Article Text

Abstract
Background Type 2 diabetes (T2D) is preventable, it is increasing in prevalence and it is a major risk factor for morbidity and mortality. Importantly, residents of neighbourhoods with high levels of disorder are more likely to develop T2D than those living in less disordered neighbourhoods and neighbourhood disorder may exacerbate genetic risk for T2D.
Method We use genetic, self-reported neighbourhood, and health data from the Health and Retirement Study. We conducted weighted logistic regression analyses in which neighbourhood disorder, polygenic scores for T2D and their interaction predicted T2D.
Results Greater perceptions of neighbourhood disorder (OR=1.11, p<0.001) and higher polygenic scores for T2D (OR=1.42, p<0.001) were each significantly and independently associated with an increased risk of T2D. Furthermore, living in a neighbourhood perceived as having high levels of disorder exacerbated genetic risk for T2D (OR=1.10, p=0.001). This significant gene×environment interaction was observed after adjusting for years of schooling, age, gender, levels of physical activity and obesity.
Conclusion Findings in the present study suggested that minimising people’s exposure to vandalism, vacant buildings, trash and circumstances viewed by residents as unsafe may reduce the burden of this prevalent chronic health condition, particularly for subgroups of the population who carry genetic liability for T2D.
- genetics
- neighborhood/place
- diabetes
Statistics from Altmetric.com
Type 2 diabetes (T2D) is a leading risk factor for cardiovascular and cancer-related morbidity and mortality, is increasing in prevalence worldwide and is preventable.1 Many factors contribute to the development of T2D, including individual characteristics (eg, physical activity, genetic risk2) and broad social factors (eg, lack of outlets for physical activity3). Many individual behaviours are either supported or constrained by features of people’s neighbourhoods, such as resources that support physical activity.4 Some have therefore theorised that neighbourhood features relate to residents’ health through people’s health behaviours.5
Very little work has evaluated the extent to which neighbourhood disorder relates to T2D through interactions with genetic risk. A number of genetic loci increase the risk of T2D, and the heritability of T2D ranges from 20% to 80%.6 A growing literature indicates that T2D is the result of interactions between genotype and environment (GxE), where genetic risk for T2D is heightened by factors such as sedentary lifestyles and obesity.7 We believe that these lifestyles are downstream of more fundamental social factors such as the places in which people live.8 In the present study, we examined whether increased perceptions of neighbourhood disorder exacerbate genetic risk for T2D.
Neighbourhoods and diabetes
People living in neighbourhoods perceived to be disordered (eg, unsafe, vandalised) report more chronic health conditions including diabetes.9 This relationship is posited to be established through a sense of fear,10 which results in a state of physiological vigilance11 and unwillingness to engage in outdoor physical activity. Moreover, neighbourhood disorder was found to completely explain the well-established association between neighbourhood economic disadvantage and poorer health.9 These findings suggest that efforts to improve neighbourhood conditions may also reduce community-level burden of disease.
Findings from the Moving to Opportunities Study, one of the few examples of a randomised controlled study of neighbourhoods and health, suggest that people who move out of high-poverty areas have reduced prevalence of diabetes and extreme obesity.12 Findings such as these support the causal hypothesis of neighbourhoods, or that neighbourhood poverty is uniquely associated with an increased risk for cardiometabolic diseases. Coupled with research indicating that neighbourhood disorder mediates the neighbourhood poverty-T2D association, there is strong reason to believe that efforts to mitigate neighbourhood disorder may help to slow the rapidly growing population of individuals affected by T2D and other chronic health conditions.
Diabetes and GxE
A diagnosis of T2D is thought to be a consequence of both genetic and environmental influences6 and some argue that genetic influences only manifest in certain environments.7 Evidence in support of this argument aligns with the social trigger GxE hypothesis which posits that adverse environmental features strengthen the genotype-outcome association.13 For instance, although specific genetic variants explain only a small proportion of variance in the likelihood of developing T2D,6 those carrying these variants who also engage in sedentary behaviours are at an increased risk of disease.7 This literature has established the importance of considering both genetic and environmental processes in the development of T2D, and the importance of moving beyond the candidate gene approach. Complex traits, including those with relevance in public health, are polygenic, or influenced by multiple genetic regions.14 As such, GxE investigations would benefit from the inclusion of summary genetic scores that account for a greater portion of variance in the health outcome than can be observed with single genetic variants.15
Recent research has investigated GxE occurring within the larger environments in which people live. For instance, youth are at increased risk of obesity, an outcome strongly associated with T2D,16 when they carry genetic variants for higher body mass index (BMI) and attend schools with fewer resources to maintain a healthy weight.17 It follows, then, that resources (or lack thereof) within neighbourhoods may further interact with genetic risk for T2D. Despite current evidence for GxE in relation to cardiometabolic outcomes,17 however, existing reviews18 demonstrate a paucity of research on potential interactions with neighbourhood disorder (although see Coulon et al 19 for a GxE in relation to waking cortisol). Older adults may be particularly vulnerable to neighbourhood disorder, through age-related declines in cognitive and physical health and functioning,20 and because many chronic cardiometabolic diseases become apparent in older adulthood. Given that incident T2D is increasing rapidly worldwide,1 it is critical to investigate whether modifiable features of neighbourhoods contribute to this public health issue.
The present study
The goal of the present study is to examine whether perceptions of neighbourhood disorder trigger or exacerbate genetic risk for T2D. This study adds to the growing body of research investigating GxE in the context of people’s larger environments, which has already demonstrated interactions with school-level factors.17 We will use a polygenic score (PGS) for T2D that summarises genome-wide genetic risk, rather than focusing on any single genetic region. By conducting this research with a nationally representative sample of older adults, findings from this research may inform intervention efforts aimed at containing the population of individuals affected by T2D.
Method
Participants and procedures
We used data from the Health and Retirement Study (HRS) national survey, the purpose of which was to examine health and retirement among US men and women over 50 years of age. Starting in 1992, participants’ economic, physical, mental and cognitive well-being have been assessed every 2 years. The sample is refreshed every 6 years by adding people aged 51–56 years to maintain representativeness of the population aged over 50 years. As part of the core HRS interviews, respondents reported any chronic health conditions they had. In 2006, HRS researchers conducted face-to-face interviews with a random half of households. During these interviews, Buccal swabs were used to collect DNA samples. In 2008, DNA was extracted from saliva samples from participants in the other half of HRS households. These samples have been combined and genotyped. HRS researchers also collected anthropometric data from participants, including height and weight. During these interviews, participants completed psychosocial questionnaires including items assessing neighbourhood disorder. The questionnaire was administered again in 2010 (a follow-up from 2006) and 2012 (a follow-up from 2008), and the present study included the most recent responses to the items assessing T2D and neighbourhood disorder. All participants signed separate consent forms prior to providing biological samples.
The PGSs used in the present analyses were constructed using data from non-Hispanic whites and may therefore not have the same predictive ability among those from other racial/ethnic groups.21 22 As such, the analytic sample in the present study was restricted to those who self-reported non-Hispanic white race/ethnicity and who had T2D PGSs (n=12 090). Of those 12 090 participants, 1527 did not complete additional waves of the HRS after genetic data were collected in 2006/2008, 1643 did not return the psychosocial questionnaire with items assessing neighbourhood disorder, and 288 did not complete the core interview including questions about T2D. A smaller group of individuals did not respond to questions assessing T2D (n=3), neighbourhood disorder (n=5) and physical activity (n=26), resulting in an analytic sample of 8588 respondents.
Measures
Diabetes
As part of the core HRS interview, participants answered the question, "Has a doctor ever told you that you have diabetes or high blood sugar?" At the time the question was answered, HRS interviewers had knowledge regarding whether the respondents had reported having diabetes in previous waves of the survey. Respondents were coded as having diabetes (scored 1) if they currently or had previously reported having diabetes, and were coded as not having diabetes (scored 0) if they currently did not or disputed ever having had diabetes.
Neighbourhood disorder
Participants responded to four questions regarding neighbourhood disorder.23 Item responses, which ranged from 1 to 7, indicated the degree to which participants perceived vandalism, trash and vacant buildings in their neighbourhoods as well as the degree to which they believed people would feel safe walking in their neighbourhoods alone. Items assessing vandalism, safety and vacant buildings were reverse-coded and all responses were averaged so that higher scores indicated greater perceived neighbourhood disorder (Cronbach’s α=0.82).
Genetic data
At the Centre for Inherited Disease Research,24 DNA was genotyped using the Illumina HumanOmni2.5–4 V.1 array. Roughly 2.4 million single nucleotide polymorphisms (SNPs) were measured, of which roughly 1.9 million passed quality control procedures (see Weir25 for quality assurance/quality control procedures). At the University of Washington Genetics Coordinating Center, roughly 21 million SNPs were examined for allele status using Imputation to the 1000 Genomes Project.24
In a meta-analysis of 12 genome-wide association studies including 34 840 cases and 114 981 controls of European descent, researchers identified 10 novel genome-wide significant loci for T2D, and provided a supplementary table listing all genome-wide significant SNPs.26 Based on this meta-analysis, HRS researchers constructed a T2D PGS among non-Hispanic whites.27 In the construction of the scores, all genotyped SNPs were used (no imputed SNPs and no clumping or pruning based on linkage disequilibrium). Scores were constructed by summing the weighted beta estimates. Final T2D PGSs were standardised among non-Hispanic whites (mean=0, SD=1). To adjust for potential population stratification, or that people from different racial/ethnic backgrounds may have differing genetic structures,28 the top five principal components27 were included as covariates in statistical models.
Additional covariates
HRS respondents indicated the number of days they had engaged in vigorous (eg, running, cycling, swimming, digging with a shovel), moderate (eg, gardening, cleaning the car, dancing, walking, stretching) or light (eg, vacuuming, laundry) physical activity with the following scale: 1=never, 2=1–3 times per month, 3=one time per week, 4=more than one time per week and 5=every day. In the present study, this information came from the RAND HRS file.29 In the present study, the total number of days reported in each of these levels of physical activity were weighted so that vigorous activity (multiplied by 5; score ranged from 5 to 25) received greater weight than moderate activity, which received greater weight (multiplied by 3; score ranged from 3 to 15) than light activity (multiplied by 1; score ranged from 1 to 5). A summary physical activity variable was constructed that summed across the weighted number of days reported in each of these levels of physical activity (score ranged from 9 to 45).
Height and weight assessed in the face-to-face interviews were used to construct a measure of BMI, calculated as the ratio of a person’s weight in kilograms to height in metres squared. Using this formula, participants were categorised as obese if this ratio were at or greater than 30. Participants reported the total number of years of schooling they had completed. We also included age and gender as covariates.
Statistical analyses
We survey set the data to accommodate the complex survey design in HRS. We used the svy: suite of commands in Stata 13 to conduct logistic regressions examining T2D. Before testing the key hypothesis for GxE in the present study, potential rGE, or correlation between the PGS for T2D and perceptions of neighbourhood disorder were assessed. To this aim, we evaluated two models, one in which perceptions of neighbourhood disorder were regressed on the T2D PGS, and the other in which T2D PGSs were regressed on perceptions of neighbourhood disorder. Both of these models were adjusted for age, gender, years of schooling, physical activity, obesity and principle components.
In our first logistic model predicting T2D, we tested the hypotheses that higher PGSs for T2D and neighbourhood disorder would each be related to increased odds of T2D, adjusting for age, gender, years of schooling, self-reported physical activity, obesity and principle components. Model 2 additionally included an interaction term; we examined whether higher perceptions of neighbourhood disorder would strengthen the hypothesised association between the T2D outcome and PGSs (GxE). In model 3, interactions between all covariates (age, gender, years of schooling, physical activity and obesity) and both predictors (perceptions of neighbourhood disorder and PGSs for T2D) were included as covariates.30
Results
About 19% of the weighted sample reported having been told by a doctor that he or she had T2D either at present or some point in the past. Roughly 41% of the sample was categorised as obese, with a BMI at or greater than 30. On a scale from 1 to 7, participants reported low levels of disorder (mean=2.36, SD=0.02). The weighted sample was fairly physically active and well-educated, with average scores of 24.02 on the summary measure of physical activity (SD=0.11, on a scale from 9 to 45) and 13.88 years of schooling (SD=0.07), on average. Participants were, on average, 66.53 years of age (SD=0.11) and there were more women (53.58%) than men. Regression models evaluating potential rGE, or the possibility that PGSs for T2D and perceptions of neighbourhood disorder are significantly associated with one another, yielded null results (p=0.186, p=0.186, respectively).
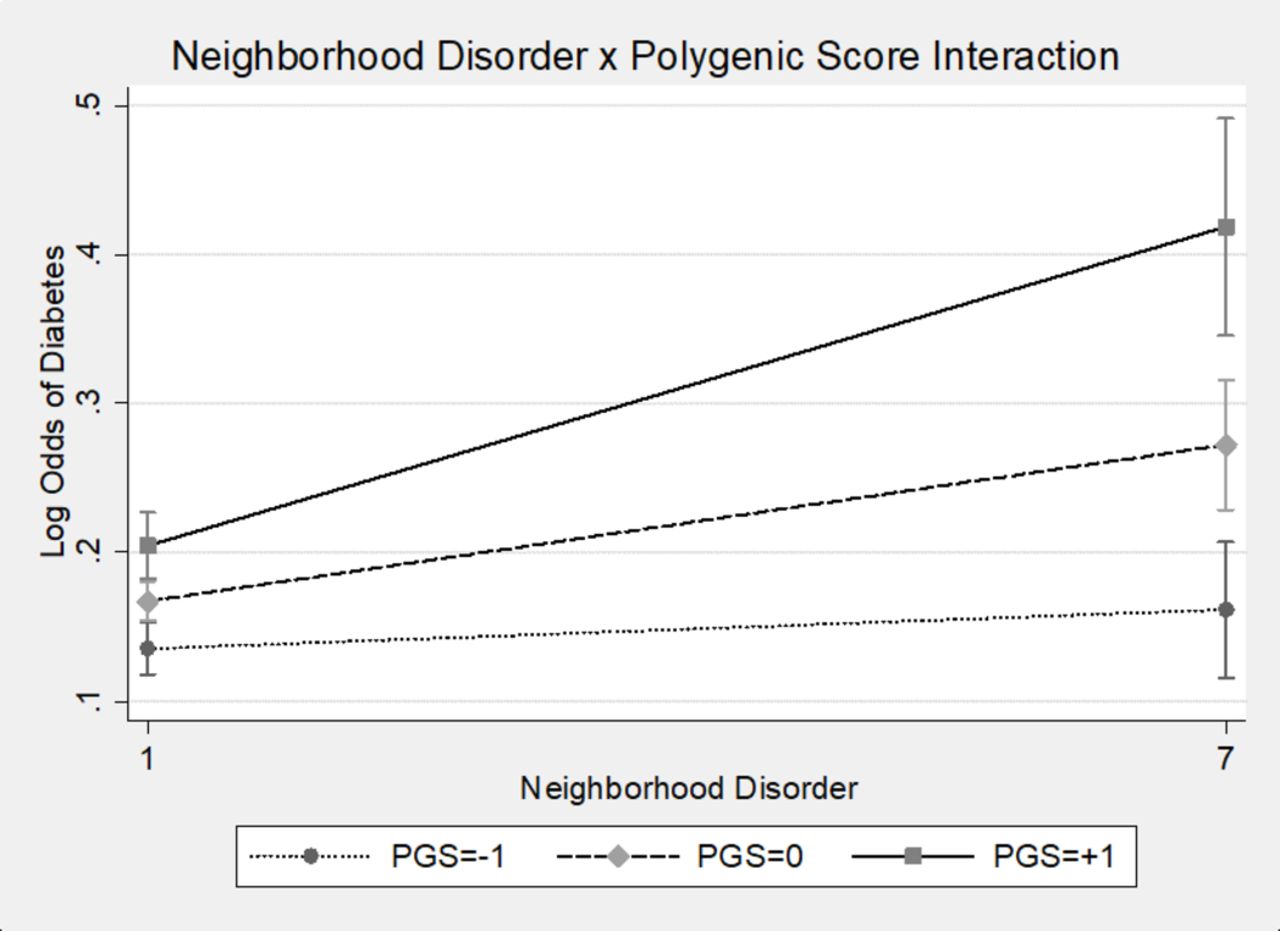
Results of logistic regression models predicting T2D are presented in table 1. Model 1 results indicated that higher T2D PGSs and perceptions of neighbourhoods disorder were significantly associated with greater odds of having T2D. Men, older adults, those categorised as obese and those who engaged in less physical activity were more likely to have T2D than women, younger adults, those not categorised as obese and those who were more physically active. We tested our primary hypothesis that higher neighbourhood disorder would trigger genetic risk for T2D in model 2. The interaction between neighbourhood disorder and T2D PGSs was significant (figure 1); higher T2D PGSs were associated with greater risk of T2D, and this was even more so for those living in neighbourhoods perceived as having higher levels of disorder. This interaction remained statistically significant in model 3 when the covariate×T2D PGS and covariate×perceptions of neighbourhood disorder interactions were added.

{kind=link}
Neighbourhood disorder×type 2 diabetes polygenic score (PGS) interaction.
Main and interactive effects of T2D PGS and neighbourhood disorder on T2D: logistic regressions
Discussion
It has already been established that both individual-level and neighbourhood-level factors are related to the development of T2D.2 Furthermore, researchers have posited that both genetic susceptibility and some exogenous ‘diabetogenic’ trigger are prerequisites in the development of type 1 diabetes.31 In support of our hypothesis, results from the present study suggest a similar triggering of the disease process with regard to T2D, and specifically indicates that perceptions of neighbourhood disorder may exacerbate individuals’ genetic predisposition for T2D.
That individual characteristics may moderate the association between neighbourhood features and health is not a new concept. However, extant examples generally find that those with greater social ties32 or higher individual socioeconomic status,33 both representing individual social characteristics, fare better in more adverse neighbourhood environments. The novel finding in the present study is that an additional individual characteristic, people’s underlying genetic vulnerability to T2D, interacts with features of the neighbourhood (ie, perceptions of disorder).
Although evidence indicating the health relevance of neighbourhood features for residents’ health has been growing substantially in recent decades,5 efforts to make health salutary neighbourhood change have been slower to progress.34 Reasons for the apparent disconnect between the evidence base and policy change include lack of clarity regarding the specific neighbourhood features that associate with residents’ health34 as well as relatively small neighbourhood effects sizes.35 Results from the present study may inform solutions to these obstacles. First, we focused on a specific feature of residents’ neighbourhoods, that is, perceptions of disorder. Second, we showed that the strength of the association between neighbourhood disorder and T2D depended on residents’ genotypes for SNPs related to T2D. This is important because it suggests that neighbourhood effects may have been underestimated in previous investigations reporting only average neighbourhood effects. Taken together, our findings suggest that minimising residents’ exposure to neighbourhood disorder may reduce incident T2D at community levels.
A clear limitation of the present study was the restricted sample. Given that the PGSs used in the present study were derived from individuals of European descent, the present analyses included only those self-reporting as non-Hispanic white. This restriction minimises generalisability of the findings. Generalisability may be of particular concern in the present study for two reasons. First, non-Hispanic white individuals generally reside in less disordered neighbourhoods compared with racial and ethnic minorities in the United States.36 Indeed, the non-Hispanic white participants in the present study generally reported low levels of neighbourhood disorder. Second, a related but distinct phenomenon is that which indicates people perceive more disorder in neighbourhoods with a greater number of racial/ethnic, particularly Latino or black, residents.36 It is therefore critical that future tests of these questions include racial/ethnic minorities, both in the construction of PGSs, and in the investigation of GxE.
In the present study, neighbourhood disorder was reported by the respondents. One concern regarding self-reported neighbourhood indicators involves common source bias, or that individuals who view their experiences through a negative lens may overestimate levels of disorder in their neighbourhoods. However, researchers have directly compared objectively-assessed and self-reported levels of neighbourhood disorder and have found that these assessments are highly correlated.37 Moreover, given the intimate nature of the data, some have argued that the ideal informant regarding daily levels of disorder and other social processes within a neighbourhood are the residents themselves.38 Nevertheless, future research may benefit from the inclusion of measures of neighbourhood disorder from outside raters. As stated elsewhere,39 this suggestion is in line with recommendations regarding the inclusion of multidimensional and multilevel characteristics of the built and social environment in order to properly understand the full contours of environmental moderation of genetic influences on health. Lastly, although we included years of schooling as a covariate in our models (which neither interacted with T2D PGSs nor perceptions of neighbourhood disorder), future research may be strengthened with the inclusion of objective measures of neighbourhood socioeconomic standing.
Notwithstanding these limitations, the present analyses represent the first investigation of potential neighbourhood GxE in relation to T2D, and suggest that one way by which neighbourhoods establish their associations with T2D may be through a triggering of genetic risk. Findings support the notion that neighbourhood improvement efforts, perhaps by reinvesting in community-building surveillance, building repairs and other maintenance programmes may assist in curbing an important current public health concern.
What is already known on this subject
People who live in disordered neighbourhoods, that is, those with more trash and vandalism, generally have poor health.
Exposure to neighbourhood disorder is associated with an increased risk for type 2 diabetes, for example, which is a highly heritable health outcome.
A large literature suggests individual differences in susceptibility, however, with neighbourhood disorder related to worse health consequences for some than others.
What this study adds
Results from the present study suggest that exposure to neighbourhood disorder ‘triggers’ genetic risk for type 2 diabetes.
Although living in a neighbourhood perceived to have high levels of disorder increases peoples’ risk for type 2 diabetes, this is even more so for those genetically predisposed to the disease.
This finding may help to explain individual differences in susceptibility to neighbourhood disorder, and supports efforts for neighbourhood improvement.
References
Footnotes
Contributors JWR contributed to the conception of the study, data analysis and interpretation and drafting of the manuscript. JDB contributed to the data analysis interpretation and drafting of the manuscript. EC contributed to the collection of data and drafting of the manuscript. All authors read and approved the final manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This research was based on work supported by a National Institutes of Health/National Institute on Aging training grant (T32-AG000037-37) and a National Institutes of Health/National Institute on Aging career development grant (1K99AG055699-01) to JWR, and a National Institutes of Health/National Institute on Aging grant (R25 AG053227). These sources of funding supported the data analysis and writing of this report. The data collection for the Health and Retirement Study is also supported by the National Institute on Aging (U01 AG009740).
Competing interests None declared.
Ethics approval This study was approved by the Institutional Review Board of the University of Michigan.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement HRS data sets are publicly available. No additional unpublished data were used.
Patient consent for publication Not required.