Article Text

Abstract
More than 30 years ago, the older of us published a paper with the proposal that all scientific papers should start with a statement along the lines of: “These are the opinions on which I base my facts”. Why pretend? To take a topical example, if you are on the nature side of the nature/nurture debates, is it likely that your next paper will be an apologia: “I take it all back; genes don’t matter at all; it is all environment”? Unlikely. Similarly, if you are on the other side. (We know. It’s both.) Here, we are not in any way arguing for a relativist credo that would say opinions are all. Along with other readers of this journal, we spend a good part of our working lives gathering, analysing and interpreting empirical evidence. Evidence matters. But everyone has values and they do affect our positions.
Statistics from Altmetric.com
Relevant to the matter at hand, we have a core value that says that systematic social differences in health that are judged to be avoidable are unfair, inequitable.1 Putting these inequities in health right is a matter of social justice. This was the guiding principle that underlay the Commission on Social Determinants of Health (hereafter the Commission).2 The Commission was set up by the former Director-General of the World Health Organization (WHO), J W Lee, to marshal the scientific evidence in order to lay the basis for action on social determinants of health.
If all that was needed was an affirmation of values, the Commission could have had one teleconference and declare for fairness. Yes, the values told us that avoidable health inequalities, health inequities, were wrong. But what was needed was a set of recommendations on how to put them right. That took a review of the evidence. In this commentary, we want to discuss the approach we took to evidence, but the importance of values should not be underestimated.
We stated quite explicitly that tackling health inequities is not simply a technical matter, it is an ethical pursuit. This elicited strong reactions when the Commission’s report was published on 28 August 2008.3 The Economist newspaper showed that they had read the report carefully but criticised us for putting equity in centre stage. The Lancet praised us for putting equity in centre stage.
At various points in the Commission’s life, the point was put to us strongly that, for the Commission’s recommendations to be taken seriously, we had to show that taking action on health equity would be good for the economy. A previous WHO Commission, on Macroeconomics and Health, had argued for massive investment in disease control in order to promote economic development.4 Many people thought that anything that led the international community to invest in disease control had to be applauded. It is also encouraging to see more recent arguments that health is good for the economy5 and health inequalities are particularly costly.6
But the Commission did not revisit this territory. Our starting position was the social determinants of health—social included economic—not the health determinants of economics. Our conclusion was, not surprisingly, informed by all that we learnt through the three and a half years of the Commission’s extensive work: health inequities arise because of a toxic combination of poor social policies, unfair economic arrangements and bad politics. These, in turn, affect the circumstances in which people are born, grow, live, work and age. This second position—that social circumstances lead to health rather than health leads to social circumstances—was not just a value but a judgement derived from decades of research. The Black Report set it out clearly in the 1980s; so did William Farr nearly a century and a half earlier; so, come to think of it, did Hippocrates.
By setting out our stall explicitly, commentators could know where we stand. If, like The Economist, these prior positions are simply too much excess ethical baggage, they can treat our report accordingly. To quote The Economist: “it would be a pity if the new report’s saner ideas were obscured by the authors’ quixotic determination to achieve perfect political, economic and social equity”.7 If commentators agree with our starting position, there is still the question: what can be done about it and how to go about doing it. Hence the Commission’s process of gathering, sifting and passing judgements on evidence and formulating recommendations.
THE COMMISSION ON SOCIAL DETERMINANTS OF HEALTH: CORE CONCERNS
We were concerned with inequities in health within and between countries, and the disadvantage arising from ill-health. It needed to be repeated that improvement of the overall health of a society was a major societal achievement, as was reduction in inequities within society. That these are two major goals bore repeating because of the often made comment that one way of achieving greater equity in health is to stop the better off from improving. The aim, of course, is for everyone’s health to improve and for the gap in health to be reduced.
The third concern, to reduce the disadvantage due to ill-health, helped deal with another tension. In many quarters, people equate inequities in health with inequities in healthcare. The purpose of the Commission was, true to its title, to address the social determinants of health. Healthcare is important, of course, when people get sick. Health systems were well within the purview of the Commission, and we took the view that health systems are among the social determinants of health; predominantly, not exclusively, because they deal with disadvantage resulting from ill-health.
Two headlines captured attention when we published the report. The first was the contrast between life expectancy of 43 for a woman in Zambia compared with 86 for a woman in Japan. We said that there is no necessary biological reason why there should be a 43 year span in life expectancy across the world. The second, which caused a media feeding frenzy in the UK, was the 28 year life expectancy gap between men in Calton in Glasgow and men in Lenzie 13 km away. These extremes are, indeed, shocking, but the more fundamental point was that health and disease follow the social gradient (fig 1). What had been observed in rich countries was widely seen in low- and middle-income countries.8

The implications of the gradient are profound. Much attention, globally, on health inequities has focused on the poorest of the poor. In population-attributable risk terms, however, much of the ill-health attributable to lower socioeconomic position is not confined to the bottom 10%. This implies interventions that affect the whole of society not only those at the bottom.
WHAT CONSTITUTES EVIDENCE?
There has long been debate within epidemiology between well-done analytical studies and randomised controlled trials. Can one draw conclusions about causation, and the likely benefits of interventions, from observational studies? If in that debate you think the only evidence worth considering is that from randomised controlled trials, you can happily save time by not reading our report. We describe the social determinants of health as the circumstances in which people are born, grow, live, work and age; and the inequitable distribution of power, money and resources that are drivers of those circumstances of daily life. It will not take long to assemble all the randomised controlled trials of the health effects of income redistribution in sub-Saharan Africa; or to conduct a systematic review of the effects on health equity of social protection mechanisms in Latin America; or the effect of trade agreements on life expectancy in low-income countries.
Many people within the Commission, like many epidemiologists, have spent their research lives on analytical epidemiological studies isolating causal effects. Traditionally, case studies, action research, qualitative studies, descriptive studies were seen as not quite up to this purpose. Striving to produce a report and set of evidence-based recommendations about what could be done to improve global health equity, the Commission had to take a fit-for-purpose approach to evidence, balancing the use of different types of evidence, and assessed the degree to which action in social determinants of health was shown to be possible and effective. Given the global reach of the Commission, and that some countries do not even have vital registration systems let alone a tradition of population health research, laying a reasoned basis for action required such an open approach to evidence. We also applied chains of reasoning. For example, suppose one poses the question: is collective action, at the grassroots level, good for health? If it can reasonably be shown that collective action can lead to improved housing and employment conditions, and given that a wealth of evidence points to the importance of housing and employment conditions for health, it is a reasonable supposition that collective action to improve housing and employment will be beneficial for health equity.
To illustrate the power, and necessity, of diversifying the evidence base, let’s take one area in which the Commission makes recommendations—early child development. A randomised control trial, undertaken by Walker and colleagues10 in Kingston, Jamaica, provided nutritional supplementation and psychosocial stimulation to a group of stunted children aged 9–24 months. They also assessed non-stunted children. Reassessing all participants almost 18 years later, the researchers found that those in the non-stimulated stunted group had marked deficits in reading and mathematics and were more likely to drop out of school. Evidence, from analytical epidemiological research, indicates that lower educational attainment has implications for future employment and is likely to increase the risk of poverty and poorer health among such individuals. The power of this randomized controlled trial is its illustration that stunting in early childhood is significantly associated with cognitive and educational deficits in late adolescence, which are reduced by stimulation at a young age, thereby providing evidence for the types of effective intervention that can be made in early childhood.
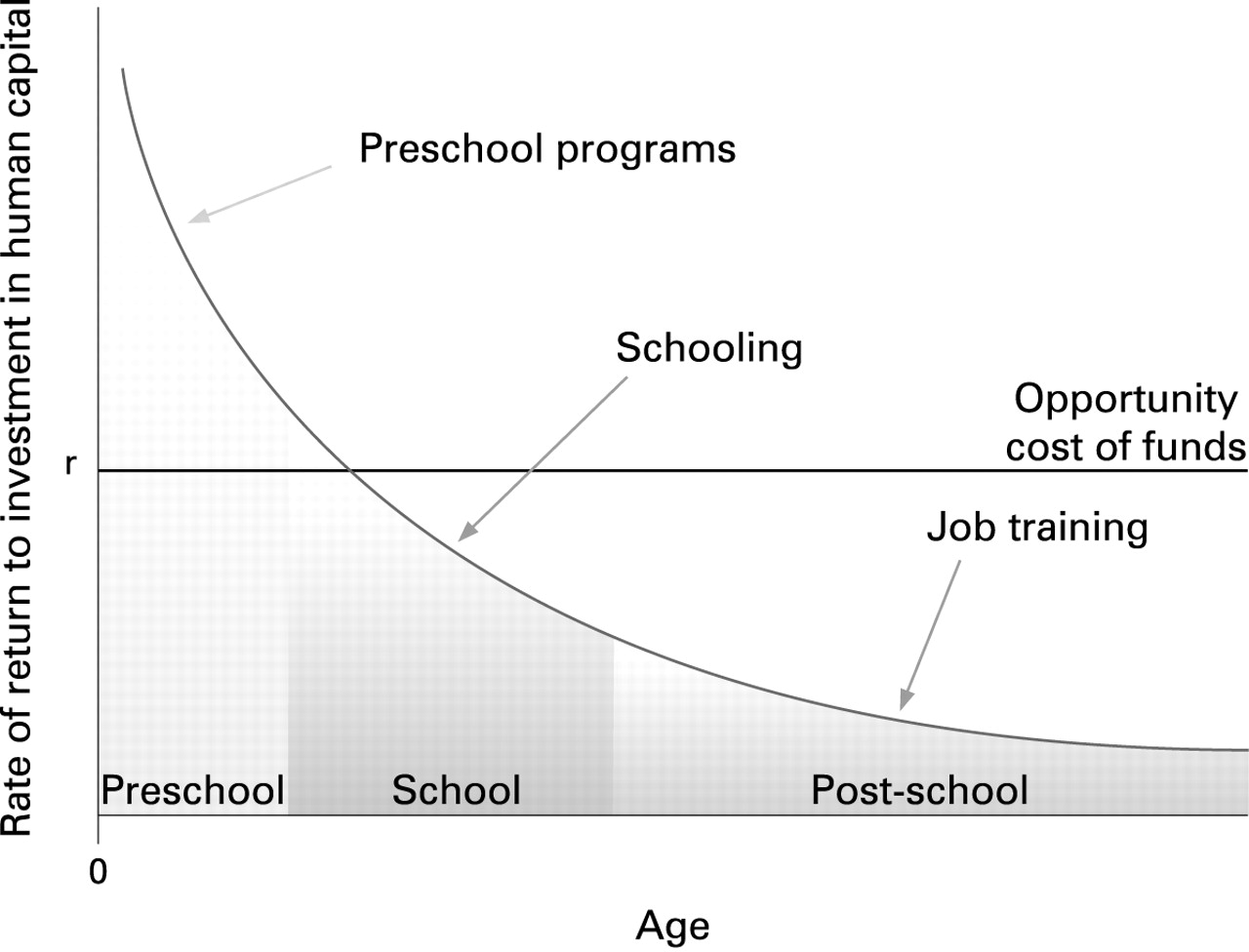
Making the case that intervention in early childhood is good for health equity is one thing. The question that often follows, from policy-makers, is one of efficiency—the cost–benefits of such an approach compared with others. Economic analysis, therefore, is a necessary part of the evidence arsenal for health equity. For example, assessing a large literature on the rate of economic return from investment in skill attainment at different stages in life (fig 2) led Heckman11 to conclude:

Investing in disadvantaged young children is a rare public policy initiative that promotes fairness and social justice and at the same time promotes productivity in the economy and in society at large. Early interventions targeted toward disadvantaged children have much higher returns than later interventions such as reduced pupil teacher ratios, public job training, convict rehabilitation programs, tuition subsidies, or expenditure on police.
We made the point that social policy impacts significantly on health equity. Poverty and lower incomes at the individual level are clearly linked to health. If the relationship between income and health is partially causal and curvilinear, as several studies have suggested, then income redistribution will generate positive public health effects. Does this have any relevance in early life? Absolutely, and we know this through policy analysis—ecological level analysis that looks at the correlation between measures of, for example, disadvantage and the generosity of different types of social policy. Lundberg and colleagues undertook both historical and comparative analysis of the effects of specific social policies on poverty rates, health and survival.12 The correlation of family policy generosity and relative poverty among children in 15 welfare democracies (figure 3) shows a clear negative association (family policy generosity refers to the average amount and not to the population coverage of the systems), with countries such as Finland, Norway and Sweden, countries with generous family policies, having lower child poverty rates. If we look at details, we find that this association is mainly due to policies that support dual-earner families. The contribution of this type of family policy may either be direct through the amount of benefits paid or indirect by supporting two earners and thereby raising the market income of the household. In any way, family policy transfers seem to have redistributive effects and are therefore good for health.

{kind=link}
{kind=link}
{kind=link}
What this study adds
This study expands the discourse about the types of evidence with which to inform policy and practice that will address global health inequity through action on the social determinants of health.
Policy implications
If policy is to address health equity through action on the social determinants of health, policy-makers must broaden the scope of what constitutes evidence and make judgements on evidence compiled on a fitness-for-purpose basis.
What this example shows is that there is no simple translation of evidence of health effect to judgement and recommendation. In almost none of the areas of social determinants of health that the Commission considered was that the case. We were required to broaden the scope of what constituted evidence to include both a variety of types of evidence, including case studies, and chains of plausible reasoning. Failure to broaden in this way would have been a recipe for doing nothing. In conclusion, tackling global health equity through action on the social determinants of health is a matter of social justice, requiring judgement informed by evidence compiled on a fitness-for-purpose basis.
Footnotes
Funding: None declared.
Competing interests: None.