Article Text

Abstract
Background Existing research has found a positive association between cognitive function and residence in a socioeconomically advantaged neighbourhood. Yet, the mechanisms underlying this relationship have not been empirically investigated.
Objective To test the hypothesis that neighbourhood socioeconomic structure is related to cognitive function partly through the availability of neighbourhood physical and social resources (eg, recreational facilities, community centres and libraries), which promote cognitively beneficial activities such as exercise and social integration.
Methods Using data from a representative survey of community-dwelling adults in the city of Chicago (N=949 adults aged 50 and over), cognitive function was assessed with a modified version of the Telephone Interview for Cognitive Status instrument. Neighbourhood socioeconomic structure was derived from US census indicators. Systematic social observation was used to directly document the presence of neighbourhood resources on the blocks surrounding each respondent's residence.
Results Using multilevel linear regression, residence in an affluent neighbourhood had a net positive effect on cognitive function after adjusting for individual risk factors. For white respondents, the effects of neighbourhood affluence operated in part through a greater density of institutional resources (eg, community centres) that promote cognitively beneficial activities such as physical activity. Stable residence in an elderly neighbourhood was associated with higher cognitive function (potentially due to greater opportunities for social interaction with peers), but long term exposure to such neighbourhoods was negatively related to cognition.
Conclusions Neighbourhood resources have the potential to promote ‘cognitive reserve’ for adults who are ageing in place in an urban setting.
- Cognitive function
- neighbourhood
- urban health
- elderly
- cognitive problems
- multilevel models
- social epidemiology
Statistics from Altmetric.com
- Cognitive function
- neighbourhood
- urban health
- elderly
- cognitive problems
- multilevel models
- social epidemiology
Introduction
Dementia is a common and disabling brain disorder among older adults that has consequences for independence, functional decline, institutionalisation and mortality.1–3 The key feature of dementia is a decline in cognitive function, including impairments in memory, attention and executive function. There is growing evidence that risk factors at both the individual and community levels are related to cognitive function.
At the individual level, evidence has been accumulating that hypertension, obesity, diabetes and heart disease are risk factors for cognitive impairment and dementia, in part through pathways such as chronic inflammation and oxidative stress.4 Conversely, physical activity (particularly frequent or vigorous physical activity) and adherence to a Mediterranean-type diet have been found to be protective against cognitive decline,5–9 likely a result of decreased vascular inflammation. At the same time, social interaction and integration within a social network are associated with a lower incidence of dementia,10–12 potentially due to greater opportunities to engage in healthy behaviours or the increased mental stimulation afforded by integration within a supportive social network. Similarly, individuals with more formal years of education have a reduced risk of dementia,13 ,14 at least partly as a result of similar underlying pathways. Collectively, these findings have contributed to the ‘cognitive reserve’ hypothesis,15 which suggests a direct effect of mental stimulation or physical activity on brain development and function that mitigates cognitive decline either through neural reserve (pre-existing brain networks have more capacity and are therefore less susceptible to decline) or neural compensation (capacity to activate alternate networks to compensate for pathological disruption).
Recently, a parallel literature has begun to examine the relationship between cognitive function and characteristics of the surrounding environment using secondary data sources (eg, decennial census) linked to individual survey respondents. This research has shown that, controlling for individual socioeconomic resources, living in an area with a high proportion of adults with low levels of education is associated with lower cognitive function among American older adults.16 This effect was particularly pronounced for older adults with the least education,16 highlighting the importance of incorporating cross-level interactions to consider questions of ‘person–environment fit’ for potentially vulnerable subpopulations.17 Similar findings have been found in the UK, where neighbourhood socioeconomic deprivation (eg, high proportion of low income, unemployed and lower educated residents) was associated with decreased cognitive function (although no cross-level interactions were found).18 Using longitudinal data for older Mexican Americans, Sheffield and Peek19 found that, net of individual socioeconomic status, residence in an economically advantaged area (eg, high household income) was associated with slower rates of cognitive decline over a 5-year period.
Authors of these papers have speculated that living in highly educated and socioeconomically advantaged neighbourhoods may promote cognitive function and/or buffer cognitive decline in part through their greater density of physical resources (recreational centres, gyms, parks, walking paths, healthy food stores) as well as social and institutional resources (libraries, bookstores, community centres, social clubs)16 ,19 that promote protective health behaviours (eg, physical activity) and facilitate mental stimulation (eg, social interaction and cognitive activities such as reading and/or playing games). However, to date these hypothetical pathways have not been empirically tested.
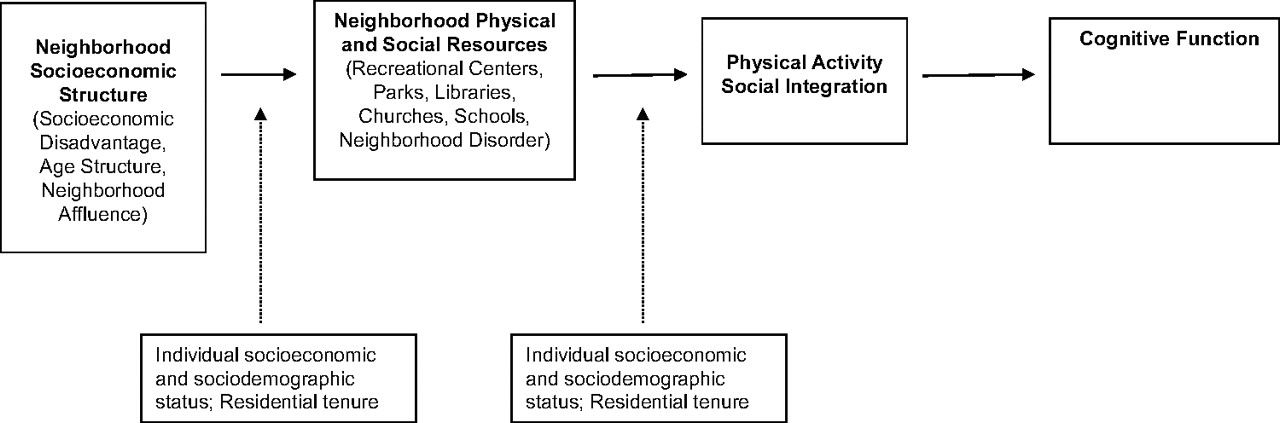
In this paper we explicitly test the hypothesis that neighbourhood socioeconomic structure is associated with the prevalence of neighbourhood physical and social resources, which in turn are associated with the frequency of physical and social activities of individuals in these environments, and resulting levels of cognitive function (figure 1). Following the existing literature16 we also test for cross-level interactions between neighbourhood context and individual socioeconomic and sociodemographic position, hypothesising that contextual composition or resources may be particularly salient for individuals at highest risk for cognitive impairment (eg, older adults, racial/ethnic minorities, or those from lower socioeconomic position). Contextual effects may also vary by duration of exposure to particular neighbourhoods, as reflected by cross-level interactions with residential tenure.

{kind=link}
Hypothesised pathways in the relationship between neighbourhood socioeconomic structure and cognitive function, including cross-level interactions (dotted lines).
We test these hypotheses using a large representative survey of Chicago residents 50 years of age and older with a rich array of data on neighbourhood characteristics. Consistent with the existing literature we focus on indicators of neighbourhood socioeconomic disadvantage (typically captured through the proportion of residents in poverty, on public assistance and unemployed) and examine its impact on cognition through the shortage of physical (eg, recreational centres, parks) and institutional (eg, libraries, churches, schools) resources in each neighbourhood, as well as through indicators of neighbourhood social and physical disorder (eg, visual signs of decay, crime). We also examine the effects of neighbourhood age structure, speculating that cognitive function is better when living in an area with a higher proportion of older adults, in part through increased opportunities for social interaction with peers or a greater density of age-specific resources (eg, senior centres). We also go beyond examining the effect of disadvantaged neighbourhoods to consider the effects of affluent neighbourhoods,20 ,21 which are distinguished by the demographic profile associated with gentrification (eg, highly educated, young adults, working in professional occupations), and likely to attract a set of institutions and resources conducive to cognitive health (eg, places to exercise, well maintained buildings and parks). Consistent with the existing literature we focus on two mediators of these environments among individuals, levels of physical activity and social integration, and we control for a broad array of individual socioeconomic and sociodemographic characteristics that could confound the relationships under study.
Methods
Data
Data come from the Chicago Community Adult Health Study conducted in 2002 through face-to-face interviews with a multi-stage representative sample of 3105 adults aged 18 and over, living in all 343 neighbourhood clusters in the city of Chicago.22 A response rate of 72% is one of the highest in a major American city in recent decades.23 The weighted sample matches the 2000 census population estimates for the city of Chicago in terms of age, race/ethnicity and gender. To focus on the age group most at risk for the development of cognitive impairment,2 we restrict our analyses to 949 adults aged 50 and over. All study procedures were reviewed and approved by the University of Michigan's Institutional Review Board and study participants gave informed consent.
Outcome measure
Cognitive function was assessed using a modified version of the Telephone Instrument for Cognitive Status (TICS).24 A composite index was derived from five tasks assessing memory, orientation and executive functioning: (a) an immediate word recall test of 10 common nouns (10 points); (b) a delayed recall test of the same 10 nouns approximately 5 min later (10 points); (c) naming the day of the week and the date (2 points); (d) naming the current president of the USA and the past president (2 points); and (e) a serial 3s test that required subtracting 3 from 20 six times (1 point). A summary score was created by summing the number of correct answers (max=25), with a higher score indicating better cognitive function. Refusals to answer any question were coded as incorrect.
Neighbourhood measures
We include indicators from the US census using the census tract as a proxy for neighbourhood. Census tracts have on average about 4000 people and are designed to capture homogenous areas that roughly map to neighbourhoods.25 Each respondent's address was geocoded to the 2000 census tract, and linked to the US decennial census for that year. We focus on three indices of neighbourhood social and economic structure. The age structure of a tract is captured through the proportion of persons in each tract who are aged 65 and older. Neighbourhood socioeconomic disadvantage is an average of six census indicators: per cent of households with income less than $15 000 annually, per cent of households with incomes over $50 000 annually (reverse coded), per cent of working age adults who are unemployed, per cent of families in poverty, per cent of households on public assistance income, and per cent of female-headed families. Neighbourhood affluence is an average of four census indicators: per cent of adults with college degrees or higher, per cent of adults in professional or managerial occupations, per cent of adults aged 30–39 years, and median home value (expressed as a percentage of the maximum median home value in all sampled census tracts). Factor loadings for the items in the socioeconomic indices range from 0.82 to 0.95 (disadvantage) and from 0.71 to 0.99 (affluence); corresponding α reliabilities=0.95 and 0.90, respectively.
Neighbourhood resources
In addition to census indicators we draw on a rich source of data on neighbourhood resources. The Chicago Community Adult Health Study was specifically designed to examine the relationship between neighbourhoods and health, and observational data were collected on the city block around each respondent's residence through the method of systematic social observation.26 ,27 Systematic social observation capitalises on the interviewer's visit to the home to directly measure the physical and social conditions of the block during the day. While walking around the residential block where each respondent lives, the survey interviewer characterised these respondent-centred neighbourhoods using a standardised instrument. Inter-rater reliability of this method was demonstrated using a subsample of 80 blocks in a pilot study conducted in 2001 where two raters made separate, independent observations of the same block at the same time (agreement=0.78 to 1.00; κ=0.27 to 0.91).
We constructed tract-level measures of neighbourhood resources from these block level observations, including the proportion of blocks within the tract where there are public recreational centres (eg, gyms, swimming pools, or buildings where residents can exercise and play sports) as well as institutions such as schools, churches, libraries and community centres that provide opportunities for social interaction or intellectual stimulation. An index of neighbourhood disorder27 (capturing social and physical disorder that may discourage residents from accessing resources in their neighbourhood) is derived from observations of the block with respect to the presence of graffiti, garbage, litter or broken glass, cigarette butts, empty beer/liquor bottles, abandoned cars, and drug-related paraphernalia or condoms on sidewalks or in street gutters, that are aggregated to the tract level using multilevel item response models to create an overall measure expressed on a logit scale (ranging from negative to positive), with a high score indicating a high presence of disorder (α reliability=0.935). In addition, we draw on geographic data from the city of Chicago to create a measure of park area in square miles in each census tract. We include indicators for each respondent's length of residence at current address in order to capture duration of exposure to these environments.
Individual mediators
We focus on two potential mediators of neighbourhood resources at the individual level. First, social integration is assessed by the frequency of getting together with friends, neighbours and relatives, either going out together or visiting in each other's homes (measured on a 6-point scale ranging from 0 to 5: never, less than once per month, once per month, 2 or 3 times per month, once a week, more than once a week). Respondents were also asked to indicate whether they participated in community or civic activities within the past year (eg, worked on a community project, attended a community meeting). A binary variable for civic engagement indicates whether the respondent participated in any such activity in the past year.
Second, respondents were also asked to report on their physical activity habits in a typical week over the past 12 months. Using questions from the National Health Interview Survey,28 respondents were asked about ‘physical activities such as exercise, sports, or physically active hobbies that you do in your leisure time and that cause you to sweat or increase your breathing or heart rate’. Activities were classified as either light to moderate (light or moderate activities for at least 10 min that cause only light sweating or a slight to moderate increase in breathing or heart rate; walking continuously for 20 min or more; home maintenance such as painting or outside yard work, including gardening and shovelling snow) or vigorous (engaging in activities for at least 10 min that cause heavy sweating or large increases in breathing or heart rate). Following Scarmeas et al,8 a three category summary physical activity variable was constructed based on the frequency and intensity of activities: no physical activity (no walking, exercise, sports or physically active hobbies); some physical activity (light to moderate physical activity once per week or less regardless of duration, light to moderate activity 2–3 times per week for 20 min or more, light to moderate activity four or more times per week for less than 20 min, vigorous activity once per week or less for 20 min or more, walking once per week or less for 20 or more minutes, or working around the house 1–3 times per week); and heavy physical activity (light to moderate activity four or more times per week for 20 min or more, vigorous activity two or more times per week regardless of duration, walking 20 min or more two or more times per week, or working around the house four or more times per week).
Individual controls
We control for key sociodemographic and health factors that could account for the relationships between cognitive function and neighbourhood characteristics. Sociodemographic factors include age, gender, marital status, race/ethnicity, employment status and socioeconomic position. Age is represented by two dummy variables contrasting young-old (age 60–69) and very old adults (age 70+) with middle-age adults (age 50–59). Gender is a dummy variable coded 1 for males and 0 for females. Marital status is captured by three dummy variables contrasting divorced/separated, widowed and never married, with married respondents. Race/ethnicity is categorised according to three dummy variables contrasting black, Hispanic and other race/ethnicity (including Native American, Asian or Pacific Islander) with whites. Employment status is captured using three dummy variables contrasting the unemployed, retired (or unable to work because of a health problem) and homemakers, with employed respondents. Socioeconomic position is assessed through the respondent's level of education (classified as less than high school, high school diploma or college degree) and reported household income (captured with two dummy variables contrasting those with annual incomes less than $15 000 and $15–40 000 with those whose annual incomes are over $40 000; a dummy variable indicates missing data on income). We also control for underlying physical health status using an index of self-reported chronic health problems that sums the number of medically diagnosed health conditions (eg, hypertension, heart attack, stroke, arthritis, diabetes, peripheral artery disease). (Additional controls for smoking, body mass index, depressive symptoms, living arrangements and immigrant status were also considered (results not shown), but did not change the results reported here.)
Statistical analysis
To account for the clustering of observations within census tracts (mean=2.1 respondents per tract, range=1–11)29 we used multilevel linear regression to examine the effect of neighbourhood characteristics on cognitive function. Analyses were performed with the MIXED procedure in SAS V.9.2 and the neighbourhood variables were grand mean centred with an SD of one.30 Statistical significance was assessed with a two-tailed α of 0.05 and all models were weighted by post-stratification sample weights to account for the sampling design as well as differential coverage and non-response across neighbourhood clusters.
Results
Descriptive statistics for the study sample are presented in table 1. Average scores on the cognitive function measure fall at the midpoint of the scale (range 2–24) and the overall distribution of the scores follows a normal distribution. Respondents visit with friends and neighbours about once a week on average, and about half have participated in a community activity in the past year. Two-thirds engage in some physical activity in a typical week, while 12% are not physically active. Respondents tend to be long term residents of their neighbourhoods, with over half residing at their address for 10 years or more.
Descriptive statistics for study sample (N=949); Chicago Community Adult Health Study (age 50+)
Table 2 presents the results from the multilevel linear regression models. The first column (model A) reports the results for the unconditional (intercept only) model. There is significant variation in cognitive function across census tract neighbourhoods (variance components for the intercept, p<0.001), with almost 30% of the total variation in cognitive function lying between tracts (intraclass correlation coefficient (ICC)=0.29). The second column (model B) in table 2 adds the neighbourhood census indicators and, as hypothesised, neighbourhood socioeconomic disadvantage is associated with worse cognitive function while neighbourhood affluence is associated with better cognitive function (a 1 SD increase in neighbourhood affluence is associated with almost a one point increase on the cognitive function measure).
Effects of neighbourhood characteristics, controls and mediators on cognitive function; Chicago Community Adult Health Study, age 50+ (N=949)
The third column of table 2 (model C) adds the individual control variables that could account for the relationship between neighbourhood census characteristics and cognitive function if, for example, individuals with more risk factors for lower cognitive function (eg, health problems, lower education) tend to live in areas characterised by neighbourhood socioeconomic disadvantage. Indeed, the negative effect of living in a disadvantaged neighbourhood is completely explained by the addition of the control variables, but a net positive effect of neighbourhood affluence on cognition remains. The effects of neighbourhood age structure become statistically significant after adjusting for the controls, but the effects vary by duration of residence in the neighbourhood as indicated by significant cross-level interactions with residential tenure. As hypothesised, residence in an area with a higher proportion of older adults was positively associated with cognitive function, but only for those with more stable exposures to these neighbourhoods (tenure of 6–10 years), and was negatively associated with cognition for very long term residents of these types of neighbourhoods (more than 10 years). (Other cross-level interactions involving sociodemographic or socioeconomic variables were not statistically significant.) Results from model C also illustrate notable gender, racial/ethnic and socioeconomic disparities in cognition. Males, non-whites, and those with less than a college education have significantly lower cognitive function scores, net of the effects of income and health status. Widowhood, retirement and being a homemaker are also associated with worse cognitive function.
Model D in table 2 adds the neighbourhood resources that were hypothesised to explain the effect of neighbourhood socioeconomic structure on cognition. We found no effect of the proportion of recreational centres or park area in one's neighbourhood, but living in a neighbourhood with a higher density of institutional resources (such as libraries, schools and community centres) was associated with higher cognitive function scores, net of individual resources. However, this benefit was reserved only for white respondents. Exposure to greater institutional resources was negatively associated with cognitive function for African Americans (and negatively but not significantly for Hispanic adults). Institutional resources account for almost half of the adjusted effect of neighbourhood affluence on cognition ((0.28–0.15)/0.28=0.46, model C to model D), effectively explaining the statistical significance of the positive affluence effect. Neighbourhood resources did not explain any of the effects of neighbourhood age structure on cognitive function.
Models E and F in table 2 add the physical activity and social integration variables to try to explain the adjusted effects of neighbourhood resources on cognitive function. Vigorous physical activity (model E) was positively associated with cognition, explaining a small part (4%) of the positive effect of institutional resources for white respondents ((1.81–1.73)/1.81=0.04, model D to model E). Social integration was strongly and positively associated with higher cognitive function (model F), but did not account for any of the effects of neighbourhood institutions (although social integration explained a marginal part of the positive effect of neighbourhood age structure among those living in elderly neighbourhoods between 6 and 10 years, model D to model F). Results from model F also indicate that some of the social disparities in cognition are a function of fewer opportunities for social engagement among the less educated, homemakers and men. At this point these analyses have explained 33% of the variance in cognitive function in our sample by including a range of individual and neighbourhood characteristics (R2=0.33, model F). But significant variation in cognition remains between neighbourhoods (ICC=0.21, model F), suggesting that other unmeasured factors at the neighbourhood and/or individual level remain to be accounted for.
Discussion
Using data from a large representative sample of older Chicago adults, we tested the complex pathways in the relationship between neighbourhood characteristics and cognitive function. Similar to other studies16 ,19 we found significant variation in cognitive function across neighbourhoods at a level that is rarely seen in the literature on neighbourhoods and health,31 suggesting that neighbourhood characteristics may be a source of unexplored differences in cognitive function across adults living in different settings. We also replicated the findings that neighbourhood socioeconomic disadvantage is related to cognition.16 ,18 ,19 However, we went beyond the current literature by examining the effects of neighbourhood affluence on cognition in addition to disadvantage, and modelled the mediating effects of neighbourhood resources and individual behaviours to explain the effects of neighbourhood socioeconomic structure.
Whereas the negative effects of neighbourhood disadvantage were effectively explained by common factors that both increase the risk of cognitive decline as well as select people into disadvantaged neighbourhoods, neighbourhood affluence had a net positive association with cognitive function that operated in part through a greater density of institutional resources such as community centres, schools and libraries. However, the cognitive benefits of institutional resources were found only for white respondents, while a greater density of neighbourhood institutions was negatively associated with cognitive function for African American and Hispanic respondents. This negative association suggests that neighbourhood institutional resources hypothesised to promote cognitive function16 ,19 might have less benefit among racial and ethnic minority groups if language or cultural barriers prevent full access to opportunities offered within these institutions.
The positive relationship between institutional resources and cognition among white respondents was partly explained by physical activity, suggesting that resources such as community centres and senior centres may provide white older adults with the opportunity to exercise, which has been found to have positive consequences for cognitive function (vascular hypothesis).32 By empirically examining this conceptual sequence, we show that neighbourhood affluence (and the greater density of institutional resources in these areas) has the potential to act as a source of ‘cognitive reserve’, particularly for white adults who are ageing in place in an urban setting.
Contrary to our expectations, a greater density of recreational centres and park area were not associated with cognitive function, suggesting the need to examine alternate indicators of neighbourhood resources that could promote cognitively beneficial physical activity. While social interaction was strongly and positively related to cognitive function, it did not account for any of the effects of institutions in our data. We also examined the effects of neighbourhood age structure, speculating that cognitive function would be better when living in an area with a higher proportion of older adults, in part through increased opportunities for social interaction with peers as well as the exchange of information about resources and services.33 ,34 As hypothesised, residence in an area with a higher proportion of older adults was positively associated with cognitive function for those with more stable exposures to these neighbourhoods (residence over 5 years) but was negatively associated with cognition for very long term residents of these types of neighbourhoods (more than 10 years). While a stable period or exposure to neighbourhoods with a higher proportion of older adults may provide opportunities for more peer group interaction33 ,34 (although our measure of social interaction was only marginally able to detect any mediating effect), prolonged exposure to older adult neighbourhoods may reflect a collective ageing in place that is associated with structural decline,35 with adverse consequences for cognitively healthy behaviours.
Limitations
This study was limited to older adults living in the city of Chicago, and the findings may not be generalisable to other urban centres. Further studies in other settings are needed to investigate these relationships further. Measures of physical activity and social integration were based on self-report, which may have limited the strength of their association with cognitive function. Cross-sectional data also preclude an understanding of the direction of association between variables, and we are unable to rule out reciprocal causation. However, our capacity to examine the impact of the urban environment on cognitive function was considerably enhanced by using independent observational measures of the neighbourhood characteristics that adults encounter in their day-to-day lives.
In summary, these findings emphasise the importance of considering urban design for the cognitive health of older adults who are ageing in place. Although people with dementia may be concentrated in institutions, the majority of older adults with dementia live in the community.36 Our results stress the importance of intelligent design of outdoor environments for individuals at risk for cognitive decline.37 ,38
What is already known on this subject
Existing research to date has speculated that living in highly educated and socioeconomically advantaged neighbourhoods can promote cognitive function and/or buffer cognitive decline in part through their greater density of physical resources (recreational centres, gyms, parks, walking paths, healthy food stores) as well as social and institutional resources (libraries, bookstores, community centres, social clubs) that promote protective health behaviours (eg, physical activity) and facilitate mental stimulation (eg, social interaction and cognitive activities such as reading and/or playing games).
To date these hypothetical pathways have not been empirically tested.
What this study adds
Using representative data from a cross-sectional survey of community dwelling older adults, this study examined the complex pathways in the relationship between neighbourhood socioeconomic structure and cognitive function.
Residence in an affluent neighbourhood had a net positive effect on cognitive function after adjusting for individual risk factors.
For white respondents, the effects of neighbourhood affluence operated in part through a greater density of institutional resources (eg, community centres) that promote cognitively beneficial activities such as physical activity.
Stable residence in an elderly neighbourhood was associated with higher cognitive function (potentially due to greater opportunities for social interaction with peers), but long term exposure to such neighbourhoods was negatively related to cognition.
Neighbourhood resources have the potential to promote ‘cognitive reserve’ for adults who are ageing in place in an urban setting.
References
Footnotes
The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the sponsors. An earlier version of this paper was presented at the Annual Meeting of the Gerontological Society of America, Atlanta, Georgia, November 2009.
Funding This study was funded by the National Institutes of Health NIH/NICHHD Grant RO1HD050467. PJC was supported by the Centers for Disease Control and Prevention (Grant Number K01EH000286-01). KML was supported by NIH/NIA Grant R01 AG027010.
Competing interests None.
Ethics approval This study was conducted with the approval of the University of Michigan IRB.
Provenance and peer review Not commissioned; externally peer reviewed.