COVID-19 in Pregnant Women and Neonates: A Systematic Review of the Literature with Quality Assessment of the Studies

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
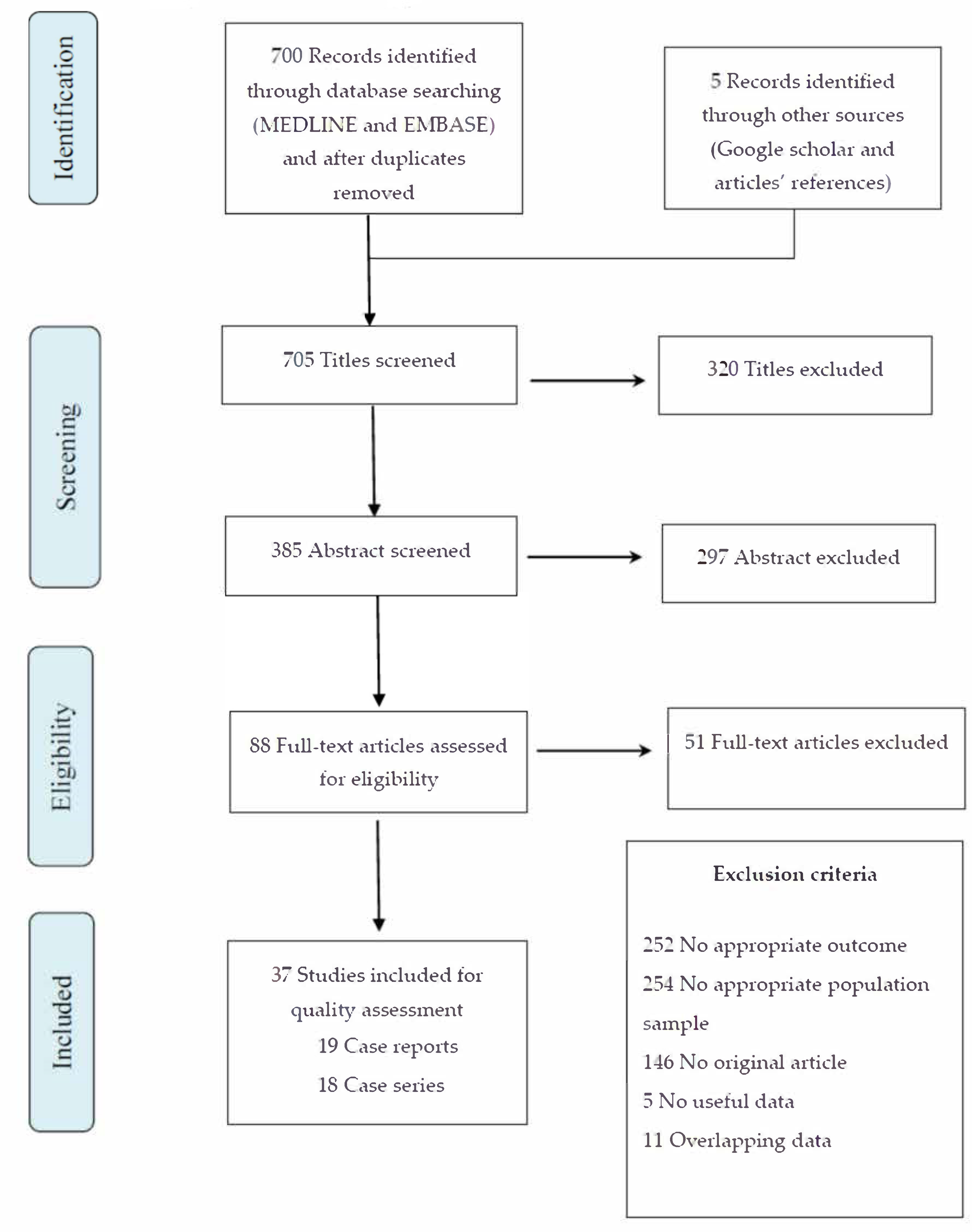
2.1. Study Design and Search Strategy
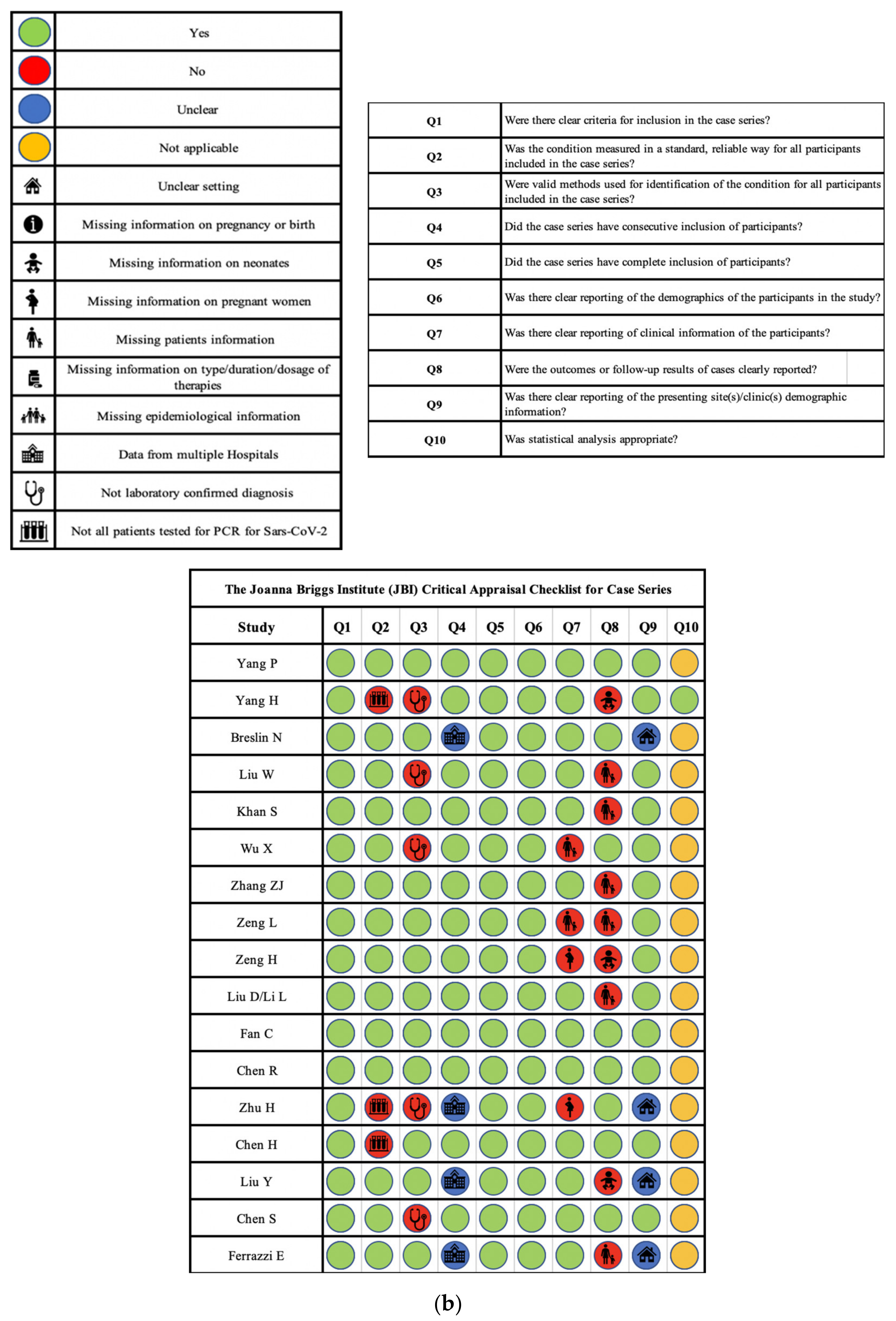
2.2. Study Eligibility and Quality Assessment
2.3. Data Extraction and Definitions
2.4. Statistical Analysis
3. Results
3.1. Included Studies
3.2. Quality Assessment
3.3. Maternal Characteristics and Outcomes
3.4. Neonatal Characteristics and Outcomes
4. Discussion
4.1. SARS-CoV-2 Infection in Pregnant Women
4.2. SARS-CoV-2 Infection in Neonates
4.3. International Guidelines on the Management of Infected Pregnant Women and Neonates
4.4. Limitations of the Study
5. Conclusions
6. Key Issues
- SARS-CoV-2 infection in pregnant women appeared associated with mild or moderate disease in the majority of cases, with a low incidence of severe complications and low mortality rates;
- Outcomes of neonates born from infected women were mainly favorable, although neonates at risk should be closely monitored to carry out early intervention for patients with abnormal findings;
- Further studies are needed to investigate the possibility of vertical transmission.
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kakodkar, P.; Kaka, N. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 History of the outbreak. Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [Green Version]
- De Wit, E.; van Doremalen, N.; Falzarano, D.; Munster, V.J. “SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Microbiol. 2016, 14, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wang, L.L.; Zhao, S.J.; Kwak-Kim, J.; Mor, G.; Liao, A.H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J. Reprod. Immunol. 2020, 139, 103122. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Graham, A.L. Potential maternal and infant outcomes from coronavirus 2019-NCOV (SARS-CoV-2) infecting pregnant women: Lessons from SARS, MERS, and other human coronavirus infections. Viruses 2020, 12, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med Res. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Database Syst. Rev. Implement. Rep. 2019, 23, 1–7. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, J.S.W.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- China N H CotPsRo. New Coronavirus Pneumonia Prevention and Control Program (Seventh Trial Edition) (2020); National Health Commission: Beijing, China, 2020. [Google Scholar]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Paret, M.; Lighter, J.; Madan, R.P.; Raabe, V.N.; Shust, G.F.; Ratner, A.J. SARS-CoV-2 infection (COVID-19) in febrile infants without respiratory distress. Clin. Infect. Dis. 2020, 452. [Google Scholar] [CrossRef]
- Han, M.S.; Seong, M.-W.; Heo, E.Y.; Park, J.G.; Kim, N.; Shin, S.; Cho, S.I.; Park, S.S. Sequential analysis of viral load in a neonate and her mother infected with SARS-CoV-2. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowe, B.; Bopp, B. COVID-19 vaginal delivery—A case report. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 465–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karami, P.; Naghavi, M.; Feyzi, A.; Aghamohammadi, M.; Novin, M.S.; Mobaien, A.; Qorbanisani, M.; Karami, A.; Norooznezhad, A.H. Mortality of a pregnant patient diagnosed with COVID-19: A case report with clinical, radiological, and histopathological findings. Travel Med. Infect. Dis. 2020, 101665. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Wei, H.; Zhang, Z.; Chang, J.; Ma, X.; Gao, X.; Chen, Q.; Pang, Q. Vaginal Delivery Report of a Healthy Neonate Born to a Convalescent Mother with COVID19. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Gidlöf, S.; Savchenko, J.; Brune, T.; Josefsson, H. COVID-19 in pregnancy with comorbidities: More liberal testing strategy is needed. Acta Obstet. Gynecol. Scand. 2020. [Google Scholar] [CrossRef] [Green Version]
- Kalafat, E.; Yaprak, E.; Cinar, G.; Varli, B.; Ozisik, S.; Uzun, C.; Azap, A.; Koc, A. Lung ultrasound and computed tomographic findings in pregnant woman with COVID-19. Ultrasound Obstet. Gynecol. 2020, 55, 835–837. [Google Scholar] [CrossRef] [Green Version]
- Díaz, C.A.; Maestro, M.L.; Pumarega, M.T.M.; Antón, B.F.; Alonso, C.P. First case of neonatal infection due to SARS-CoV-2 in Spain. An. Pediatr. 2020, 92, 237–238. [Google Scholar] [CrossRef]
- Aghdam, M.K.; Jafari, N.; Eftekhari, K. Novel coronavirus in a 15-day-old neonate with clinical signs of sepsis, a case report. Infect. Dis. 2020, 52, 427–429. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Lee, J.; Kim, E.; Woo, K.; Park, H.Y.; An, J. Emergency cesarean section performed in a patient with confirmed severe acute respiratory syndrome Coronavirus-2: A case report. Korean J Anesthesiol. 2020. [Google Scholar] [CrossRef]
- Zambrano, L.I.; Fuentes-Barahona, I.C.; Bejarano-Torres, D.A.; Bustillo, C.; Gonzales, G.; Vallecillo-Chinchilla, G.; Sanchez-Martínez, F.E.; Valle-Reconco, J.A.; Sierra, M.; Bonilla-Aldana, D.K.; et al. A pregnant woman with COVID-19 in Central America. Travel Med. Infect Dis. 2020, 101639. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 from an Infected Mother to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, W.; Dan, W.; Guo-Ce, C.; Xu-Wei, T.; Ling-Kong, Z. SARS-CoV-2 infection with gastrointestinal symptoms as the first manifestation in a neonate. Chin. J. Contemp. Pediatr. 2020, 22, 211–214. [Google Scholar] [CrossRef]
- Wen, R.; Sun, Y.; Xing, Q.S. A patient with SARS-CoV-2 infection during pregnancy in Qingdao, China. J. Microbiol. Immunol. Infect. 2020, 53, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, R.; Zheng, S.; Chen, X.; Wang, J.; Sheng, X.; Zhou, J.; Cai, H.; Fang, Q.; Yu, F. Lack of Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, China. Emerg. Infect. Dis. 2020, 26, 1335–1336. [Google Scholar] [CrossRef]
- Wang, X.; Zhou, Z.; Zhang, J.; Zhu, F.; Tang, Y.; Shen, X. A case of 2019 Novel Coronavirus in a pregnant woman with preterm delivery. Clin. Infect. Dis. 2020, 10, ciaa200. [Google Scholar] [CrossRef]
- Iqbal, S.N.; Overcash, R.; Mokhtari, N.; Saeed, H.; Gold, S.; Auguste, T.; Mirza, M.; Ruiz, M.; Chahine, J.J.; Waga, M.; et al. An Uncomplicated Delivery in a Patient with Covid-19 in the United States. N. Engl. J. Med. 2020, 382, e34. [Google Scholar] [CrossRef]
- Song, L.; Xiao, W.; Ling, K.; Yao, S.; Chen, X. Anesthetic Management for Emergent Cesarean Delivery in a Parturient with Recent Diagnosis of Coronavirus Disease 2019 (COVID-19): A Case Report. Transl. Perioper. Pain Med. 2019, 7, 234–237. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.K.; Tao, X.W.; Yuan, W.H.; Wang, J.; Liu, X.; Liu, Z.S. First case of neonate infected with novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 2020, 58, E009. [Google Scholar] [CrossRef]
- Yang, P.; Wang, X.; Liu, P.; Wei, C.; He, B.; Zheng, J.; Zhao, D. Clinical characteristics and risk assessment of newborns born to mothers with COVID-19. J. Clin. Virol. 2020, 104356. [Google Scholar] [CrossRef]
- Li, L.; Liu, D.; Yang, L. Follow-Up Information About the Four Pregnant Patients with Coronavirus Disease (COVID-19) Pneumonia Who Were Still in the Hospital at the End of Our Study. Am. J. Roentgenol. 2020, W1–W2. [Google Scholar] [CrossRef]
- Breslin, N.; Baptiste, C.; Gyamfi-Bannerman, C.; Miller, R.; Martinez, R.; Bernstein, K.; Ring, L.; Landau, R.; Purisch, S.; Friedman, A.M.; et al. COVID-19 infection among asymptomatic and symptomatic pregnant women: Two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am. J. Obstet. Gynecol. MFM 2020, 2, 100118. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Sun, G.; Tang, F.; Peng, M.; Gao, Y.; Peng, J.; Xie, H.; Zhao, Y.; Jin, Z. Clinical features and outcomes of pregnant women suspected of coronavirus disease 2019. J. Infect. 2020, 81, e40–e44. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, J.; Li, W.; Zhou, Z.; Liu, S.; Rong, Z. Clinical characteristics of 19 neonates born to mothers with COVID-19. Front. Med. 2020, 14, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Peng, L.; Siddique, R.; Nabi, G.; Nawsherwan; Xue, M.; Liu, J.; Han, G. Impact of COVID-19 infection on pregnancy outcomes and the risk of maternal-to-neonatal intrapartum transmission of COVID-19 during natural birth. Infect. Control Hosp. Epidemiol. 2020, 41, 748–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Sun, R.; Chen, J.; Xie, Y.; Zhang, S.; Wang, X. Radiological findings and clinical characteristics of pregnant women with COVID-19 pneumonia. Int. J. Gynaecol. Obstet. 2020, 150, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J.; Yu, X.; Fu, T.; Liu, Y.; Jiang, Y.; Yang, B.X.; Bi, Y. Novel Coronavirus Infection in Newborn Babies Under 28 Days in China. Eur. Respir. J. 2020. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal Early-Onset Infection with SARS-CoV-2 in 33 Neonates Born to Mothers with COVID-19 in Wuhan, China. JAMA Pediatr. 2020, e200878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrazzi_Mode of Delivery and Clinical Findings in COVID-19-Infected Pregnant Women in Northern Italy. PREPRINT. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3562464 (accessed on 10 April 2020).
- Fan, C.; Lei, D.; Fang, C.; Li, C.; Wang, M.; Liu, Y.; Bao, Y.; Sun, Y.; Huang, J.; Guo, Y.; et al. Perinatal Transmission of COVID-19 Associated SARS-CoV-2: Should We Worry? Clin. Infect. Dis. 2020, ciaa226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Zeng, H.; Xu, C.; Fan, J.; Tang, Y.; Deng, Q.; Zhang, W.; Long, X. Antibodies in Infants Born to Mothers with COVID-19 Pneumonia. JAMA 2020, 323, 1848–1849. [Google Scholar] [CrossRef]
- Chen, S.; Huang, B.; Luo, D.J.; Li, X.; Yang, F.; Zhao, Y.; Nie, X.; Huang, B.X. Pregnant women with new coronavirus infection: A clinical characteristics and placental pathological analysis of three cases. Zhonghua Bing Li Xue Za Zhi 2020, 49, E005. [Google Scholar] [CrossRef]
- Chen, R.; Zhang, Y.; Huang, L.; Cheng, B.; Xia, Z.; Meng, Q. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing Cesarean delivery: A case series of 17 patients. Can. J. Anesth. 2020, 67, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Wang, L.; Fang, C.; Peng, S.; Zhang, L.; Chang, G.; Xia, S.; Zhou, W. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. Transl. Pediatrics 2020, 9, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Li, L.; Wu, X.; Zheng, D.; Wang, J.; Yang, L.; Zheng, C. Pregnancy and Perinatal Outcomes of Women with Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Analysis. Am. J. Roentgenol. 2020, 18, 1–6. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Tang, K.; Guo, Y. Clinical manifestations and outcome of SARS-CoV-2 infection during pregnancy. J. Infect. 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Liu, S.; Tan, T.; Huang, W.; Dong, Y.; Chen, L.; Chen, Q.; Zhang, L.; Zhong, Q.; Zhang, X.; et al. Treatment with convalescent plasma for critically ill patients with SARS-CoV-2 infection. Chest 2020, 1–5. [Google Scholar] [CrossRef]
- Panahi, L.; Amiri, M.; Pouy, S. Risks of Novel Coronavirus Disease (COVID-19) in Pregnancy; a Narrative Review. Arch. Acad. Emerg. Med. 2020, 8, e34. [Google Scholar]
- Karimi-Zarchi, M.; Neamatzadeh, H.; Dastgheib, S.A.; Abbasi, H.; Mirjalili, S.R.; Behforouz, A.; Ferdosian, F.; Bahrami, R. Vertical Transmission of Coronavirus Disease 19 (COVID-19) from Infected Pregnant Mothers to Neonates: A Review. Fetal Pediatric Pathol. 2020, 39, 246–250. [Google Scholar] [CrossRef] [Green Version]
- Zaigham, M.; Andersson, O. Maternal and Perinatal Outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet. Gynecol. Scand. 2020. [Google Scholar] [CrossRef] [Green Version]
- WHO. Consensus Document on the Epidemiology of Severe Acute Respiratory Syndrome (SARS). 2003. Available online: https://www.who.int/csr/sars/en/WHOconsensus.pdf (accessed on 30 January 2020).
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 200642. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Liu, F.; Li, J.; Zhang, T.; Wang, D.; Lan, W. Clinical and CT imaging features of the COVID-19 pneumonia: Focus on pregnant women and children. J. Infect. 2020, 80, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final Data for 2018 Figure 1. Number and rate of triplet and higher-order multiple births: United States. Natl. VitalStatistics Rep. 2019, 68, 1980–2018. [Google Scholar]
- Kimberlin, D.W.; Stagno, S. Can SARS-CoV-2 Infection Be Acquired in Utero?: More Definitive Evidence Is Needed. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Available online: https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2020/03/novel-coronavirus-2019 (accessed on 5 April 2020).
- Royal College of Obstetricians and Gynaecologist. Information for Healthcare Professionals Coronavirus (COVID-19) Infection in Pregnancy 2; Royal College of Obstetricians and Gynaecologist: London, UK, 2020. [Google Scholar]
- Davanzo, R.; Moro, G.; Sandri, F.; Agosti, M.; Moretti, C.; Mosca, F. Breastfeeding and Coronavirus Disease-2019. Ad interim indications of the Italian Society of Neonatology endorsed by the Union of European Neonatal & Perinatal Societies. Matern. Child Nutr. 2020, e13010. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Design | Setting, Country | Population | Objective | Results |
|---|---|---|---|---|---|
| Yang P | Case series | Zhongnan Hospital of Wuhan University, Wuhan, China | 7 pregnant women with COVID-19 7 neonates | To describe clinical characteristics of neonates born from pregnant women with SARS-CoV-2 | Good outcomes were reported for pregnant women with SARS-CoV-2 and their offspring of neonatal pharyngeal swabs, amniotic fluid samples, and umbilical cord blood samples all tested negative for SARS-CoV-2 by RT-PCR. |
| Paret M | Case report | Department of Pediatrics, Division of Pediatric Infectious Diseases, New York University Grossman School of Medicine, New York, USA | 1 neonate | To describe clinical characteristics of SARS-CoV-2 infection in febrile infants | No adverse outcomes were reported in neonates with SARS-CoV-2 infection. Encourage routine testing of febrile infants for SARS-CoV-2, even if they lack respiratory symptoms. |
| Li L | Case series | Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China | 4 pregnant women with COVID-19 | To describe follow-up characteristics of 4 women already described in the previous article | Pregnant women suffering from pneumonia due to SARS-CoV-2 did not experience severe symptoms or acute respiratory distress syndrome during follow-up (follow-up of Liu D pregnant women) |
| Han MS | Case report | Seoul National University Children’s Hospital, Seoul, Korea, | 1 neonate | To describe the clinical characteristics of COVID-19 in a neonate and her mother; to analyze the viral load of SARS-CoV-2 in clinical specimens from different sources. | SARS-CoV-2 infection did not lead to adverse outcomes in the neonate. SARS- CoV-2 could be shed for a long time in urine and stool. |
| Yang H | Case series | Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. | 13 pregnant women with COVID-19 14 neonates | To describe the clinical characteristics and outcomes of pregnant women with confirmed SARS-CoV-2 infection | 13 Pregnant women with confirmed SARS-CoV-2 pneumonia experienced mild symptoms or were asymptomatic. All neonates tested for SARS-CoV-2 were negative. Pulmonary CT scan can be used to screen SARS-CoV-2 pregnant women in the outbreak area of SARS-CoV-2 infection. |
| Lowe B | Case report | Gold Coast University Hospital (GCUH), Southport, QLD, Australia | 1 pregnant woman with SARS-CoV-2 1 neonate | To describe a vaginal birth in a SARS-CoV-2 mother | Vaginal birth in a SARS-CoV-2 patient occurred without complications Rooming-in post-delivery for SARS-CoV-2 positive parents and breastfeeding appears possible and safe when appropriate precautions are taken. |
| Breslin N | Case series | Columbia University Irving Medical Center and Allen Hospital, New York, NY, USA | 43 pregnant women with COVID-19 18 neonates | To describe the clinical characteristics and outcome of pregnant women with COVID-19 and their neonates | The severity of COVID-19 is similar in pregnant women and non-pregnant adults. Ten women delivered vaginally without any complication. All neonates tested negative for SARS-CoV-2 |
| Liu W | Case series | Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China | 19 pregnant women with COVID-19 19 neonates | To describe the clinical characteristics and outcomes of 19 neonates born to mothers suffered from COVID-19 | RT PCR for SARS-CoV-2 tested negative on all neonatal throat swabs, gastric fluid, urine, feces, amniotic fluid, and umbilical cord blood. No one showed any clinical, radiologic, or biochemical sign of COVID-19. |
| Karami P | Case report | Vali-e-asr Hospital, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran | 1 pregnant woman with COVID-19 1 neonate | To describe a case of maternal and fetus death in a patient with COVID-19 | A 27-year-old pregnant woman at 30+3 weeks suffering respiratory distress requiring ICU admission and mechanical ventilation. She delivered vaginally after the spontaneous onset of uterine contractions. The neonate was stillborn, with Apgar 0 and did not respond to resuscitation. Lately she developed ARDS, MOF, and finally death. |
| Khan S | Case series | Renmin Hospital of Wuhan University, Wuhan, China | 3 pregnant women with COVID-19 3 neonates | To describe vaginal birth in SARS-CoV-2-positive mothers | Vaginal delivery was uncomplicated in SARS-CoV-2-positive mothers. All the 3 neonates tested negative for SARS-CoV-2. No vertical transmission of SARS-CoV-2 or intrapartum transmission was found. |
| Xiong X | Case report | Beijing YouAn Hospital, Beijing, China | 1 pregnant woman with COVID-19 1 neonate | To describe a vaginal birth in a SARS-CoV-2 positive mother | Vaginal birth in a SARS-CoV-2-positive mothers was uncomplicated. Neonate tested negative for SARS-CoV-2. No vertical transmission of SARS-CoV-2 or intrapartum transmission was found. |
| Wu X | Case series | Central Hospital of Wuhan, Wuhan, China | 23 pregnant women with COVID-19 21 neonates | To describe the clinical characteristics and to study chest CT images in SARS-CoV-2-infected pregnant women | Pregnant and non- pregnant women with SARS-CoV-2 presented similar radiological findings and clinical characteristics. Four of the 21 neonates were negative for SARS-CoV-2 on RT-PCR, 17 were clinically diagnosed as negative. |
| Zhang ZJ | Case series | Data from central government and local healthdepartments, China | 3 pregnant women with COVID-194 neonates with nucleic acid-confirmed SARS-CoV-2 | To describe the clinical characteristics and outcome of neonates with SARS-CoV-2 | Compared with adults, neonates showed milder symptoms and better outcomes. |
| Gidlöf S | Case report | Stockholm, Sweden | 1 pregnant woman with COVID-19 2 neonates | To describe the clinical characteristics and outcome of a pregnant woman with COVID-19 and her neonates; to ask for liberal testing for SARS-CoV-2 in high-risk patients. | No evidence of vertical transmission. Normal neonatal outcome. |
| Kalafat E | Case report | Ankara, Turkey | 1 pregnant woman with COVID-19 1 neonate | To describe lung ultrasound role in a pregnant COVID-19 woman | Lung-ultrasound examination is easy and could be useful in pregnant women with COVID-19 All neonatal samples tested negative for SARS-CoV-2 (swabs, cord blood, and placental swab). Mother still in ICU at time of publication. |
| Alonso DÌaz C | Case report | Madrid, Spain | 1 pregnant woman with COVID-9 1 neonate | To describe the clinical characteristics and outcome of a pregnant woman with SARS-CoV-2 and her neonate | The mother was asymptomatic at delivery, then needed mechanical ventilation in ICU. This is a suspicious case of horizontal transmission, as the initial neonatal SARS-CoV-2 test was negative. Neonate showed mild symptoms. |
| Kamali Aghdam M | Case report | Mousavi Hospital, Zanjan, Iran | 1 neonate | To describe the clinical outcome of an infected neonate | The neonate had positive throat swab and normal chest X-ray. He rapidly improved with oxygen therapy, fluids, antibiotics, and antiviral treatment (Oseltamivir). Discharged on the 6th day. |
| Lee DH | Case report | Daegu Fatimal Hospital, Daegu, South Korea | 1 pregnant woman with COVID-19 1 neonate | To describe the preventive measures required for delivery in pregnant women with COVID-19 | Mechanical obstruction during labor led to an emergency C-section. Two neonatal throat swab, placental tissue, amniotic fluid sample, and cord blood sample were negative for SARS-CoV-2. |
| Zambrano LI | Case report | Hospital Escuela of Tegucigalpa, Tegucigalpa, Honduras | 1 pregnant woman with COVID-19 1 neonate | To describe the clinical characteristics and outcome of a pregnant woman with COVID-19 and her neonate | The mother showed mild symptoms. Preterm spontaneous vaginal delivery at 32 occurred. RT-PCR test was negative for SARS-CoV-2 on neonatal throat swab. |
| Zeng L | Case series | Wuhan Children’s Hospital, Wuhan, Hubei, China | 33 neonates born from 33 pregnant women with COVID-19 | To evaluate the clinical outcome of neonates born to SARS-CoV-2-infected pregnant women and the possibility of vertical transmission | 3 neonates out of 33 (9%) had positive swabs for SARS-CoV-2 and early symptoms (one might have been septic) |
| Zeng H | Case series | Zhongnan Hospital of Wuhan University, Wuhan, China | 6 neonates born from 6 pregnant women with COVID-19 | To evaluate the possibility of SARS-CoV-2 vertical transmission | Two neonates had positive IgM, 5 had positive IgG, all 6 had raised IL-6 levels. All neonates had negative RT-PCR tests for SARS-CoV-2 on a throat swab |
| Dong L | Case report | Renmin Hospital of Wuhan University, Wuhan, China | 1 pregnant woman with COVID-19 1 neonate | To evaluate the possibility of SARS-CoV-2 vertical transmission | Neonate showed IgM and IgG positive, negative RT-PCR tests for SARS-CoV-2 on throat swab. Abnormal levels of the cytokine. Mother had Vaginal swab and breast milk RT-PCR tests for SARS-CoV-2 negative, NP swab positive. |
| Wang J | Case report | Wuhan Children’s Hospital, Tongji Medical College, Huazhong University of Science & Technology, Wuhan, China | 1 pregnant woman with COVID-19 1 neonate | To describe the clinical outcome of a SARS-CoV-2-infected neonate with gastrointestinal onset | No exams were performed during the birth or immediately after. Ten days after the birth the mother was found positive. Neonate developed GI symptoms and had both NP and anal swab positive. |
| Wen R | Case report | Qingdao Women and Children’s Hospital, Qingdao, China | 1 pregnant woman with COVID-19 | To describe the clinical outcome of a SARS-CoV-2-infected pregnant woman | Pregnant women with SARS-CoV-2 and non-pregnant adults showed similar clinical characteristics. |
| Liu D | Case series | Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China | 15 pregnant women with COVID-19 11 neonates | To describe the clinical characteristics and outcome of a pregnant woman with COVID-19 and her neonate | The severity of SARS-CoV-2 pneumonia was not affected by pregnancy and delivery in these patients.No stillbirth or abortion were reported. No neonate was infected and suffered asphyxia or death. |
| Fan C | Case series | Renmin Hospital of Wuhan University, Wuhan, China | 2 pregnant women with COVID-19 2 neonates | To evaluate the possibility of SARS-CoV-2 vertical transmission | Real-time for SARS-CoV-2 on maternal serum, cord blood, placenta tissue, amniotic fluid, vaginal swab, breast milk, and newborn’s nasopharyngeal swab after delivery were negative. Both mothers and newborns had excellent outcomes. |
| Chen R | Case series | Renmin Hospital of Wuhan University, Wuhan, China | 17 pregnant women with COVID-19 17 neonates | To compare epidural or general anesthesia for C-section delivery in pregnant women with COVID-19; to evaluate the clinical outcome of their newborns | Pregnant COVID-19 women safely received epidural or general anesthesia for Cesarean delivery All neonates tested negative for SARS-CoV-2. |
| Zhu H | Case series | 5 hospitals in Hubei, China | 9 pregnant women with COVID-19 10 neonates | To evaluate the clinical outcome of infected SARS-CoV-2 pregnant women and the possibility of vertical transmission | Perinatal COVID-19 infection could negatively affect neonates. The authors reported fetal distress, premature labor respiratory distress, thrombocytopenia and even one death. Real-time for SARS-CoV-2 on neonatal pharyngeal swabs showed negative results. |
| Chen H | Case series | Zhongnan Hospital of Wuhan University, Wuhan, China | 9 pregnant women with COVID-19 9 neonates | To describe the clinical outcome of SARS-CoV-2-infected pregnant women and the possibility of vertical transmission | Pregnant women with SARS-CoV-2 pneumonia and non-pregnant adult patients SARS-CoV-2 pneumonia have similar clinical characteristics. The authors found no evidence of intrauterine infection (amniotic fluid, cord blood, neonatal throat swab, and breast milk all tested negative for SARS-CoV-2). |
| Liu Y | Case series | Hospitals outside of Wuhan (not better defined in the text), China | 13 pregnant women with COVID-19 9 neonates1 stillborn | To evaluate the clinical outcome of SARS-CoV-2-infected pregnant women and the possibility of vertical transmission | Three Women discharged pregnant; 10 had C-section (emergency in 5 cases), 6 had preterm labor; 1 mother severe case (ARDS+MODS, needed ECMO treatment in ICU, outcome unknown). Neonates: 1 stillborn, 9 well. No evidence of vertical transmission (tests performed not specified). |
| Li Y | Case report | The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China. | 1 pregnant woman with COVID-19 1 neonate | To evaluate the clinical outcome of SARS-CoV-2-infected pregnant woman and the possibility of vertical transmission | No evidence of vertical transmission (feces urine, umbilical cord blood amniotic fluid, placenta, and breast milk samples were negative for RT-PCR for SARS-CoV-2) |
| Wang X | Case report | Affiliated Infectious Hospital of Soochow University, Suzhou, China | 1 pregnant woman with COVID-19 1 neonate | To evaluate the clinical outcome of SARS-CoV-2-infected pregnant woman and the possibility of vertical transmission | No evidence of vertical transmission. (samples of amniotic fluid, placenta, umbilical cord blood, throat swab, stool, gastric juice of the infant for SARS-CoV-2 RT-PCR tests were negative). |
| Chen S | Case series | Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China | 3 pregnant women with COVID-19 3 neonates | To evaluate the placental features of SARS-CoV-2-infected pregnant women and the possibility of vertical transmission | Tissues from 3 placentas showed no morphological alterations due to SARS-CoV-2 infection: no evidence of vertical transmission (SARS-CoV-2 RT-PCR on neonatal swab were negative). |
| Zeng LK | Case report | Wuhan Children’s Hospital of Tongji Medical College, Huazhong University of Science & Technology, Wuhan, China. | 1 neonate | To describe the clinical outcome of a SARS-CoV-2-infected neonate | The neonatal symptoms were mild (fever, rhinitis, refuse of feeding). Anal swab positive for SARS-CoV-2 longer than throat swab. |
| Ferrazzi E | Case series | Hospitals in Northern Italy, Italy | 42 pregnant women with COVID-19 42 neonates | To describe the clinical characteristics and outcome of pregnant women with COVID-19 and their neonates | SARS-CoV-2 syndrome in pregnancy is often mild or moderate. Three SARS-CoV-2 positive newborns (two breastfed without a mask because of post-partum diagnosis and one positive test after vaginal operative delivery). |
| Iqbal SN | Case report | MedStar Washington Hospital Center, Washington, USA | 1 pregnant woman with COVID-19 1 neonate | To evaluate the clinical outcome of a SARS-CoV-2-infected pregnant woman with vaginal delivery | Vaginal delivery in a SARS-CoV-2-infected mother was uncomplicated. No vertical transmission of SARS-CoV-2 or intrapartum transmission was found. |
| Song L | Case report | Wuhan Union Hospital, Wuhan, China | 1 pregnant woman with COVID-19 1 neonate | To describe the perioperative management of a pregnant women with COVID-19 who underwent an urgent C-section | Both epidural and spinal and anesthesia during an emergent cesarean delivery were safe. SARS-CoV-2 RT-PCR on neonatal swab at 3 and 7 days of life were negative. |
| Maternal Characteristics | N | % |
|---|---|---|
| Total pregnant women | 275 | |
| Ongoing pregnancies | 33 | 12 |
| Abortion in the first trimester | 3 | 1.1 |
| Gestational age | N | % |
| Total pregnant women with data | 208 | 76 |
| Missing data | 31 | 11 |
| <37 weeks of gestation | 48 | 23 |
| ≥37 weeks of gestation | 160 | 77 |
| Type of delivery | N | % |
| Deliveries | 239 | 87 |
| Vaginal | 60 | 25 |
| C-section * | 179 | 75 |
| Emergency C-section | 27 | 11 |
| Symptoms | N | % |
| Total pregnant women with data | 269 | 98 |
| Missing data | 6 | 2 |
| Fever | 155 | 58 |
| Cough | 98 | 36 |
| Mild respiratory symptoms (nasal congestion; sore throat) | 9 | 3 |
| Dyspnea | 28 | 10 |
| Myalgia/malaise/fatigue | 37 | 14 |
| GI symptoms (diarrhea or abdominal pain) | 9 | 3 |
| Asymptomatic | 22 | 8 |
| Complications | N | % |
| O2 therapy | 36 | 13 |
| ICU admission | 10 | 4 |
| Invasive ventilation/ECMO | 5 | 2 |
| Death | 1 | 0.03 |
| pPROM, preterm labor | 24 | 9 |
| SARS-CoV-2 diagnosis | N | % |
| RT-PCR for SARS-CoV-2 on Pharyngeal/ Nasopharyngeal Swab | 260 | 95 |
| IgM | 6 | 2 |
| IgG | 9 | 3 |
| Laboratory findings | N | % |
| Total pregnant women with data | 108 | 39 |
| Missing data | 167 | 61 |
| Lymphopenia (<1000/mmc) | 31 | 29 |
| Elevated CRP (>10 mg/L) | 52 | 48 |
| Elevated ALT (>45 U/L) or AST (>35 U/L) | 9 | 8 |
| Chest CT | N | % |
| Total pregnant women with data | 171 | 62 |
| Missing data (not reported/not done) | 104 | 38 |
| Positive | 162 | 95 |
| Negative | 9 | 5 |
| Chest X-ray | N | % |
| Total pregnant women with data | 48 | 17 |
| Missing data (not reported/not done) | 227 | 83 |
| Positive | 48 | 100 |
| Negative | 0 | 0.0 |
| Symptoms Before Delivery and Age | Mean | SD |
| Symptoms Before Delivery | 31.06 | 3.61 |
| Age | 9.26 | 8.96 |
| Study | N | Symptoms Onset/ Diagnosis | Isolation * | Breast-Feeding * | GA | Birth-Weight | Sars-CoV-2 Positive Swab | Symptoms | Laboratory Test | Imaging | Length of Hospitalization/Symptoms |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Paret M | 1 | 25 days | / | / | 39 | Not reported | NP | Fever | Normal | Not reported | Not reported |
| Han MS | 1 | 27 days | / | / | 38+6 | 3730 | NP | Fever, mild respiratory symptoms | Normal | X-ray Normal | 18 days |
| Diaz CA | 1 | 8 days | / | / | 38+4 | 2500 | NP | Distress | Normal (only CRP reported) | X-ray: ground glass opacities | Not reported |
| Kamali Aghdam M | 1 | 15 days | / | / | Not reported | 3460 | NP | Fever, distress, need for noninvasive respiratory support | Normal | X-ray: normal | 6 |
| Wang J | 1 | 19 days | / | / | 38+6 | 3030 | NP/Anal | Fever, gastrointestinal symptoms, cough | Thrombocytopenia | X-ray: positive, CT increased lungmarking | 14 |
| Zeng LK | 1 | 17 days | / | / | 39 | Not reported | NP | Fever, gastrointestinal symptoms (vomit, diarrhea) | lymphocytosis | Cranial, abdomen CT: negative. Chest CT: positive. X-ray: positive | 6 |
| Zhang ZJ | 1 | 17 Days | / | / | ≥37 | Not reported | Anal | Fever, cough, gastrointestinal symptoms (vomit) | Not reported | CT chest: increased lungmarking | 23 |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | 40 | Not reported | NP | Distress | Not reported | CT chest: increased lungmarking | Not reported | |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | ≥37 | Not reported | Anal | Fever | Not reported | Not reported | 30 | |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | 40 | Not reported | NP | No symptoms | Not reported | CT chest: Increased lung marking | 16 | |
| Zeng L | 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | 40 | 3250 | NP | Fever | Normal | X-ray: pneumonia | 2 (ICU) |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | 40+4 | 3360 | NP | Fever | leukocytosis, lymphocytopenia, and elevated creatine kinase–MB fraction | X-ray: pneumonia | 4 (ICU) | |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | 32+2 | 1580 | NP | Distress, refuse of feeding, need for mechanical ventilation | leukocytosis, thrombocytopenia, sepsis | X-ray: RDS and pneumonia | 11 (ICU) | |
| Ferrazzi E | 1 | Mothers’ COVID 19 diagnosis a few hours after delivery | No ° | Yes | Not reported | Not reported | NP | Not reported | Not reported | Not reported | Not reported |
| 1 | Mothers’ COVID 19 diagnosis a few hours after delivery | No ° | Yes | Not reported | Not reported | NP | Not reported | Not reported | Not reported | Not reported | |
| 1 | After birth (mother Sars-CoV-2 + during pregnancy) | Yes | No | Not reported | Not reported | NP | Gastrointestinal symptoms, distress requiring one-day mechanical ventilation | Not reported | Not reported | ICU admission for prematurity/respiratory distress |
| Neonatal Characteristics | ||
|---|---|---|
| Total neonates | 248 | |
| Stillborn neonates | 2 | |
| Neonatal Characteristics | Mean | SD |
| Birthweight (g) | 2914 | 573 |
| Gestational age | N | % |
| Neonates with data | 196 | 79 |
| <37 weeks | 54 | 28 |
| ≥37 weeks | 142 | 72 |
| Apgar score | N | % |
| Neonates with data | 190 | 77 |
| <7 at 5’ * | 5 | 3 |
| >7 at 1’ and/or at 5’ | 185 | 97 |
| >7 at 1’ | 145 | 76 |
| (* 2 stillborn were included, the Apgar score was reported). | ||
| Feeding * | N | % |
| Neonates with data | 56 | 23 |
| Breastfeeding | 13 | 23 |
| Formula | 38 | 68 |
| Both | 5 | 9 |
| Isolation | N | % |
| Neonates with data | 171 | 70 |
| Yes | 125 | 73 |
| No* (1 was isolated after 4 days, CA Diaz) | 46 | 37 |
| Symptoms | N | % |
| Neonates with data | 160 | 65 |
| Fever | 13 | 8 |
| SARS-CoV-2 + | 9 | 70 |
| Mild respiratory symptoms (cough; rhinorrhea) | 4 | 3 |
| SARS-CoV-2 + | 3 | 75 |
| Distress | 21 | 13 |
| SARS-CoV-2 + | 5 | 24 |
| Gastrointestinal symptoms | 13 | 81 |
| SARS-CoV-2 + | 5 | 38 |
| Complications | N | % |
| Need for respiratory support | 8 | 5 |
| SARS-CoV-2 + | 3 | 38 |
| Other complications | N | % |
| Asphyxia | 2 | 13 |
| Asphyxia in SARS-CoV-2 + | 1 | 50 |
| Sepsis | 1 | 0.6 |
| SARS-CoV-2 + | 1 | 100 |
| Death or stillbirth | 3 | 1 |
| Stillbirth | 2 | 0.8 |
| Death | 1 | 0.4 |
| SARS-CoV-2 diagnosis | N | % |
| RT-PCR nasopharyngeal swab | ||
| Neonates with data | 191 | 78 |
| Positive * | 14 | 7 |
| * RT-PCR-positive on fecal samples only | 2 | 1 |
| RT-PCR on fecal samples or anal swabs | N | % |
| Neonates with data | 28 | 15 |
| Positive | 5 | 18 |
| RT-PCR breast milk | N | % |
| Neonates with data | 25 | 10 |
| Positive | 0 | 0 |
| Other samples (maternal vaginal swab, placenta tissue, cord blood or amniotic fluid) | N | % |
| Neonates with data | 35 | 14 |
| Positive | 0 | 0 |
| Serological test | N | % |
| Neonates with data | 26 | 10 |
| Negative | 19 | 73 |
| Positive IgG | 4 | 15 |
| Positive IgG+ IgM | 3 | 12 |
| Laboratory findings | N | % |
| Neonates with data | 79 | 32 |
| SARS-CoV-2 + with data | 7 | 44 |
| Imaging | N | % |
| Neonates with data | 76 | 31 |
| Chest CT | 5 | 3 |
| Chest CT in SARS-CoV-2+ | 4 | 80 |
| Chest CT positive SARS-CoV-2 + | 4 | 100 |
| Chest X-ray | 70 | 92 |
| Chest X-ray in SARS-CoV-2 + | 8 | 50 |
| Chest X-ray positive in SARS-CoV-2 + | 6 | 75 |
| Both X-ray and Chest CT | 2 | 3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trippella, G.; Ciarcià, M.; Ferrari, M.; Buzzatti, C.; Maccora, I.; Azzari, C.; Dani, C.; Galli, L.; Chiappini, E. COVID-19 in Pregnant Women and Neonates: A Systematic Review of the Literature with Quality Assessment of the Studies. Pathogens 2020, 9, 485. https://doi.org/10.3390/pathogens9060485
Trippella G, Ciarcià M, Ferrari M, Buzzatti C, Maccora I, Azzari C, Dani C, Galli L, Chiappini E. COVID-19 in Pregnant Women and Neonates: A Systematic Review of the Literature with Quality Assessment of the Studies. Pathogens. 2020; 9(6):485. https://doi.org/10.3390/pathogens9060485
Chicago/Turabian StyleTrippella, Giulia, Martina Ciarcià, Marta Ferrari, Chiara Buzzatti, Ilaria Maccora, Chiara Azzari, Carlo Dani, Luisa Galli, and Elena Chiappini. 2020. "COVID-19 in Pregnant Women and Neonates: A Systematic Review of the Literature with Quality Assessment of the Studies" Pathogens 9, no. 6: 485. https://doi.org/10.3390/pathogens9060485