Article Text

Abstract
Background Public health interventions are essential to prevent a long tail of costly, avoidable and worsening ill health in coastal communities following the COVID-19 pandemic, yet no research exists to guide policy and practice as to which groups within coastal communities are vulnerable and most in need of such interventions. Within this aim, we explore engrained and emerging vulnerabilities of food insecurity, health and well-being for different demographic groups within the deprived coastal community of Fleetwood, Lancashire, UK, before and after the pandemic.
Methods Routinely collected data of free school meal eligibility, community mental health referrals and hospital admissions between 28 March 2016 and 31 December 2021 were aggregated by locality and deprivation within Fleetwood. Temporal autoregressive models, generalised linear mixed models and survival analyses were employed to compare trends and associations in food insecurity, health and well-being indicators against deprivation indices, demographics, comorbidities (including COVID-19), the COVID-19 pandemic period and locality.
Results Areas with better housing and income, but higher health and disability deprivation, showed increased levels of free school meal eligibility following the pandemic. Mental health was insensitive to the first 14 months of pandemic yet is worsened by unemployment deprivation and cardiovascular and respiratory comorbidities, with a greater predisposition to poor mental health in adolescents and young adults. After accounting for the effect of COVID-19, hospital mortality risk increased with demographic influences in fitting with the typology of coastal communities having an older population, struggling healthcare and a greater prevalence of comorbidities.
Conclusions Public health managers and policy makers seeking to prevent worsening health and well-being within coastal communities following the pandemic should focus on broader-scale patterns reflecting entrenched poor health typical of coastal communities, and emerging food insecurity within specific demographic and deprivation groups at finer scales.
- COVID-19
- mental health
- dietary patterns
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A ‘coastal excess’ of poor health and well-being exists, but predictions that this will worsen following the COVID-19 pandemic remain largely untested despite reports of greater economic downturn and food insecurity in coastal areas.
WHAT THIS STUDY ADDS
In addition to increased mortality due to COVID-19, we demonstrate how free school meal eligibility was sensitive to significant increases soon after the pandemic; less so mental health.
We uncover hidden vulnerabilities of food insecurity in different localities and deprivation groups while confirming entrenched patterns of physical and mental health in coastal communities following the pandemic.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Research, practice and policy are better informed as to how the COVID-19 crisis in coastal communities has disrupted the most deprived, and relatively less deprived, yet still vulnerable, groups which can only be represented by appropriately detailed multivariate analyses that use other measures in addition to health outcomes, such as food insecurity, deprivation and spatial data.
Introduction
England’s coastal communities are deprived, neglected and exhibit a ‘coastal excess’ of poorer health and well-being over that of their inland counterparts, with particularly elevated levels of poor mental health, chronic obstructive pulmonary disease, cardiovascular illness, smoking, kidney disease, learning disability and dementia.1 Current research demonstrates the COVID-19 pandemic to have widened this health gap, with coastal communities exhibiting greater age-standardised mortality, long COVID prevalence and unemployment rates,1–4 with similar patterns according to health status, deprivation and demographics shown elsewhere in the country.3–6 However, practice and policy aimed at improving the health of neglected coastal communities is poorly informed because limited research exists that establishes to what extent different deprivation and demographic groups within these coastal communities have experienced continued or worsening health or well-being following the pandemic.1
This work builds on our initial explorative analysis7 to specifically address dynamics of food insecurity, health, well-being, demographics and deprivation within Fleetwood, a medium-sized, socially deprived, coastal town in Lancashire, UK, pre-COVID-19 and post-COVID-19. In doing so, we provide direction for research, policy and practice aimed at reducing the threat of worsening well-being and health in these deprived communities in the face of future health and/or socioeconomic crisis.
Hospital admission data are used to represent the diagnostic and demographic composition of those in hospital by looking at their respective in-hospital mortality and readmission rates. Community mental health referral data are investigated to provide the trends in mental well-being of different demographic groups.
We also assess food insecurity due to its far-reaching and negative impact on families through both the worsening health, mental well-being, behaviour and academic performance of children8–11 and associated poorer physical and mental health of adults.12 Furthermore, these impacts may have worsened following COVID-19, which has exposed new dimensions of food insecurity, especially among adults with children and/or having disabilities, including those typically not considered deprived.13 We use free school meal eligibility data to assess food insecurity in this study as it has been previously used across research practice and policy as a practicable and accessible data source to represent food insecurity and its impacts on household health and well-being.8–11 13 Lastly, free school meals represent a statutory entitlement that strongly connects policy and practice via a wide-reaching and easy to regulate mechanism proven to reduce food insecurity.8
Free school meal eligibility in England includes all pupils in reception, year 1 and year 2 in state-funded schools, and those pupils in year 3 and upwards whose parents claim for free school meals while fulfilling the following highly restrictive income-based selection criteria: income-based jobseekers allowance; income-related employment and support allowance; income support; support under Part 5 of the Immigration and Asylum Act 1999; the guaranteed element of State Pension Credit; Child Tax Credit (provided they are not also entitled to Working Tax Credit and have an annual gross income of no more that £16 900); Working Tax Credit run-on or Universal Credit (with household income of <£7400 per annum after tax excluding any benefits).8 Consequently, children receiving free school meals are likely to be living in low-income households, which is the predominant driver behind food insecurity.13 Children receiving free school meals are also more likely to suffer from food insecurity impacts such as poor dietary intake, poor physical and mental health, poor life satisfaction and educational outcomes,8 many of which themselves represent burdens of poor health in coastal communities.1 7 14 Nationally, the proportion of pupils eligible for free school meals rose from 17.3% in January 2020 to 22.5% in January 2022, representing 1.9 million children (the equivalent of over twice the population of the city of Leeds), with household food insecurity now having reached crisis point.8 13 Thus, identifying which families are most vulnerable to food insecurity following the pandemic will inform and so improve the effectiveness of policy and practice aimed at breaking cycles of poverty, food insecurity, lower educational achievement, mental health and unemployment that may exacerbate poor health and well-being of vulnerable and neglected coastal communities for generations to come.1 8–13
The geographic heterogeneity of health and well-being is explored by aggregating data according to their lower-layer super output area (LSOA). LSOAs are a series of contiguous geographic units that cover the entire spatial extent of the UK. LSOAs are designed to improve the reporting of small area statistics through the consistent representation of population size. In England, LSOAs represent areas with a minimum population of 1000 and an average of 1500 people or 650 households.
The aim of this research is to provide a preliminary assessment of how socioeconomic deprivation and the COVID-19 pandemic modulate food insecurity, mortality and mental health in Fleetwood, and how these results can inform future research, policy and practice.
Study area
Fleetwood is a coastal town in Lancashire home to approximately 30 000 people, many of whom were already experiencing poor health and living in disadvantaged socioeconomic circumstances prior to the pandemic.14 Almost half of neighbourhoods in Fleetwood are among some of the 10% most deprived areas in the country and, like other deprived areas, experience some of the associated poor physical and mental health outcomes.7 14 15 As a coastal community without a large employer or industry, Fleetwood is a place that is geographically and economically ‘on the periphery’ and particularly vulnerable to the impacts of financial crises and pandemics.7 It also has a population older than the English average, with 22% of its population aged over 65 years, compared with 18% nationally.7 Fleetwood is 98% white/Caucasian14 and has an alternative claimant count (a count of combined jobseekers and universal credit claims for those categorised as seeking work) of 27.4 per 1000 people.7
Data collection
All variables considered in this study are listed in online supplemental table S1.
Supplemental material
The effect of deprivation on health and well-being was explored using: (i) the index of multiple deprivation, and its separate components, comprising: (ii) income, (iii) employment, (iv) education, skills and training, (v) health and disability, (vi) crime, (vii) barriers to housing and services and (viii) living environment, collated for each LSOA in 2019 as deciles (decile 1 being the most deprived) by the Ministry of Housing, Communities and Local Government.15
Anonymised hospital admission data between 28 March 2016 and 29 March 2021 was provided by the Lancashire Hospitals Trust, and detailed the patient LSOA, admission date, COVID-19 diagnosis, primary and secondary diagnoses (online supplemental table S1), previous admissions, admission type (planned/unplanned), age and time-to-discharge/death of 7117 hospital admissions representing 4204 unique individuals. To keep anonymity of the patients, LSOAs with less than five records were discarded.
Data on referrals to adult (aged >18 years), children (aged 0–13 years) and adolescent (aged 13–18 years) from Child and Adolescent Mental Health Services (CAMHS) were provided by NHS Lancashire and South Cumbria Foundation Trust. Monthly data from 1 January 2016 to 30 June 2021 were provided. As community mental health referrals data were not available at LSOA level, only temporal analyses were possible.
Monthly count data of total number of female and male primary school pupils and those eligible for free school meals within each LSOA between 1 January 2018 and 31 December 2021 were provided by Lancashire County Council.
Finally, the effect of the pandemic period itself was explored by creating a separate dummy variable (YES/NO), defined as occurring after 11 March 2020 (coincident with the first case of COVID-19 in Fleetwood) for hospital admissions; after 1 March 2020, for community mental health referrals (since they are monthly data) and in the years 2020 or 2021 for free school meal eligibility. For adult mental health referrals, an additional ‘pandemic pulse’ variable16 was used to adjust for the immediate drop in referrals in the early months of the pandemic, defined as pandemic pulse=1 for months March–April 2020, and pandemic pulse=0 for the other months.
Statistical analysis
Binomial and Poisson link functions within generalised linear mixed models17 were employed to assess, respectively, the effect of potential drivers of mental health diagnosis on admission to hospital and free school meal eligibility. Model performance was compared for different fixed and random effects. For the latter, LSOA, age group, COVID-19 diagnosis and the pandemic period were tested.
A Cox proportional hazard model18 was used to assess deprivation, comorbidity, pandemic and COVID-19 effects on time to death from hospital admission. Potential bias resulting from readmission was accounted for by considering readmissions as either a cluster or as a stratum. Schoenfeld residuals were used to identify explanatory factors violating assumptions of proportionality.19
In all models, important variables were initially selected based on univariate models using the criteria of p≤0.2 to indicate a potential association.20 Thereafter, variables were combined sequentially in a backward stepwise approach, removing insignificant terms (p>0.05), which were retested later during model development. Models were selected based on their lowest Akaike Information Criterion value.21 HRs, ORs, incidence rate ratios (IRRs) and their respective 95% CIs were calculated for each important variable within the chosen proportional hazard, binomial or Poisson mixed models, respectively.
The impact of the pandemic period on routine, urgent and total monthly referrals to community mental health services of males and females was examined using autoregressive integrated moving average models.22 Non-stationary means and variances were corrected using differenced time series values and log-transformations, respectively.23 Autocorrelation and partial autocorrelation functions were calculated for different time lags23 to select the model with the lowest autocorrelation between residuals.23 The temporal relationship between referrals and a small number of standardised health and socioeconomic covariates were examined. For referrals to CAMHS, the included covariates were social care contacts and hospital admissions of Fleetwood residents aged under 19 years. For adult referrals, the only included covariate was hospital admissions for people with a secondary diagnosis related to mental health. These covariates were the only ones that showed significant associations with mental health referrals. Except for community health referral data, which was not referenced to a geographic unit, all other data of deprivation, hospital admission and free school meal eligibility were aggregated by LSOA (21 in Fleetwood). Analyses were implemented using the lme4, survival, sjPLOT, ggplot and forecast packages of CRAN-R statistical programming language (https://cran.r-project.org).
Results
Free school meal eligibility
The selected models of free school meal eligibility included LSOA and pandemic as nested random effect components. A strong spatial effect is evident (figure 1), where intercept terms for some LSOAs are 3–6 times greater than others (highlighted in figure 1), while figure 2 highlights LSOAs exhibiting an increase in intercept values due to a pandemic effect. These intercepts represent the background risk of intake of free school meals in each Fleetwood LSOA independently from the explanatory factors used in this study.
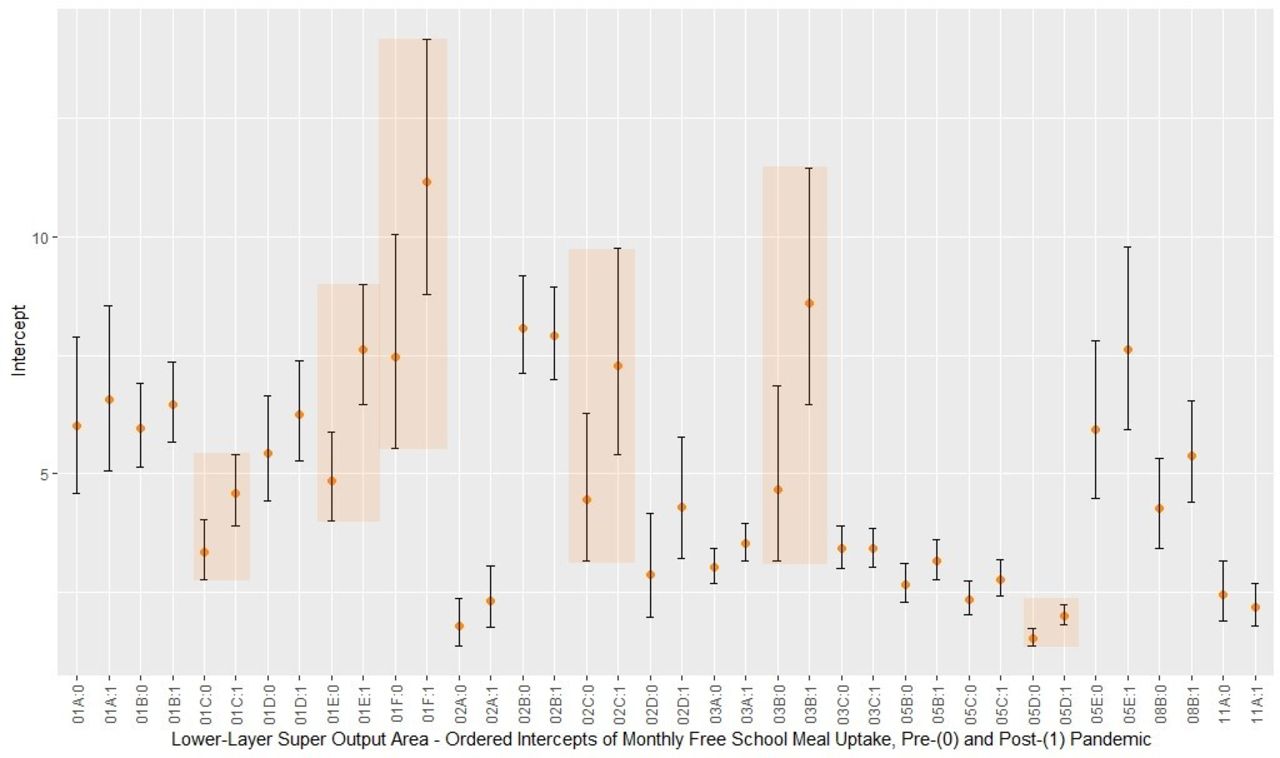
Intercepts of layer super output areas (LSOAs) and pandemic random components used to control for variance when modelling free school meal eligibility in Fleetwood. Intercepts representing free school meal numbers. Alpha-numeric codes refer to each LSOA’s unique identifying code, with a Boolean qualifier separated by a colon to signify prepandemic or postpandemic state: for example, within Fleetwood, the Park Ward of the Wyre Local Authority District has the unique LSOA code 05D and is represented by 05D:0 and 05D:1 in its prepandemic and postpandemic state, respectively. Error bars represent 1 SD from the mean (dots). Highlighted areas draw attention to the large difference between the lowest and greatest free school meal eligibility intercept values.
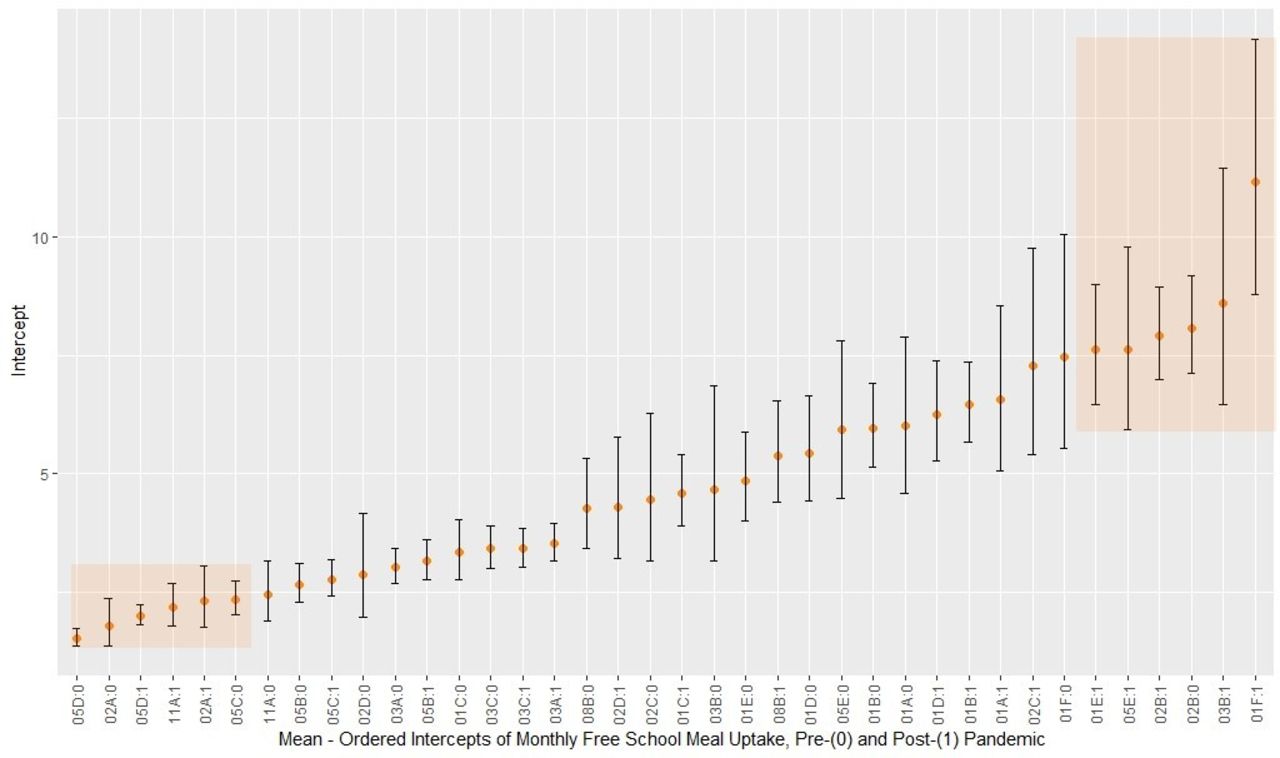
Mean-ordered intercepts of Layer super output area (LSOA) and pandemic random components used to control for variance when modelling free school meal eligibility in Fleetwood. Intercepts representing free school meal numbers. Alpha-numeric codes refer to each LSOA’s unique identifying code, with a Boolean qualifier separated by a colon to signify prepandemic or postpandemic state: for example, within Fleetwood, the Park Ward of the Wyre Local Authority District has the unique LSOA code 05D and is represented by 05D:0 and 05D:1 in its prepandemic and postpandemic state, respectively. Error bars represent 1 SD from the mean (dots). Highlighted areas draw attention to the greatest within-LSOA free school meal eligibility increases following the pandemic.
Male children in areas of higher income had the greatest risk of being eligible for free school meals (IRR=2.85, p=0.002, online supplemental table S2). However, the highest risk factor of free school meal eligibility for female children was living in areas of lower housing and service deprivation. For both male and female children, the highest risk factor is accompanied by high health and disability deprivation (male’s IRR=0.52, p<0.001; female’s IRR=0.65, p<0.001; both genders’ IRR=0.58, p<0.001; with the more deprived having a lower decile). The total number of pupils attending school was included in free school meal eligibility models as an offset to correct for class size.
Mental health
There were 295 hospital admissions of 265 individuals for primary mental health reasons, and 2314 hospital admissions of 1579 individuals admitted for other reasons but having secondary mental health diagnoses. The strongest risk factors for primary mental health admissions (online supplemental table S3) were unplanned admissions (OR 29.33, p<0.001), cardiovascular (OR 2.29, p<0.001) and respiratory (including COVID-19 diagnoses, OR 1.78, p<0.001) comorbidities, and employment deprivation (OR 0.82–0.95, p=0.002), where a higher employment deprivation decile represents a lower level of deprivation. The number of times an individual was readmitted in 12 months prior to the new admission was associated to lower likelihood of primary mental health admission (OR 0.62, p<0.001, online supplemental table S3).
Associations between employment deprivation (OR 0.90, p<0.001), cardiovascular (OR 1.63, p<0.001) and respiratory (including COVID-19) (OR 2.79, p<0.001) comorbidities and admissions with secondary mental health diagnoses were comparable to those of primary mental health admissions except for respiratory diagnosis having a higher risk association than cardiovascular for admissions with secondary mental health diagnoses (online supplemental table S4). Number of previous hospital admissions were not significantly associated with secondary mental health admissions, while both planned and unplanned admissions were risk factors (online supplemental table S4).
The random effect of primary and secondary mental health models depended more on age rather than on LSOA, COVID-19, pandemic period, gender or any of their interactions, with the intercept of the 15–19 years age group being significantly larger than the 0–9 and over 50s age groups for primary mental health admissions (figure 3). However, for secondary mental health diagnoses the 25–29 and 40–44 age group intercepts (figure 4, highlighted) were significantly greater than the 0–19 and over 65 age groups.
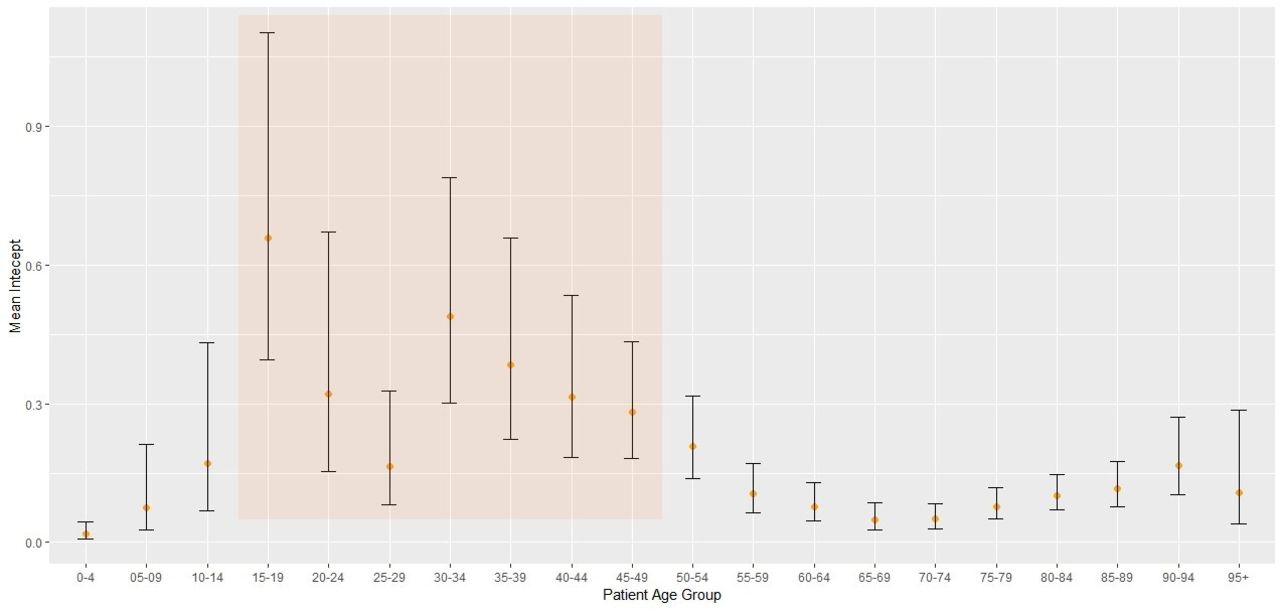
Age-ordered intercepts of age random components when modelling hospital admissions for primary mental health reasons. Error bars represent 1 SD from the mean (dots). Mean intercept is the average monthly number of admissions by age group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-ordered intercepts of age random components when modelling hospital admissions having secondary mental health diagnoses. Error bars represent 1 SD from the mean (dots). Mean intercept is the average monthly number of admissions by age group.
Mental health referrals decreased for all children and male adolescents (online supplemental figure S1, online supplemental tables S5 and S6) while increasing for adults (online supplemental figure S2, online supplemental tables S7-S9) following March 2020, but these patterns reflect trends established prior to the pandemic. Routine and total adult mental health referrals dropped immediately following March 2020, but this returned to pre COVID-19 levels by Summer 2020 (online supplemental figure S2, online supplemental table S10), meaning statistically significant changes in referrals were limited to the first 2 months of the pandemic (online supplemental table S10). Urgent adult referrals had a slight increasing trend throughout the study period and a large spike around the beginning of 2021 (online supplemental figure S2).
In-hospital mortality
Once the COVID-19 effect was accounted for, age, cancer comorbidity and unplanned admissions were the dominant factors that increased in-hospital mortality (online supplemental table S11), while having a mental health condition was associated with increased survival duration.
Discussion
Free school meal eligibility
We uncover for the first time hidden vulnerabilities of food insecurity in a deprived coastal town for both males and females living in areas with better housing and services, yet greater health and disability deprivation. Our findings support emerging evidence suggestive of increased food insecurity for those with children, having disabilities and being just outside the free school meal eligibility criteria,8 11 13 such as the ‘working poor’,12 who being in work but on low pay, are more likely to live in middle-income housing rather than subsidised rent yet may having experienced the greatest financial disruption to their lives following the pandemic.13 24 This may also indicate free school meal eligibility to under-represent these groups given its highly restrictive, income-based, eligibility criteria.8 11 Importantly, these findings highlight the role of fine-scale data in uncovering otherwise hidden spatial gradients of food insecurity, where free school meal eligibility changes from one neighbourhood to the next. This may reflect neighbourhood-scale characteristics not considered here but shown elsewhere to impact free school meal eligibility, such as ethnicity, ethics, dietary preferences, social cohesion, stigmatism, distance to school and other barriers to uptake.11
Mental health
We found no effect after the first 14 months of the COVID-19 pandemic on mental health hospital admissions, nor a pandemic effect on mental health referrals beyond existing trends or a transient ‘pandemic pulse’ (online supplemental figure S1, online supplemental tables S8 and S9).
Our findings support those of others who show mental health in adults to have worsened immediately following the pandemic,25 including those of a recent meta-analysis representing 65 studies, which concluded mental health to have returned to prepandemic levels by mid-2020.26 However, as the acute symptoms of mental health subside, long-term mental health disorders may arise from the pandemic due to the knock-on effects of unemployment, unhealthy coping mechanisms and unsustainable healthcare.27 28 Results presented here agree with established associations between poor mental health, unemployment,29 30 cardiovascular and respiratory comorbidities,30 smoking,30 multimorbidity30–33 and unplanned admissions (online supplemental tables S3 and S4),34 35 whereby the latter is disproportionately costly, damaging and indicative of poor healthcare performance or overburden.32
Younger people were more likely to be admitted to hospital for primary (15–49 years of age with few exceptions, figure 3) rather than secondary (25–64 year of age with few exceptions, figure 4) mental health reasons. These findings support patterns of higher self-harm, greater mental illness and worse mental health for younger people in coastal settings and aligns with a national trend of suicide as a leading cause of mortality in those aged 20–34 years.1–4 33 36
Hospital mortality
Relationships of increased in-hospital mortality associated with COVID-19 admissions and the pandemic period (the effect of which is more structural than individual) mimic patterns shown elsewhere34 35 37 being exacerbated by older age, unplanned admissions and cancer comorbidity (online supplemental table S4).
Patterns of mental health admission and hospital mortality in Fleetwood align well with the typology of coastal communities: harbouring multiple morbidities and mortalities associated with an ageing population and an overburdened healthcare system typified by unplanned hospital admissions,32 including elevated levels of respiratory, cardiovascular and mental health illness associated with poor living standards,1–4 and, like elsewhere in the country, a younger part of the population being susceptible to mental health disorders.33 36
Finally, our study is limited to the area of Fleetwood between 28 March 2016 and 31 December 2021 and so may under-represent long-term pandemic effects, nor do we consider effects of mortality in community and ethnicity, noting the latter’s increased risk of food insecurity, poor mental health and higher COVID-19 morbidity.5 38
Conclusion
We discover previously hidden food insecurities within the medium-sized coastal town of Fleetwood following the pandemic. Local government, policy makers and community partners seeking to prevent worsening health and well-being in coastal communities as exacerbated by the pandemic must focus both on engrained and emergent vulnerabilities, including those of nutrition. This is clear in Fleetwood, where the pandemic has exposed vulnerabilities across other dimensions outside broader scale analyses of health outcomes. Here, emergent food insecurity following the pandemic is highly spatially variable and predominates within areas of relatively higher income and better housing yet higher health and disability deprivation. As such, researchers, practice managers and policy makers should be aware of and consider the spatially variable nature of food insecurity as uncovered here, and how this may be under-represented by borough or regional-scale averages of indices used for decision making. This should include an increased role and appreciation of fine-scale, multivariate, analyses that look beyond health outcomes to appropriately represent health dynamics. Similarly, consideration should be given to the appropriate use of broad-scale deprivation indices such as the index of multiple deprivation to represent food insecurity, which may be too general nor adequately represent differences related to the sex of pupils (online supplemental table S2). Finally, the role of nutritional proxies such as free school meal eligibility in identifying community-scale vulnerabilities outside health outcomes should be understood, accounted for and adapted across research, practice and policy.
While mental health in Fleetwood was insensitive to the first 14 months of the pandemic, our work demonstrates its association with age, cardiovascular and respiratory illness and unemployment. This finding adds support to the direction taken by the ‘Healthier Fleetwood’ Initiative (www.healthierfleetwood.co.uk), which promotes synergistic interventions14 that improve mental health while also improving employment opportunities (‘job clubs’29), cardiovascular and respiratory health (physical activity-based interventions30) and the chances of smoking cessation (smoking cessation support services14), all of which may provide social connectivity14 and trusted relationships known to improve mental health of vulnerable young people.39 Given the ageing population of Fleetwood,14 engaging pharmacists to ensure correct medication regimes are upheld in older patients may also be worth consideration as this has been shown to decrease typically costly unplanned mental health hospital admissions elsewhere.32 40
Future research should focus on potentially modulating effects not considered here such as those of spatial aggregation, social cohesion, social capital and ethnicity. Finally, associations uncovered here such as those of food insecurity provide a reference point for exploring impacts of the emerging global food supply crisis and how they may compound long-term pandemic effects.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This protocol was approved by the Lancaster University Faculty of Health and Medicine Research Ethics Committee (reference number: FHMREC20121). The data used in this study are pseudonymised routinely collected data.
Acknowledgments
We thank all the members of Healthier Fleetwood, Future Fleetwood and the Fleetwood public for their support. We would like to thank Mark Spencer, Mike Walker, Afzal Patel, Neil Clarke, Ross Hughes, Collette Taylor, Margaret Orwin, Alicia Elliott, Karl Worsley, Julie Casson, Phil Horner, Stephen Milan and Mark Bowen.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RC and MF carried out the statistical analyses, drafted and revised the paper. MF designed the data collection and aggregation tool and monitored data collection. LS supervised statistical analyses and drafted and reviewed the paper. LS is the guarantor and accepts full responsibility for the finished work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was funded by the NHS, Wyre Council, Healthier Fleetwood, and Lancaster University ESPRC Impact Accelerator Account (reference: IAA: The use of innovative statistical methods aimed at improving the communities afflicted by COVID-19 patients).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.