History of modern nutrition science—implications for current research, dietary guidelines, and food policy
BMJ 2018; 361 doi: https://doi.org/10.1136/bmj.k2392 (Published 13 June 2018) Cite this as: BMJ 2018;361:k2392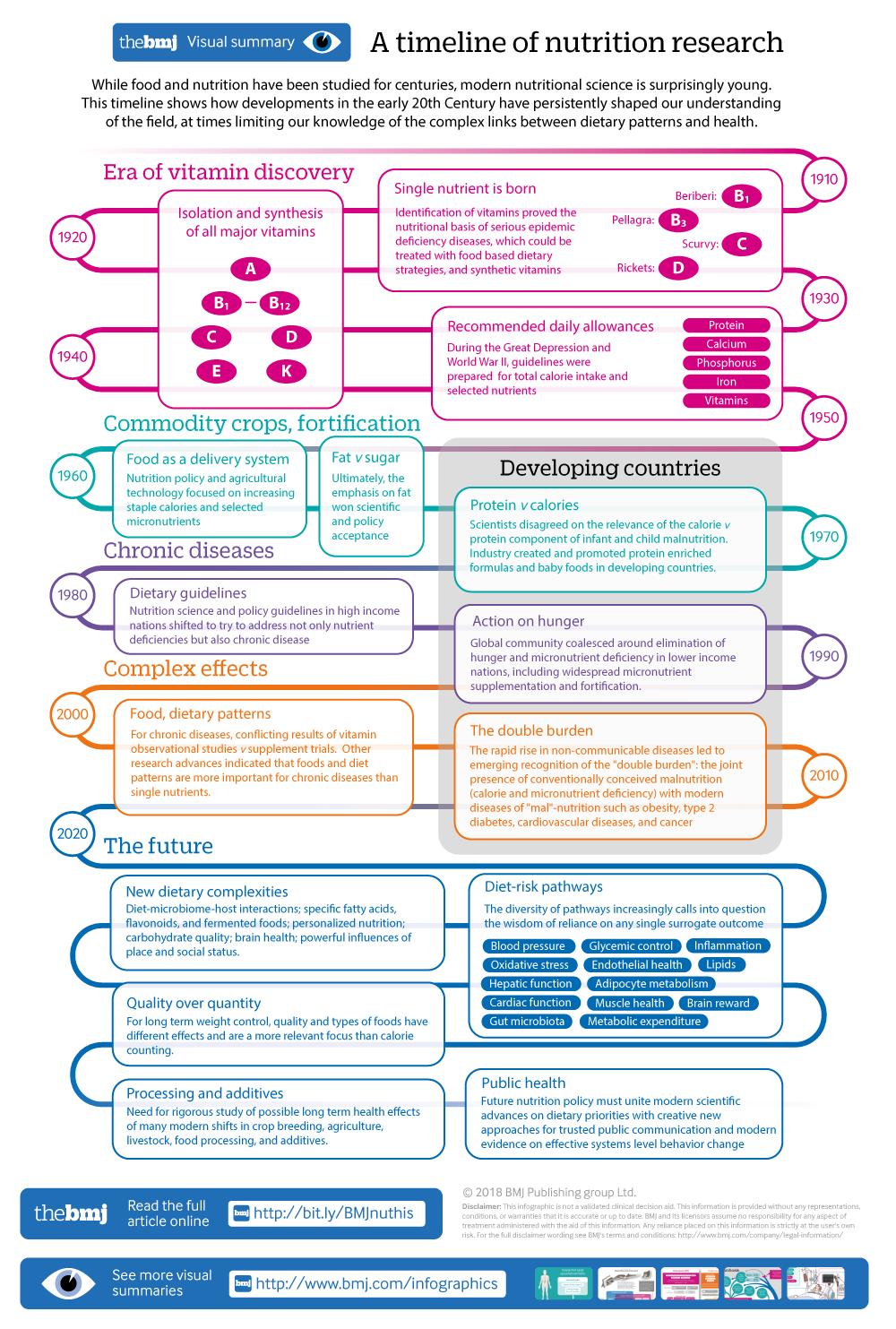
Visual summary available
A timeline of nutrition research, from the era of vitamin discovery in the early 20th Century, through current research on complex effects of dietary patterns, and onwards to the future possibilities for nutrition research and public health implementation

Food for thought
Click here to read other articles in this collection

Although food and nutrition have been studied for centuries, modern nutritional science is surprisingly young. The first vitamin was isolated and chemically defined in 1926, less than 100 years ago, ushering in a half century of discovery focused on single nutrient deficiency diseases. Research on the role of nutrition in complex non-communicable chronic diseases, such as cardiovascular disease, diabetes, obesity, and cancers, is even more recent, accelerating over the past two or three decades and especially after 2000.
Historical summaries of nutrition science have been published, focusing on dietary guidelines, general scientific advances, or particular nutritional therapies.1234 Carl Sagan said, “You have to know the past to understand the present;” and Martin Luther King, Jr, “We are not makers of history. We are made by history.” This article describes key historical events in modern nutrition science that form the basis of our current understanding of diet and health and clarify contemporary priorities, new trends, and controversies in nutrition science and policy.
1910s to 1950s: era of vitamin discovery
The first half of the 20th century witnessed the identification and synthesis of many of the known essential vitamins and minerals and their use to prevent and treat nutritional deficiency related diseases including scurvy, beriberi, pellagra, rickets, xerophthalmia, and nutritional anaemias. Casimir Funk in 1913 came up with idea of a “vital amine” in food, originating from the observation that the hulk of unprocessed rice protected chickens against a beriberi-like condition.5 This “vital amine” or vitamin was first isolated in 1926 and named thiamine, and subsequently synthesised in 1936 as vitamin B1. In 1932, vitamin C was isolated and definitively documented, for the first time, to protect against scurvy,6 some 200 years after ship’s surgeon James Lind tested lemons for treating scurvy in sailors.7
By the mid-20th century all major vitamins had been isolated and synthesised (fig 1). Their identification in animal and human studies proved the nutritional basis of serious deficiency diseases and initially led to dietary strategies to tackle beriberi (vitamin B1), pellagra (vitamin B3), scurvy (vitamin C), pernicious anaemia (vitamin B12), rickets (vitamin D), and other deficiency conditions. However, the chemical synthesis of vitamins quickly led to food based strategies being supplanted by treatment with individual vitamin supplements. This presaged modern day use and marketing of individual and bundled multivitamins to guard against deficiency, launching an entire vitamin supplement industry.

Key historical events in modern nutrition science, with implications for current science and policy
{kind=link}
This new science of single nutrient deficiency diseases also led to fortification of selected staple foods with micronutrients, such as iodine in salt and niacin (vitamin B3) and iron in wheat flour and bread.8910 These approaches proved to be effective at reducing the prevalence of many common deficiency diseases, including goitre (iodine), xerophthalmia (vitamin A), rickets (vitamin D), and anaemia (iron). Foods around the world have since been fortified with calcium, phosphorus, iron, and specific vitamins (A, B, C, D), depending on the composition of local staple foods.10111213
As one of the great accidents of nutrition history, this new science and focus on single nutrients and their deficiencies coincided with the Great Depression and second world war, a time of widespread fear of food shortages. This led to even further emphasis on preventing deficiency diseases. For example, the first recommended dietary allowances (RDAs) were a direct result of these concerns, when the League of Nations, British Medical Association, and the US government separately commissioned scientists to generate new minimum dietary requirements to be prepared for war.14 In 1941, these first RDAs were announced at the National Nutrition Conference on Defence, providing new guidelines for total calories and selected nutrients including protein, calcium, phosphorus, iron, and specific vitamins.15 These historical events established a precedent for nutrition research and policy recommendations to focus on single nutrients linked to specific disease states.
1950s to 1970s: fat versus sugar and the protein gap
During the next 20 to 30 years, calorie malnutrition and specific vitamin deficiencies fell sharply in high income countries because of economic development and large increases in low cost processing of staple foods fortified with minerals and vitamins. At the same time, the rising burdens of diet related non-communicable diseases began to be recognised, leading to new research directions. Attention included two areas: dietary fat and sugar.16171819
Early ecological studies and small, short term interventions, most prominently by Ancel Keys, Frederick Stare, and Mark Hegsted, contributed to the widespread belief that fat was a major contributor to heart disease. At the same time, work by John Yudkin and others implicated excess sugar in coronary disease, hypertriglyceridemia, cancer, and dental caries. Ultimately, the emphasis on fat won scientific and policy acceptance, embodied in the 1977 US Senate committee report Dietary Goals for the United States, which recommended low fat, low cholesterol diets for all. This was not without controversy: in 1980, the US National Academy of Sciences Food and Nutrition Board reviewed the data and concluded that insufficient evidence existed to limit total fat, saturated fat, and dietary cholesterol across the population.20
Some interpret these controversies as evidence of industry influence, and others as natural disagreement and evolution of early science.16171819 More relevant is that both the dietary fat and sugar theories relied on a nutritional model developed to address deficiency diseases: identify and isolate the single relevant nutrient, assess its isolated physiological effect, and quantify its optimal intake level to prevent disease. Unfortunately, as subsequent research would establish, such reductionist models translated poorly to non-communicable diseases.
In less wealthy countries, the main objectives of nutrition policy and recommendations during this period remained on increasing calories and selected micronutrients. In many ways, foods became viewed as a delivery vehicle for essential nutrients and calories. Accordingly, agricultural science and technology emphasised production of low cost, shelf stable, and energy dense starchy staples such as wheat, rice, and corn, with corresponding breeding and processing to maximally extract and purify the starch. As in high income nations, these efforts were accompanied by fortification of staple foods10111213 as well as food assistance programmes to promote survival and growth of infants and young children in vulnerable populations.
Scientists focused on malnutrition disagreed on the relative role of total calories and protein in infant and child diseases such as marasmus and kwashiorkor—also termed “the protein-calorie deficiency diseases.”2122 Support for the “protein gap” concept led to extensive industrial development of protein enriched formulas and complementary foods for developing countries. Other scientists supported the primary role of calorie insufficiency and believed that protein enriched formulas and foods should not replace breast milk. As one prominent scientist wrote in 1966, “Millions of dollars and years of effort… into developing these [high protein] foods would have been better spent on efforts to preserve the practice of breast feeding... being abandoned everywhere.”22
The debate essentially ended when in 1975 leading scientists in the US and London independently concluded from the scientific evidence that a lack of food was the main problem:22 “The concept of a worldwide protein gap… is no longer tenable… the problem is mainly one of quantity rather than quality of food.”23
This conclusion influenced subsequent efforts to tackle malnutrition in developing countries. For example, a formal UK advisory committee on international nutrition aid recommended that, “the primary attack on malnutrition should be through the alleviation of poverty… aid should be directed to projects that will generate income among the poor, even where such projects do not have any marked effect on the national income of the country concerned.”22
However, the earlier decades of uncertainty had fostered a multinational industry that continued to promote formula and baby foods in low income countries based on their protein content and nutrient fortification. In addition, nutrient supplementation strategies remained effective at preventing or treating endemic deficiency diseases. Thus, despite the shift in scientific thinking to focus on economic development, substantial emphasis remained or even accelerated on providing sufficient calories, most often as starchy staples, plus vitamin fortification and supplementation.
1970s to 1990s: diet related chronic diseases and supplementation
Accelerating economic development and modernisation of agricultural, food processing, and food formulation techniques continued to reduce single nutrient deficiency diseases globally. Coronary mortality also began to fall in high income countries, but many other diet related chronic diseases were increasing, including obesity, type 2 diabetes, and several cancers.
In response, nutrition science and policy guidelines in high income nations shifted to try to deal with chronic disease. Building on the 1977 Senate report, the 1980 Dietary Guidelines for Americans was one of the earliest such national guidelines.24 Many of the available data were derived from less robust types of evidence, such as from crude cross-country (ecological) comparisons and short term experiments using surrogate outcomes, mostly in healthy middle aged men. More importantly, these studies followed the deficiency disease model, largely considering isolated single nutrients. Accordingly, the 1980 dietary guidelines remained heavily nutrient focused: “avoid too much fat, saturated fat, and cholesterol; eat foods with adequate starch and fiber; avoid too much sugar; avoid too much sodium.”24 International guidelines were similarly nutrient focused.25 This led to a proliferation of industrially crafted food products low in fat, saturated fat, and cholesterol and fortified with micronutrients, as well as expansion of other nutrient focused technologies to reduce saturated fat such as partial hydrogenation of vegetable oils.
At the same time the global community prioritised action to eliminate hunger and micronutrient deficiency in lower income nations. Major micronutrient targets during this period were iron, vitamin A, and iodine. Evidence was increasing that vitamin A supplements could prevent child mortality from infection, such as measles, as well as preventing night blindness and xerophthalmia.26 Field trials provided a basis for WHO recommendations for widespread micronutrient supplementation, especially during pregnancy, with iron and vitamin A, and for fortification of salt with iodine to prevent goitre and developmental abnormalities such as congenital hypothyroidism and hearing loss.
Based on these priorities, the UN, national governments, and other international groups adopted portfolios for preventing micronutrient deficiencies through supplementation and fortification and integration of the growing relevant evidence. Scientific investigations further focused on other environmental factors that may interact with micronutrients and dietary protein, such as infection and related poor sanitation, leading to concepts such as subclinical enteritis or malabsorption called first “tropical enteritis,” then “environmental enteropathy,” and currently “environmental enteric dysfunction.”272829
Thus, in both lower and higher income nations, for partly overlapping reasons, a nutrient specific focus continued to shape both scientific inquiry and policy interventions.
1990s to the present: evidence debates, diet patterns, the double burden
Among the most important scientific development of recent decades was the design and completion of multiple, complementary, large nutrition studies, including prospective observational cohorts, randomised clinical trials, and, more recently, genetic consortiums. Cohort studies provided, for the first time, individual level, multivariable adjusted findings on a range of nutrients, foods, and diet patterns and a diversity of health outcomes. Clinical trials allowed further testing of specific questions in targeted, often high risk populations, in particular effects of isolated vitamin supplements and, more recently, specific diet patterns. Genetic consortiums provided important evidence on genetic influences on dietary choices, gene-diet interactions affecting disease risk factors and endpoints, and Mendelian randomisation studies of causal effects of nutritional biomarkers.
These advances were not without controversy, in particular the general discordance of findings between cohort studies and those of supplement trials for specific vitamins on cardiovascular and cancer endpoints.3031 Some experts interpreted the discordance as evidence for irredeemable shortcomings of observational studies (inherent residual confounding). Others believed it showed the limitations of single nutrient approaches to chronic diseases as well as potentially reflecting the different methodological designs, with trials often focused on short term, supraphysiological doses of vitamin supplements in high risk patients, while observational studies often focused on habitual intake of vitamins from food in general populations.
In contrast to single nutrients, physiological intervention trials, large cohort studies, and randomised clinical trials provided more consistent evidence for diet patterns, such as low fat diets (few significant effects) or Mediterranean and similar food based patterns (consistent benefits).3233 This concordance was supported by advances in research methods and better understanding of the complementary strengths of different study designs.343536373839
Together, these advances suggested that single nutrient theories were inadequate to explain many effects of diet on non-communicable diseases. This pushed the field beyond the RDA framework and other nutrient metrics designed to identify thresholds for nutrient deficiency diseases, and towards complex biological effects of foods and diet patterns.4041424344 Such factors were increasingly seen to reflect joint contributions and interactions between carbohydrate quality (eg, glycaemic index, fibre content), fatty acid profiles, protein types, micronutrients, phytochemicals, food structure, preparation and processing methods, and additives.
Prospective cohorts and dietary intervention trials showed that a focus on total fat, a mainstay of dietary guidelines since 1980, produced little measurable health benefit; conversely, nutrient based recommendations for specific foods such as eggs, red meats, and dairy products (eg, based on dietary cholesterol, saturated fat, calcium) belied the observed relations of these foods with health outcomes.3233 For weight loss and glycaemic control, decades of emphasis on low fat diets were questioned by the results of a series of prospective cohort studies, metabolic feeding studies, and randomised trials, which showed that foods rich in healthy fats produced benefit, while foods rich in starch and sugar caused harm.33454647 This progress was extended to recognition of the relevance of diet patterns such as traditional Mediterranean or vegetarian diets that emphasised minimally processed foods such as fruits, vegetables, nuts, beans, whole grains, and plant oils and low amounts of highly processed foods rich in starch, sugar, salt, and additives.3233
These recent scientific shifts help explain many uncertainties and controversies in nutrition today. After decades of focus on simple, reductionist metrics such as dietary fat, saturated fat, nutrient density, and energy density, the emerging true complexities of different foods and diet patterns create genuine challenges for understanding influences on health and wellbeing. For several categories of foods, meaningful numbers of prospective observational or interventional studies have become available only recently.3338 Growing realisation of the importance of overall diet patterns has stimulated not only scientific inquiry but also a deluge of empirical, commercial, and popular dietary patterns of varying origin and scientific backing.48 These range, for example, from flexitarian, vegetarian, and vegan to low carb, paleo, and gluten-free. Many of these patterns have specific aims (eg, general health, weight loss, anti-inflammation) and are based on differing interpretations of current evidence.
In lower income countries, concerns about vitamin supplementation have emerged, such as harms associated with higher dose vitamin A supplements, risk of exacerbating infections such as malaria with iron, and safety concerns about folic acid fortification of flour, which might exacerbate neurological and cognitive deficits among people with low vitamin B12 levels.49505152 In addition, a precipitous rise in non-communicable diseases in these countries has led to new focus on the “double burden”—both conventionally conceived malnutrition (insufficient calories and micronutrients) leading to poor maternal and child health and modern malnutrition (poor diet quality) leading to obesity, type 2 diabetes, cardiovascular diseases, and cancer. These dual global burdens are increasingly found within the same nation, community, household, and even person.535455
Yet, after decades of focus in the international nutrition community on vitamin supplements, food fortification, and starchy staples to provide calories, the necessary shift towards diet quality is slowed by considerable inertia. This is seen, for example, in the reductionist, single nutrient focus of many of the UN sustainable development goals. Even when non-communicable diseases are considered, the predominant focus is on obesity rather than the diverse risk pathways and conditions affected by nutrition—facilitating a misleading concept of “overnutrition” rather than unhealthy dietary composition as the root problem.55
Future of nutrition science
Building on the evidence for multifaceted effects of different foods, processing methods, and diet patterns,3233 new priorities for research are emerging in nutrition science. These include optimal dietary composition to reduce weight gain and obesity; interactions between prebiotics and probiotics, fermented foods, and gut microbiota; effects of specific fatty acids, flavonoids, and other bioactives; personalised nutrition, especially for non-genetic lifestyle, sociocultural, and microbiome factors; and the powerful influences of place and social status on nutritional and disease disparities.335657585960
For lower income nations and populations, rigorous investigation is required to understand the optimal dietary patterns to jointly tackle maternal health, child development, infection risk, and non-communicable diseases.
Our understanding of diet related biological pathways will continue to expand (fig 1),335761 highlighting the limitations of using single surrogate outcomes to determine the full health effects of any dietary factor. In addition, future conclusions about diets and health should be based on complementary evidence from controlled interventions of multiple surrogate endpoints, mechanistic studies, prospective observational studies, and, when available, clinical trials of disease outcomes.3536373839 This will require moving away from the current simplistic belief that reliable nutritional evidence can be derived only from large scale randomised trials.
Given the large and continuing global rise in agribusiness and manufactured foods, nutrition science must keep pace with and systematically assess the long term health effects of new food technologies. Relatively little rigorous evaluation has been done on potential long term health consequences of modern shifts in agricultural practices, livestock feeding, crop breeding, and food processing methods such as grain milling and processing; plant oil extraction, deodorisation, and interesterification; dairy fat homogenisation; and use of emulsifiers and thickeners.
Additional complexity may arise in nutritional recommendations for general wellbeing versus treatment of specific conditions. For example, dietary recommendations for treating obesity are now particularly controversial. Many scientists continue to support a basic “energy imbalance” concept of obesity, wherein calories from different foods are all considered equal.62 Conversely, growing evidence suggests that, over longer periods, diet composition may be a more relevant focus than calories because of the varied influences of different foods on overlapping pathways for weight control such as satiety, brain reward, glycaemic responses, the microbiome, and liver function.56636465 Over months to years, some foods may impair pathways of weight homeostasis, others may have relatively neutral effects, and others may promote integrity of weight regulation. These long term effects will be especially relevant as anti-obesity efforts shift from secondary prevention (weight loss in people with obesity) towards primary prevention (avoidance of long term weight gain in populations).
Recognition of complexity is a key lesson of the past. This is common in scientific progress whether in nutrition, clinical medicine, physics, political science, or economics: initial observations lead to reasonable, simplified theories that achieve certain practical benefits, which are then inevitably advanced by new knowledge and recognition of ever-increasing complexity.35
Nutrition policy
Like nutrition science, policy needs to move from simplistic reductionist strategies to multifaceted approaches. Nutrition policy to reduce non-communicable diseases has so far generally relied on consumer knowledge—simply inform the public through education, dietary guidelines, product nutrition labels, etc, and people will make better choices. However, it is now clear that knowledge alone has relatively limited effects on behaviour, and that broader systems, policy, and environmental strategies are needed for effective change.6667
Compounding these challenges, many current strategies remain focused on reductionist constructs such as total fat or total saturated fat,4168 overlooking the importance of food type and quality, processing methods, and diet patterns. Another example of policy lag involves energy balance. Policy makers continue to promote total calorie labelling laws for menus and packaging and other calorie reduction policies, rather than aiming to increase calories from healthy foods and reduce calories from unhealthy foods.
The public is understandably bewildered by these evolving dietary messages. Many food companies compound the confusion by marketing products rich in refined flours, sugar, salt, and industrial additives, exploiting added micronutrients or terms such as “organic,” “local,” or “natural” to supply a false aura of healthiness. Public uncertainty is amplified by competing nutritional messages from varied media sources, online and social networks, cultural thought leaders, and commercial outlets, whose messages vary depending on underlying goals, expertise, perspectives, and competing interests.35
Although reductionist policies may have some value to reduce specific additives—eg, trans fats, sodium, added sugar—whole food based policies will be crucial to fully address diet related illnesses. Most policy innovation has focused on sugar sweetened drinks, following the model of the WHO Framework Convention on Tobacco Control: tax, restrict places of sale, restrict marketing, use warning labels. This construct breaks down for incentivising consumption of healthy foods. Integrated policy, investment, and cultural strategies are needed to create change in food production and manufacturing, worksites, schools, healthcare systems, quality standards and labelling, food assistance programmes, research and innovation, and public-private partnerships.
To be effective, future nutrition policy must unite modern scientific advances on dietary priorities (specific foods, processing methods, additives, diet patterns) with trusted communication to the public and modern evidence on effective systems level change. This includes a shift from the global medicalisation of health towards addressing the interconnected personal, community, sociocultural, national, and global determinants of food environments and choices.6667 In both lower and higher income countries, interventions must consider the double burdens of food insecurity and chronic disease, and their links to disparities in education, income, and opportunity. This will require substantially more funding for research, both from government sources and through appropriately fashioned, transparent public-private partnerships.6970 Guided by knowledge of the past, creative new approaches are needed for accelerated scientific investigation, coordination, and translation of current and future advances.
Key messages
Modern nutrition science is young: It is less than one century since the first vitamin was isolated in 1926
The first half of the 20th century focused on the discovery, isolation, and synthesis of essential micronutrients and their role in deficiency diseases
●This created strong precedent for reductionist, nutrient focused approaches for dietary research, guidelines, and policy to address malnutrition
This reductionist approach was extended to address the rise in diet related non-communicable diseases—eg, focusing on total fat, saturated fat, or sugar rather than overall diet quality
Recent advances in nutrition science have shown that foods and diet patterns, rather than nutrient focused metrics, explain many effects of diet on non-communicable disease
●Lower income countries are recognising a growing “double burden” (combined undernutrition and non-communicable disease)
Nutrition policy should prioritise food based dietary targets, public communication of trusted science, and integrated policy, investment, and cultural strategies to create systems level change across multiple organisations and environments
Footnotes
Contributors and sources: All three authors have widely studied, reported on, and served in policy advisory roles on nutrition and health issues. DM had the idea for the article and drafted it with IR. All authors contributed to revising the draft and approved the final version. The authors selected the literature for inclusion in this manuscript based on their own expertise and knowledge, discussions with colleagues, and editorial and reviewer comments.
Competing interests: We have read and understood BMJ policy on declaration of interests and declare the following interests: DM reports personal fees from Acasti Pharma, GOED, DSM, Nutrition Impact, Pollock Communications, Bunge, Indigo Agriculture, and Amarin; scientific advisory board, Omada Health, Elysium Health, and DayTwo; and chapter royalties from UpToDate; all outside the submitted work. This research was partly supported by the NIH, NHLBI (R01 HL130735). The funders had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Provenance and peer review: Commissioned; externally peer reviewed.
This article is one of a series commissioned by The BMJ. Open access fees for the series were funded by Swiss Re, which had no input into the commissioning or peer review of the articles.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.