpatient population with T2DM treated virtually.
Results Leading up to COVID-19 onset, non-hospitalised patients had higher average ketones (0.64 vs 0.52 mmol/L; p=0.016) and greater weight loss (6.8% vs 4.2%; p=0.009) compared with those hospitalised. Greater weight loss was significantly associated with lower likelihood of hospitalisation (adjusted OR=0.91, p=0.005), controlling for enrolment demographics and medical characteristics.
Conclusions Therapies such as MSKD, which elicit rapid, significant weight loss, may favourably impact COVID-19 hospitalisation rate and severity in individuals with T2DM and obesity.
- COVID-19
- Nutritional treatment
- Diabetes mellitus
- Weight management
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Type 2 diabetes and obesity are independent risk factors for severe COVID-19 infection and death.
WHAT THIS STUDY ADDS
Patients not hospitalised had higher mean ketones during treatment with a medically supervised ketogenic diet and achieved greater weight loss at the time of COVID-19 diagnosis.
Greater weight loss in those with type 2 diabetes and obesity is associated with lower odds of hospitalisation in those diagnosed with COVID-19.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
Therapies such as a medically supervised weight loss treatment which elicit rapid, significant weight loss may be a useful tool for individuals with type 2 diabetes mellitus and obesity to reduce risk of COVID-19-related hospitalisation.
Introduction
Type 2 diabetes mellitus (T2DM)1 2 and obesity3 are independent, non-additive4 risk factors for severe COVID-19 infection and death. A medically supervised ketogenic diet (MSKD), together with continuous remote care, can quickly reduce glycaemia and weight in those with T2DM.5 A ketogenic diet shows promise in reducing the severity of and risk of death from COVID-19, as demonstrated in a retrospective inpatient hospital study.6
However, the impact of a ketogenic diet and its clinical effects on COVID-19 severity in an ambulatory population are unknown. Thus, we explored factors associated with COVID-19 severity in patients with T2DM in a US-based, geographically diverse, outpatient, remote care clinic delivering an MSKD for T2DM treatment.
Research design and methods
This real-world, retrospective, exploratory analysis assessed the COVID-19 severity of those who reported that diagnosis among the T2DM outpatient population treated at Virta Health. Patients in our telemedicine clinic are treated with an MSKD and supported by a care team of health coaches and licensed medical providers through a continuous remote care platform. We guide patients to restrict carbohydrate intake to sustain nutritional ketosis as assessed by blood beta-hydroxybutyrate. Nutrition recommendations are individualised, though this typically means less than 50 g of carbohydrates daily. Dietary fats are encouraged to be consumed to satiety.
Initial guidance for protein intake is calculated using 1.5 g/kg of reference body weight (ie, medium-frame ‘ideal’ and gender-specific) using the Metropolitan Life Insurance ‘Ideal Body Weight’ tables7 with adjustments made ad hoc based on factors such as activity level and biomarker responses. Our previous study demonstrated that these recommended targets were sufficient in limiting lean mass loss compared with other weight loss interventions,8 pointing to the adequacy of these recommendations. While patients are not required to report dietary intake, these recommendations generally result in 5%–10% of energy as carbohydrates, 15%–20% protein and 70%–75% fat.
Patient-reported clinical events are recorded in medical records and monitored in ongoing safety evaluations. Patients who reported a COVID-19 diagnosis were asked for additional information regarding symptoms, severity, and treatment via questionnaire as part of a quality improvement initiative and recorded in medical records. De-identified data obtained from medical records of patients with T2DM who reported a COVID-19 diagnosis between 1 March 2020 and 9 May 2021 were included. Prevalence of hospitalisation, treatment with supplemental oxygen or ventilation, and death were assessed from patient or emergency contact report.
We assessed differences in demographics (age, gender), enrolment characteristics (hemoglobin A1c (HbA1c), weight and body mass index (BMI)), and clinical markers during treatment (mean blood glucose, mean blood ketones and weight change) between patients with COVID-19 diagnosis who were and were not hospitalised. Χ2 tests were used to compare group distributions for categorical variables. Welch independent samples t-tests were used for continuous variables given unequal sample sizes. Multivariate logistic regression was used to assess associations with hospitalisation, controlling for demographics, enrolment characteristics, days in treatment and clinical markers during treatment. To assess survey response bias, demographics, enrolment characteristics, and clinical markers during treatment were compared between survey responders and non-responders.
Results
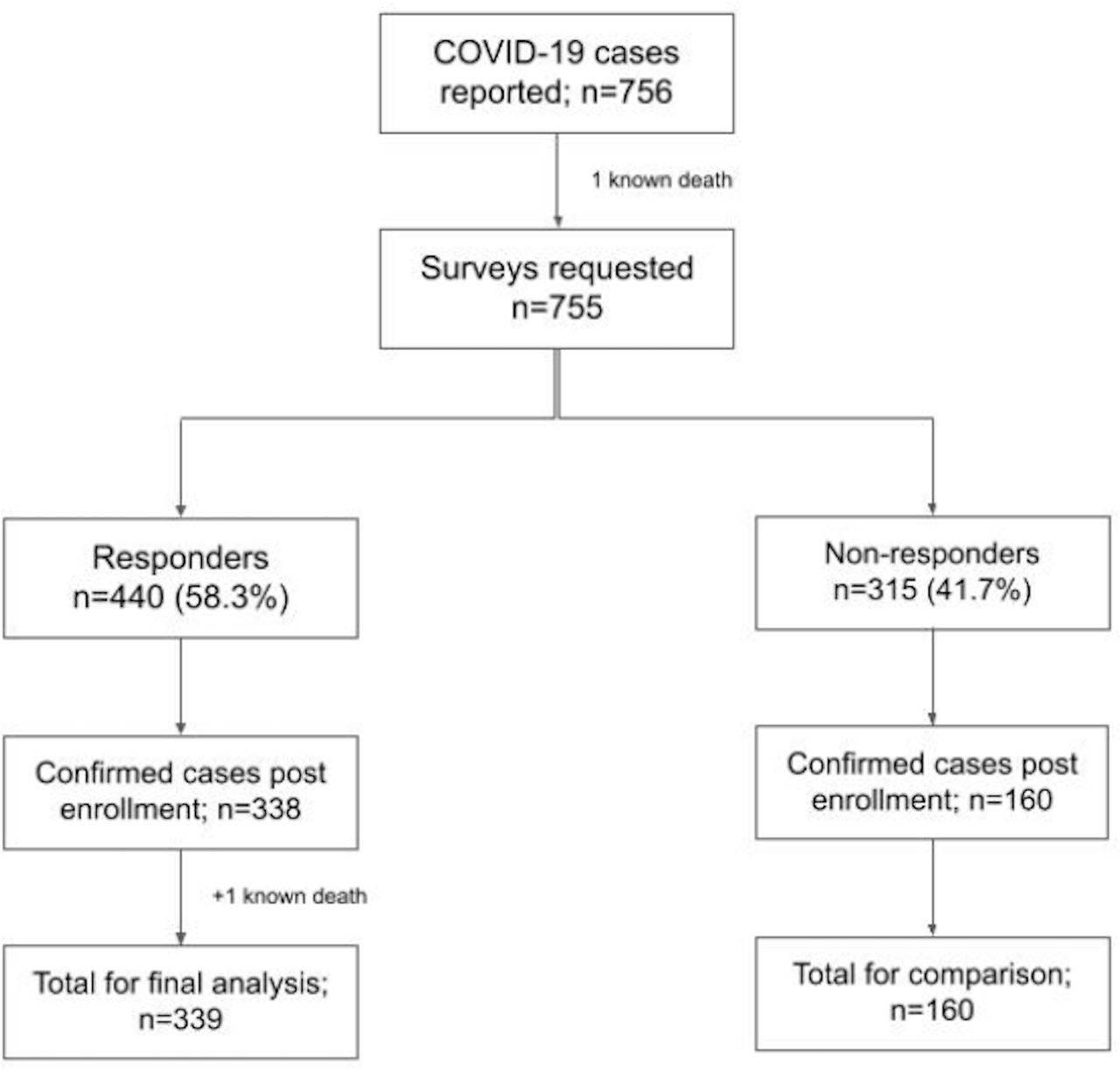
A COVID-19 diagnosis was reported by 756 patients with T2DM; 600 (79.3%) had a known COVID-19 event date and 440 (58.3% of total; 73.3% of those with known dates) responded to medical providers’ questionnaires regarding COVID-19 severity and treatment (figure 1). Patients who received a COVID-19 diagnosis prior to beginning an MSKD (n=102) were excluded from this analysis. Outcomes were assessed among individuals who received a COVID-19 diagnosis after initiation of an MSKD and responded to the survey plus one individual with a known COVID-19-related death (n=339). Patients were 54.9±8.7 years of age with a BMI of 34.8±6.8 kg/m2 at the time of COVID-19 diagnosis, 50% female and from 44 US states.
{kind=link}
Reported COVID-19 cases (n=756) and severity surveys eligible for analysis in patients with type 2 diabetes (n=339). Final analysis=analysis comparing those hospitalised versus non-hospitalised; comparison=analysis comparing characteristics of responders versus non-responders; eligible for final analysis=returned surveys with a corresponding known COVID-19 event date post-initiation of MSKD. MSKD, medically supervised ketogenic diet.
Hospitalisation, supplemental oxygen use, ventilation, and death were reported by 38 (11.2%), 34 (10%), 6 (1.8%), and 1 (0.29%) patients, respectively. Symptoms reported by more than 70% of the patients included fatigue, headache, muscle/joint pain and fever/chills. Ongoing health issues were reported in 38.9% of patients, who commonly reported fatigue, shortness of breath, headache and brain fog.
There were no differences in demographics or enrolment characteristics between hospitalised and non-hospitalised patients. Patients not hospitalised had higher mean ketones during treatment with MSKD and achieved greater weight loss at the time of COVID-19 diagnosis (table 1). In a multivariate logistic regression, greater weight loss was significantly associated with lower likelihood of hospitalisation (adjusted OR=0.91, p=0.005), controlling for age, gender, enrolment weight and HbA1c, and days since MSKD initiation (table 2). The relationship between mean ketones and hospitalisation in a separate model controlling for the same factors was not significant (p=0.192).
Characteristics of patients with type 2 diabetes by hospitalisation status following COVID-19 diagnosis
Multivariate logistic regression of factors associated with hospitalisation in patients with type 2 diabetes and a COVID-19 diagnosis
No differences in age, time in treatment (days on MSKD), enrolment HbA1c or weight, or mean blood glucose levels during treatment with MSKD were detected between survey responders and non-responders with a known COVID-19 diagnosis date after MSKD initiation (n=160). However, responders had a higher enrolment BMI compared with non-responders (37.4±7.5 vs 35.8±6.6 kg/m2; p=0.028), and non-responders had less weight loss (5.3±5.7 vs 6.6±6.4%; p=0.034), lower mean ketones (0.55±0.3 vs 0.62±0.4 mmol/L; p=0.022) and less ketone logging (0.66±0.4 vs 0.79±0.4 values/week; p<0.001).
Conclusions
In a geographically diverse outpatient telemedicine clinic patient population with T2DM and obesity, only 11% of patients who reported a COVID-19 diagnosis required hospitalisation. Fewer were treated with supplemental oxygen and ventilation, and only one death (0.3% of diagnosed) due to COVID-19 was reported. No baseline differences were noted between those requiring hospitalisation and those who did not. During treatment and prior to developing COVID-19, non-hospitalised patients had higher mean ketones and greater percentage weight loss in univariate analyses. Greater weight loss was associated with lower likelihood of hospitalisation after controlling for demographics and clinical markers.
The observed incidence of COVID-19-related hospitalisation and death among ambulatory patients with T2DM in our clinic was low relative to other reports. A regional medical system reported COVID-19 hospitalisation and death rates of 44% and 5%, respectively, among ambulatory patients with T2DM.1 In patients with T2DM hospitalised with COVID-19, over 20% mortality has been observed within 4 weeks of admission.9 Beyond demographic and geographical diversity, our population may differ from other healthcare systems in that patients proactively chose to engage in a digital intervention and many had already experienced metabolic improvements. Additionally, existing access to telemedicine and the ability to maintain ongoing care and monitor metabolic health markers from home may have contributed to lower observed severity rates in our population.
Among our patients, greater per cent weight loss was associated with lower likelihood of hospitalisation. A recent retrospective, matched cohort study similarly observed that in people with or without type 2 diabetes, prior substantial weight loss (20.8%) resulting from surgery was associated with a 49% lower risk of hospitalisation relative to a control group who lost only 2.3% body weight on average.10 This suggests that clinically significant weight loss achieved through a variety of interventions may improve COVID-19 outcomes. Past research on MSKD demonstrated weight loss concurrent with significant reductions in inflammatory cytokines over 2 years.11 COVID-19 mortality is highly correlated with the severity of the inflammation-related cytokine storm and presence of multiple comorbidities, including diabetes and obesity, which increase one’s risk of developing severe infection.12 Weight loss, and perhaps associated reductions in inflammation, may play a critical role.6
Ketones are also known to be potent modulators of inflammation.13 However, in a multivariate logistic regression, greater weight loss, but not ketones, was significantly associated with lower likelihood of hospitalisation, controlling for age, gender, enrolment weight and HbA1c, and days since MSKD initiation. Higher mean ketones were present in non-hospitalised patients, and in past research, ketones have been associated with greater per cent weight loss.14
Mean glucose during treatment with MSKD was not associated with hospitalisation. Although high glucose on hospital admission15 16 and during infection16 has been associated with poor prognosis, no relationship between HbA1c and mortality has been observed.17 Taken together, this suggests longer term glycaemic control may play a lesser role in risk of severe disease, while glycaemic control during infection may be a modifiable risk factor worthy of attention.
Limitations of this analysis include self-reported events and total unreturned surveys (41.7% of total; 26.7% of known COVID-19 dates). Survey non-responders displayed features of lower healthcare engagement as seen by less weight loss, lower mean ketones and lower logging frequency, demonstrating a potential bias toward patients with greater health improvement. However, given that patients reported the diagnosis of COVID-19 and remained engaged with their care team, it is less likely they suffered severe cases resulting in hospitalisation and death without reporting.
Patients included in this analysis were not asked to complete any tasks not already part of their care in the Virta Clinic. Since food tracking is not a required component of the treatment, dietary information was not reported and therefore, details regarding micronutrient intake are unavailable. Though we recognise that specific micronutrients such as zinc, vitamin C, vitamin D, vitamin A and others18 19 can play a significant role in disease severity including hospitalisation, we were unable to analyse their potential influence and interaction on our outcomes.
Additionally, due to the nature of the study design, a real-world retrospective analysis of patients enrolled in the Virta Clinic and its treatment, there was no control group available for comparison with our results. Future analyses could compare these results with those of a group not following an MSKD to explore diet-specific influences on the likelihood of hospitalisation in those diagnosed with COVID-19.
Our results demonstrate that therapies such as MSKD, which elicit rapid, significant weight loss, may favourably impact hospitalisation rate and severity of COVID-19 in patients with T2DM. In addition to vaccination and following public health recommendations, an MSKD may be an effective preventive strategy to mitigate the severity of future COVID-19 in individuals with T2DM and obesity.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to acknowledge the Virta Health care team and support team members for their dedication in treating and monitoring our patients. Thank you to Dr. Robert Ratner for project oversight and input.
References
Footnotes
Presented at Research previously presented at ADA’s 81st annual meeting. 40-LB—2021 ADA. COVID-19 Severity in a Geographically Diverse, U.S.-based, Ambulatory Population with Type 2 Diabetes on a Medically Supervised Ketogenic Diet.
Contributors BMV contributed to study design, conducted the study, interpreted data, drafted the manuscript and edited the draft. CGPR contributed to study design, interpreted the data and edited the draft. MVT carried out statistical analyses, interpreted results and edited the draft. MPG contributed to the study design and analysis plan, conducted the analyses and interpreted the data. RNA and SJA interpreted the data and edited the draft. ALM contributed to the study design and analysis plan, interpreted the data and edited the draft. All authors revised and provided final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BMV, CGPR, MVT, RNA, SJA and ALM are employed by Virta Health and offered stock options. MPG served on advisory boards with United Therapeutics, Altavant and Bayer; has been a speaker in pulmonary hypertension for Bayer, Janssen and United Therapeutics; and received grant funding from Janssen.
Provenance and peer review Not commissioned; externally peer reviewed.