Article Text

Abstract
This study explored the prevalence of low serum vitamin D in patients admitted with acute respiratory tract infections (ARTIs) such as COVID-19. This study investigated whether patients with COVID-19 had lower serum vitamin D compared with patients with ARTIs of other aetiology. A case–control study was performed with cases of COVID-19 and controls of non-COVID-19 ARTIs. Patients were enrolled from a single general medical ward in a secondary care hospital between 15 April 2020 and 15 May 2020. Exclusion criteria were an oxygen requirement of >8 L/min. Data collected included serum 25-hydroxyvitamin D concentration, venous plasma glucose concentration and heamoglobin A1c. Outcomes measured were length of hospital stay, deaths, the need for high dependency and intensive care unit involvement. A total of 60 patients of five ethnic groups were enrolled, 85% (n=46) were of White-British ethnicity. The data analysis is based on these 46 patients of which 24 were non-COVID-19 patients with ARTI and 22 were patients with COVID-19. Overall, 80% of the study population had a serum vitamin D concentration below 50 nmol/L with median concentrations of 30 nmol/L and 35 nmol/L for patients with COVID-19 and non-COVID-19 ARTIs respectively. A Mann-Whitney sign-ranked test with respect to serum vitamin D concentration found no statistically significant difference between cases and controls, p=0.09. There was no significant difference in the length of stay, body mass index and rates of various comorbidities such as diabetes mellitus (DM), hypertension and lung disease in both study groups. However, DM was found to be associated with lower serum vitamin D concentrations. The results of this study support published literature showing an association between low serum vitamin D and ARTIs including COVID-19. However, this study did not identify patients with COVID-19 to have a statistically significant lower serum vitamin D concentration than non-COVID-19 patients with ARTI.
- COVID-19
- nutrient deficiencies
- pulmonary disease
Data availability statement
Data is available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A correlation between low serum vitamin D concentrations and acute respiratory tract infections including COVID-19 may exist.
WHAT THIS STUDY ADDS
This study demonstrates the significant prevalence of vitamin D deficiency and insufficiency among hospitalised patients.
This study identified both COVID-19 and acute respiratory tract infections are equally associated with low serum vitamin D concentrations.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights the requirement for further research into the effects of low serum vitamin D concentration on acute respiratory tract infections including COVID-19.
This study advocates the need to screen inpatients for vitamin D deficiency and insufficiency.
Introduction
SARS-CoV-2, a novel member of the coronavirus family, is the cause of the COVID-19.
SARS-CoV-2 represents one of seven coronaviruses known to infect humans, and the third virulent strain causing severe pneumonia and acute respiratory distress syndrome (ARDS).1–3
Infections with SARS-CoV-2 have produced a wide spectrum of phenotypes, ranging from asymptomatic individuals to mild symptoms such as fever, dry cough, myalgia, diarrhoea and anosmia, to more severe disease manifestations including hypoxaemia, pneumonia, ARDS, multiorgan failure and death.4
ARDS is a common cause of mortality and morbidity in patients with COVID-19. A cytokine storm driven by the virus has been implicated. Patients with the infection have shown the upregulation of inflammatory cytokines such as IL-6.5 Similarly, overactivation of proinflammatory Th17 cells and cytotoxic CD8 T cells have been observed.6 The subsequent astounding release of proinflammatory cytokines has the capability to induce systemic consequences such as shock and multiorgan failure.
In a similar manner to SARS-COV-1, SARS-CoV-2 is known to enter host cells via the cell surface receptor ACE 2 and reduce its expression in lung tissue.7 8
Experimental evidence from mice studies suggests that the manifestation of ARDS in relation to SARS COV-2 is partly due to a shift in the equilibrium away from ACE-2 and angiotensin 1–7 towards a predominance of ACE and angiotensin 2 resulting in more severe acute lung injury.9–11
Vitamin D3 (1,25(OH)2D3) is a fat-soluble secosteroid which typically participates in calcium homeostasis. Multiple studies have demonstrated an extraskeletal role of vitamin D in its interaction with the immune system and the renin-angiotensin-aldosterone system (RAAS).
Vitamin D receptor (VDR)-negative mice demonstrate elevated renin and angiotensin II production as well as more severe pulmonary oedema compared with wild-type mice following lipopolysaccharide aspiration.12 13
A multitude of adaptive and innate immune cells possess VDR. The exact immunoregulatory effects of vitamin D are often disease specific. The effects of vitamin D on cells of the innate immune system are largely stimulatory, resulting in enhanced phagocytoses and an amplified production of antimicrobial peptides.14 On the contrary, the effects of vitamin D on the adaptive immune system are characteristically inhibitory.15–18
It is proposed then that low serum vitamin D concentrations may exacerbate COVID-19, first by worsening the already displaced equilibrium of ACE and ACE-2, and second, through the disinhibition of the adaptive immune system.
The risk factors associated with low serum vitamin D concentration are many. A cross-sectional survey of 1828 middle aged Caucasian adults identified lower serum vitamin D concentrations in relation to obesity/underweight, female gender, reduced physical activity and reduced sun exposure.19 A meta-analysis of 23 studies also found that obesity was associated with a 35% increased prevalence of vitamin D deficiency when compared with normal body weight individuals.20 The biological mechanisms underpinning the associations between body mass index (BMI) and vitamin D deficiency are yet to be understood. It has been suggested that obesity may result in decreased serum concentrations of vitamin D secondary to decreased sun exposure and increased fat sequestration.21 22
A systematic review and meta-analysis of 17 observational studies consisting of 2756 patients identified an association between vitamin D deficiency and higher mortality, higher rates of hospital admission and prolonged inpatient stay in adults with COVID-19.23
Another meta-analysis of 26 observational studies consisting of 8176 patients with COVID-19 found that vitamin D deficiency did not increase the risk of developing COVID-19; however, severe cases of COVID-19 were associated with vitamin D deficiency.24
A limitation to both of these meta-analyses included the inability to independently assess the impacts of confounding variables such as gender, ethnicity, BMI, diabetes and advanced age, all of which are known risk factors for vitamin D deficiency and severe COVID-19 outcomes.23 24
Prior to COVID-19, vitamin D deficiency has been studied with particular interest in the context of acute respiratory tract infections (ARTIs). A 2017 individual participant data meta-analysis including 10 933 participants in 25 randomised control trials found an overall protective effect of vitamin D supplementation against ARTI, the greatest benefit being seen in those with severe vitamin D deficiency.25
These studies in combination with the biological plausibility reiterate the important immunomodulatory role of vitamin D in relation to ARTIs including COVID-19.
Aim
The aim of this study was to evaluate the vitamin D status of inpatients with COVID-19 and inpatients with non-COVID-19 ARTIs.
Method
Research design
Case–control study.
Participants
The demographic information for the participants included in the study are shown in table 1. Participants included a total of 60 inpatients from a single general medical ward at Medway Maritime Hospital, Gillingham, Kent, United Kingdom between 15 April 2020 and 15 May 2020.
Participant demographics
Exclusion criteria for admission to this particular ward included an oxygen requirement of over 8 L/min.
Procedure
Blood sampling and determination of serum vitamin D concentration
At admission participants had three blood samples taken: one serum separating tube, one fluoride oxalate tube and one potassium EDTA tube. These samples were processed for 25-hydroxyvitamin D, random venous plasma glucose and haemoglobin A1c (HbA1c).
25-hydroxyvitamin D was processed by UniCel DxI Immunoassay System using Beckman Access 25(OH) Vitamin D UniCel DxI Reagent Pack. Serum vitamin D concentration reference ranges used in this study are the National Institute for Health and Care Excellence (NICE) recommended ranges as follows: Less than 25 nmol/L is vitamin D deficiency, 25–50 nmol/L is vitamin D insufficiency and greater than 50 nmol/L is vitamin D sufficiency.26
Plasma glucose and HbA1C determination
Enzymatic UV testing was used for the quantitative determination of glucose in human plasma on a Beckman Coulter AU analyser (AU680) using Beckman reagents. The glucose method used was a hexokinase/glucose 6 phosphate dehydrogenase method. The quality of all glucose results was assured by the continued participation in the United Kingdom National External Quality Assessment Service (UK NEQAS). High-pressure liquid chromatography was performed for HbA1C measurement using TOSOH BioScience system.
COVID-19 status determination
On admission to hospital, nasopharyngeal and oropharyngeal swabs were processed for the detection of COVID-19 using real-time reverse transcription PCR amplification technology performed on VitaPCR Instrument.
Auxiliary patient information
Information was collected from general practice (GP) and hospital records regarding patient’s admission date, discharge date, comorbidities, BMI, medications and any intensive care/high dependency stay during the admission.
Data analysis
Data selection
Initially, 60 patients met the non-exclusion criteria. It was observed that 87% of the patients were of White British ethnicity. The rest of the ethnic groups consisted of Black British, Asian Indian, Black African and those for whom ethnicity was unrecorded. Due to the sparse and statistically unrepresentative numbers, these groups were excluded from further analysis. The sample subjected to statistical analysis included only the White British discharged patients.
Principal component analysis:
The whole data set of 60 patients and seven variables consisting of random plasma glucose concentration, HbA1c, age, weight, height, length of hospital stay and serum vitamin D concentration were initially examined with Principal Component Analysis (PCA).27 28 PCA is a multivariate data analysis technique which enables the reduction of high dimensional data into a set of uncorrelated principal components that provide further insights into relationships between variables. Recent applications of PCA in COVID-19 studies have been published.28 29 A projection of serum vitamin D concentration (nmol/L), length of hospital stay (days) and BMI (kg/m2) onto the principal components graphically provided insights regarding the pattern distribution of patients relative to their COVID-19 status. Further information is provided in online supplemental material
Supplemental material
Statistical analysis
With respect to the 46 discharged patients of White British ethnicity, normality tests by Kolmogorov-Smirnov (p=0.000), Lilliefors (p=0.023) and Anderson-Darling (p=0.007) showed that the data was not normally distributed. The Mann-Whitney sign-ranked test was used for ascertaining p values.
Graphical analysis
Graphical profiles were generated with respect to COVID-19 status; serum vitamin D concentration; length of stay; BMI; and comorbidities such as diabetes mellitus (DM), hypertension (HTN) and lung disease (LD).
PCA and statistical analysis were performed in Matlab.30 Tabulations and visualisations were performed in Microsoft Excel and Tableau software.31 32
Results
Comorbidities
Table 2 shows that the comorbidities among both cohorts were of similar frequency. The total number of comorbidities exceeds the total number of patients highlighting that some patients had more than one comorbidity.
Frequency of comorbidities in the patient cohorts
Vitamin D analysis
Table 3 highlights the degree of vitamin D insufficiency and deficiency seen in the entire hospitalised patient cohort. Irrespective of COVID-19 status, 80% (N=37) of the entire cohort had low serum vitamin D concentrations (<50 nmol/L) with 39% (N=18) having vitamin D deficiency.
COVID-19 positive and negative cohorts with regards to serum vitamin D concentration and length of inpatient stay
The median vitamin D concentration for both study groups was within the insufficient range. A Mann-Whitney test revealed no statistically significant difference between the length of stay and serum vitamin D in both groups (p value 0.86 and 0.09, respectively).
The median serum vitamin D concentration for the patients who required high dependency unit or intensive treatment unit were paradoxically higher than those who did not. However, these numbers are too few to draw any statistically significant conclusion.
The histogram in figure 1 shows the left skew with respect to serum vitamin D concentration in both study groups.

Distribution of study participants into serum vitamin D concentration intervals of 10 nmol/L.
Length of stay analysis
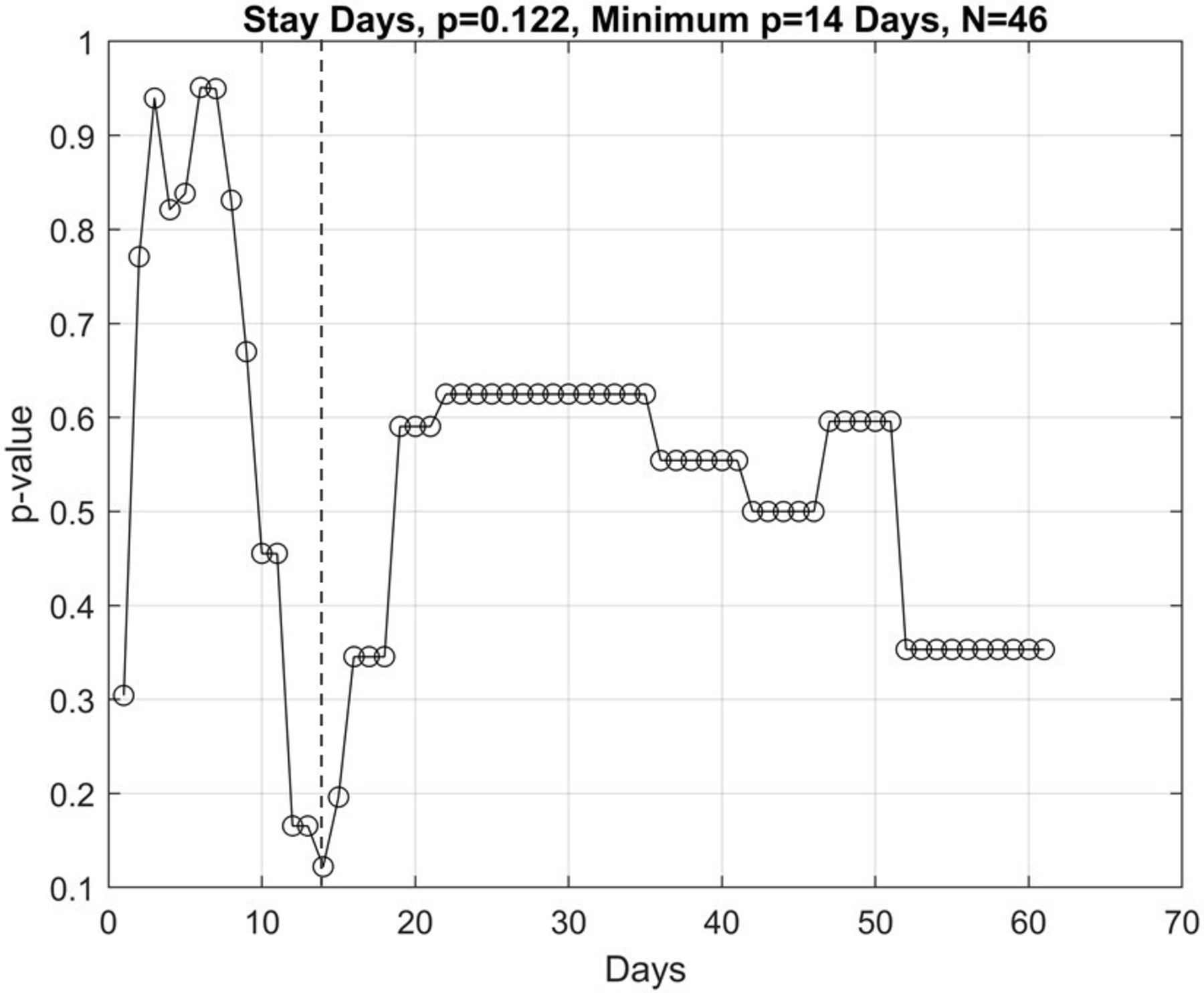
It is observed in figure 2 that the lowest p value of 0.122 was seen when comparing patients discharged with a length of stay shorter than 14 days to those with a length of stay longer than 14 days.
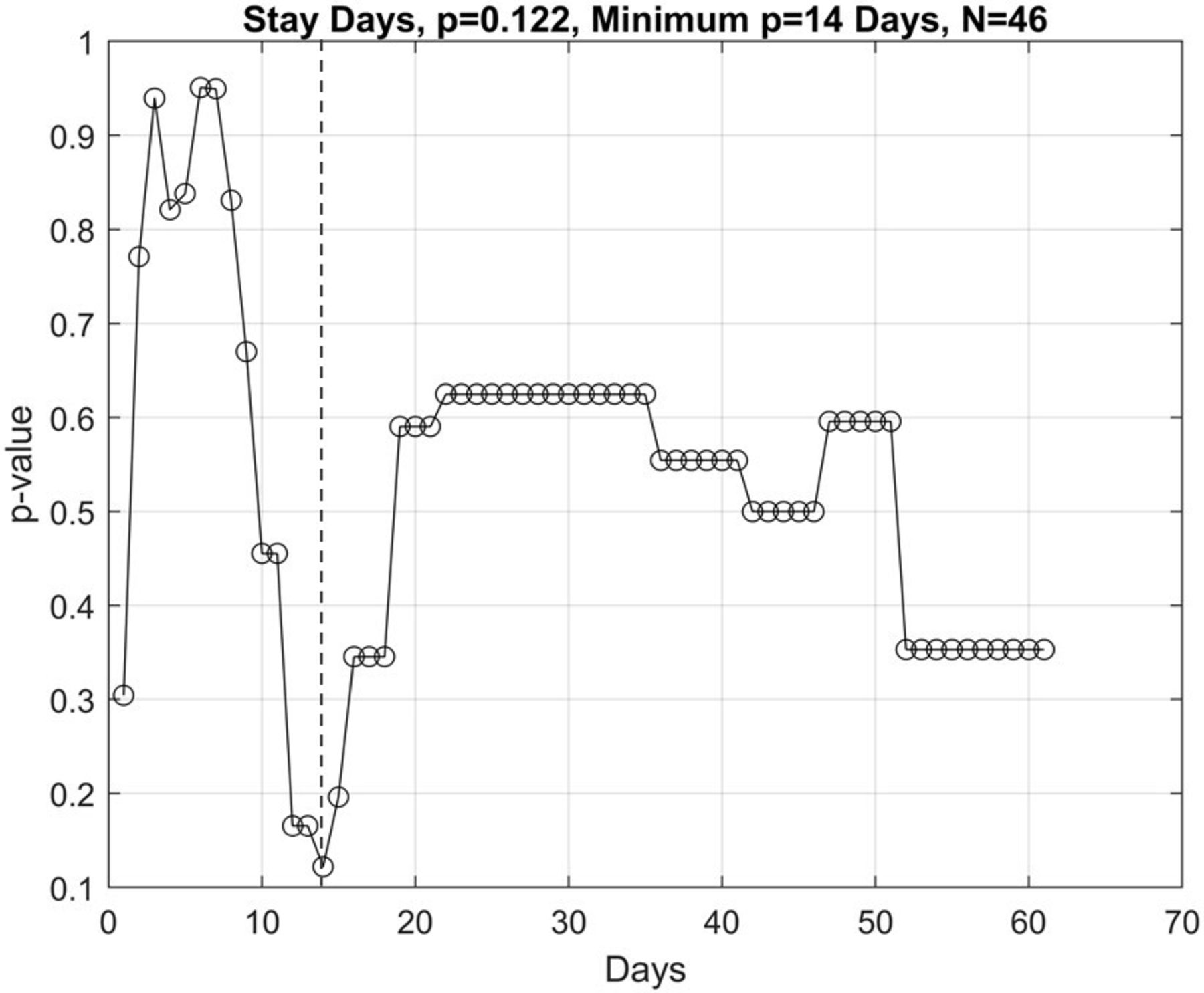
The association analysis of serum vitamin D concentration with respect to length of stay using Mann-Whitney ranked sign test. The x-axis represents the length of hospital stay used to generate dichotomous groups for comparison. The y-axis represents the p values generated when comparing dichotomous groups.
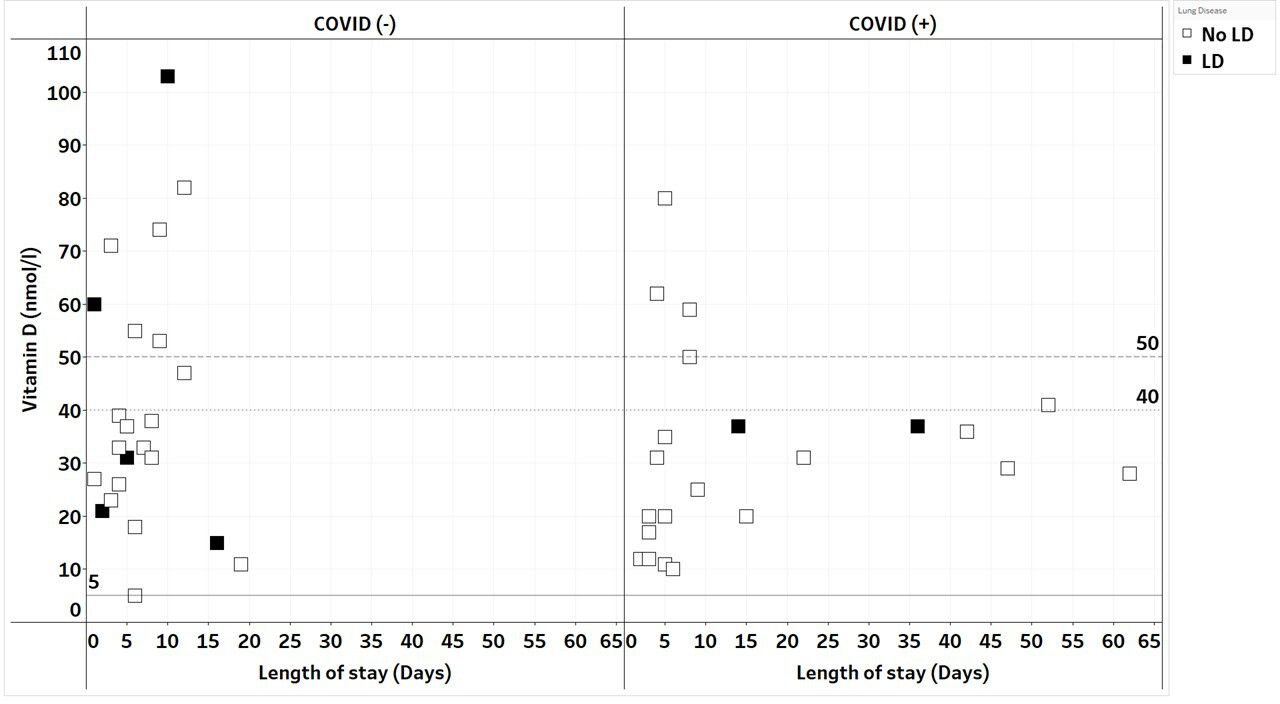
Figure 3 shows that no patient with a vitamin D serum concentration of greater than 50 nmol/L stayed longer than 14 days.

Serum vitamin D concentration with respect to length of stay irrespective of COVID-19 status. Horizontal lines highlight serum vitamin D concentrations of 50 nmol/L and 40 nmol/L.
Subgroup analysis with regards to BMI and comorbidity
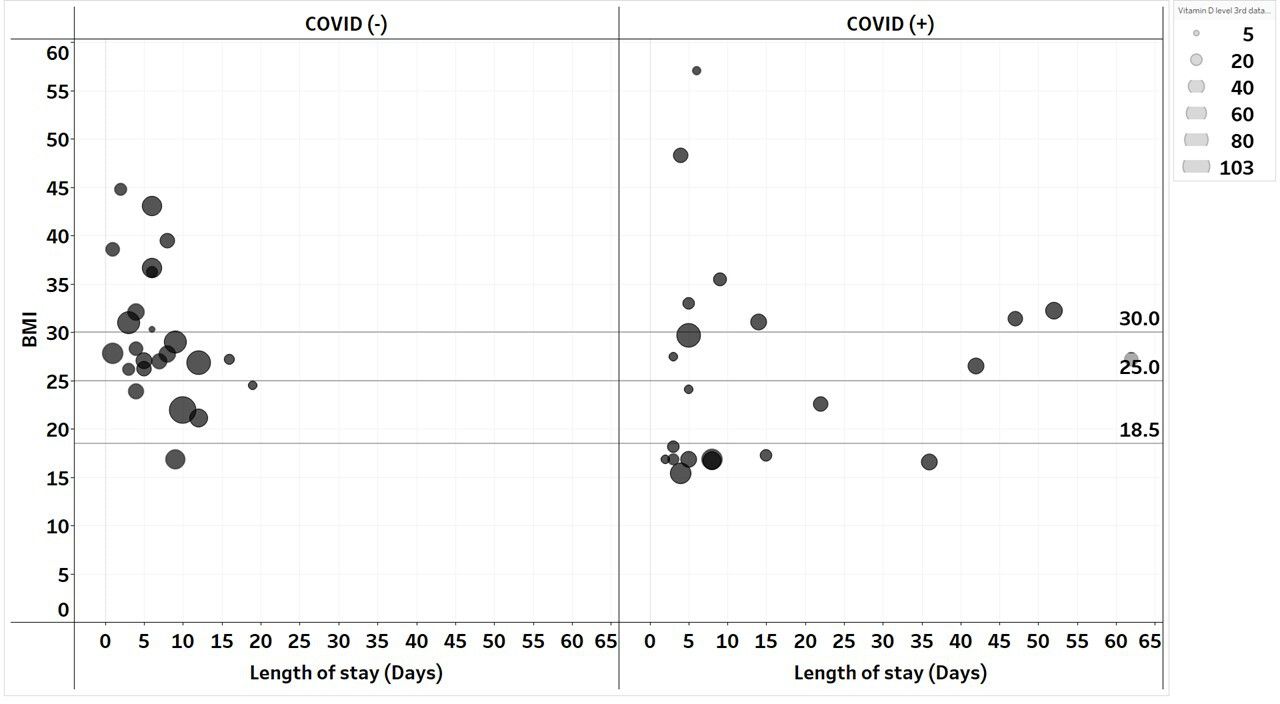
Figure 4 shows that the median BMI of COVID-19-positive patients of 25.3 was not significantly different from the median BMI of 27.8 seen in the COVID-19-negative patients. It can be noted that eight underweight patients (BMI<18.5) were seen in the COVID-19-positive group while only one was seen in the COVID-19-negative group, unfortunately such a small number does not lend itself to statistical comparison. No association was seen between BMI and length of stay, BMI and serum vitamin D concentration, BMI and COVID-19 status.

Distinction between BMI (kg/m2), serum vitamin D concentration, COVID status and length of stay. The x-axis represents length of stay. The y-axis represents the BMI with horizontal lines delineating BMI thresholds. The size of the circle represents the serum vitamin D concentration.
Figure 5 depicts the significant prevalence (37%) of DM in the study sample. There was no association between DM and length of stay or COVID-19 status. However, an association is noticed with regards to DM and serum vitamin D concentration irrespective of COVID-19 status. The majority of the patients with DM (88%) had serum vitamin D concentrations of less than 50 nmol/L.
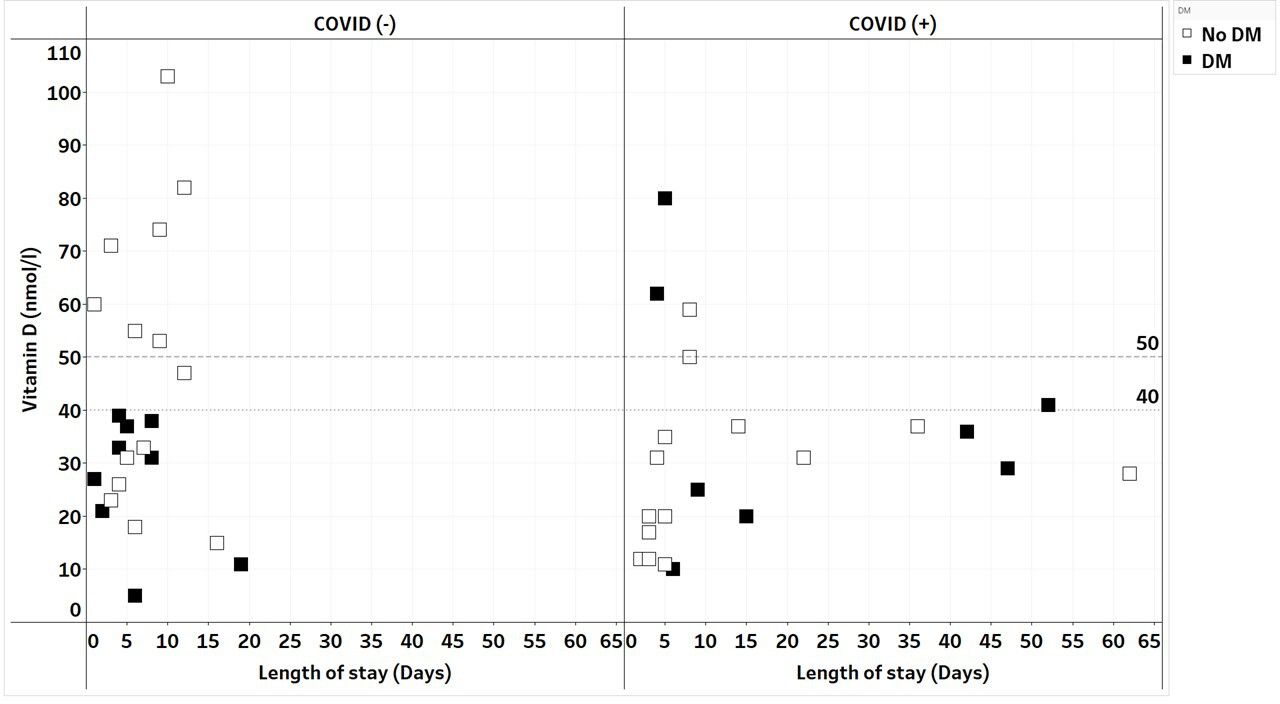
Projection of diabetes mellitus (DM) on COVID-19 status relative to serum vitamin D concentrations and length of stay.
Figure 6 shows that hypertension was seen in 50% of the study sample. No obvious association was seen between hypertension and serum vitamin D concentration, hypertension and length of stay, hypertension and COVID-19 status.
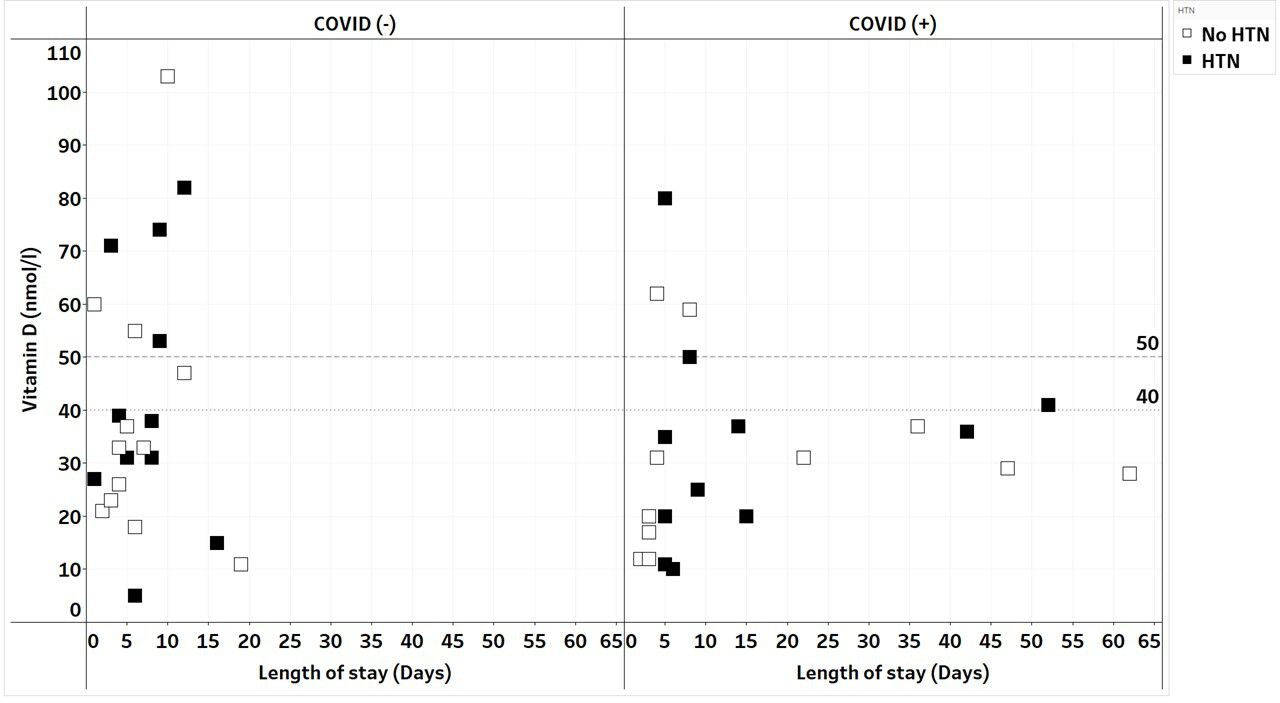
Projection of hypertension (HTN) on COVID-19 status relative to serum vitamin D concentrations and length of stay.
Figure 7 shows lung disease (chronic obstructive pulmonary disease (COPD) and asthma) to have been present in 15% of the study sample. No obvious association was seen between lung disease and serum vitamin D concentration, lung disease and length of stay, lung disease and COVID-19 status.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Projection of lung disease (LD) on COVID-19 status relative to serum vitamin D concentrations and length of stay.
Discussion
The findings of this study demonstrate the significant prevalence of vitamin D insufficiency and deficiency in hospitalised patients with both COVID-19 and non-COVID-19 ARTIs. Eighty per cent of the study sample had a serum vitamin D concentration <50 nmol/L. These results support previous studies demonstrating the presence of low serum vitamin D during ARTIs.25
Such prevalence would advocate for proactive screening of vitamin D, especially in those admitted to hospital for respiratory tract infections. It has been shown that improving overall vitamin D status could help reduce the economic burdens of several diseases.33
We did not observe a statistically significant difference in the serum vitamin D concentrations of patients with COVID-19 compared with non-COVID-19 patients with ARTI, both study groups had low median serum vitamin D concentrations of 30 nmol/L and 35 nmol/L, respectively.
The use of a control group consisting of a non-hospitalised healthy cohort may have produced a starker contrast in serum vitamin D concentration.
In this study, we found no statistically significant association between length of stay and serum vitamin D concentration. However, we did note that no patient with a normal serum vitamin D concentration had a length of stay beyond 14 days. Despite the lack of statistical significance, such an observation suggests further studies with larger sample sizes evaluating length of stay in relation to vitamin D are to be considered.
It is generally known that patients can have a delayed hospital discharge for non-medical reasons such as waiting for an available bed in a nursing home or other facility or waiting for adequate care provisions and equipment to be installed at home. When accounting for such discrepancies, we found no significant difference in outcome to be present.
This study was conducted prior to the widespread use of corticosteroids, antivirals and immunotherapies for the management of COVID-19. Thus, there was no difference in the medical management between the two study cohorts. The treatment for both groups at the time of the study included oxygen therapy and antibiotics to treat for superadded bacterial infections.
A subgroup analysis of comorbidities identified that no significant difference in BMI, hypertension and lung disease were present between the COVID-19 and non-COVID-19 ARTI groups. BMI and the presence of hypertension and lung disease were not associated with discrepancies in length of stay and serum vitamin D concentration. Interestingly, DM was found to be more prevalent in patients with low serum vitamin D concentrations. This particular association has been noted in the literature.34
A large comparative analysis performed in the USA of 906 849 hospitalisations estimated the attributable risk of DM at 20.5%, obesity at 30.2% and hypertension at 26.2%.35 In this study, the substantial prevalence of hypertension and diabetes mellitus within the COVID-19-positive group was apparent at 50% and 37%, respectively.
The limitations of this study include its nature as an ethnically homogenous small sample. This limitation was driven by external factors such as sample collection window and rates of patient turnover. The study was also confined to moderately unwell cases of hospitalised patients requiring less than 8 L/min of oxygen further limiting its size.
Conclusion
This study was able to demonstrate the significant prevalence of vitamin D insufficiency and deficiency in hospitalised patients with ARTIs including COVID-19. This study did not demonstrate patients with COVID-19 to have a statistically significant difference in serum vitamin D compared with non-COVID-19 patients with ARTIs. Both study groups demonstrated near similar insufficiencies and deficiencies in vitamin D. Further studies comparing such groups could provide useful insights into the relationship of serum vitamin D concentration and ARTIs of various aetiologies including COVID-19.
Current literature on COVID-19 and vitamin D is suggestive of an association, a meta-analysis consisting of 39 studies of various designs and sample sizes, along with a meta-analysis of 10 case–control studies have shown vitamin D deficiency to be associated with increased risk of COVID-19 infection.36 37
Further work is required to ascertain whether there is a genuine causation underpinning this relationship.
Data availability statement
Data is available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study obtained local ethical approval from the department of Research and Innovation, Medway Maritime Hospital. Patients did not receive additional venepuncture as part of this study. The blood tests used in this study were done as part of routine clinical assessments for all patients at the trust during the COVID-19 pandemic.
Acknowledgments
We acknowledge the valuable contribution of the patients who participated in this study.
Patients nor the public were involved in the production of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SS is the guarantor of this study. SS conceptualised the study including the study design and obtained the approval from the hospital research team to perform the study on COVID-19 patients during the pandemic. ZAIE performed the data collection and wrote the initial draft of the manuscript. NF provided guidance and direction during the study. JT performed the data analyses, produced the graphs and wrote the data analysis subsection. Revision and editing of the manuscript were performed by all authors. All authors approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.