Article Text

Abstract
Introduction Stunting or linear growth faltering, measured by length-for-age Z-score (LAZ), remains a significant public health challenge, particularly in rural low-income and middle-income countries. It is a marker of inadequate environments in which infants are born and raised. However, the contributions of household resource insecurities, such as food and water, to growth and growth trajectory are understudied.
Methods We used the cluster-randomised Sanitation Hygiene and Infant Nutrition Efficacy trial to determine the association of household-level food insecurity (FI) and water insecurity (WI) on LAZ and LAZ trajectory among infants during early life. Dimensions of FI (poor access, household shocks, low availability and quality) and WI (poor access, poor quality, low reliability) were assessed with the multidimensional household food insecurity and the multidimensional household water insecurity measures. Infant length was converted to LAZ based on the 2006 WHO Child Growth Standards. We report the FI and WI fixed effects from multivariable growth curve models with repeated measures of LAZ at 1, 3, 6, 12 and 18 months (M1–M18).
Results A total of 714 and 710 infants were included in our analyses of LAZ from M1 to M18 and M6 to M18, respectively. Mean LAZ values at each time indicated worsening linear growth. From M1 to M18, low food availability and quality was associated with lower LAZ (β=−0.09; 95% −0.19 to –0.13). From M6 to M18, poor food access was associated with lower LAZ (β=−0.11; 95% −0.20 to –0.03). None of the WI dimensions were associated with LAZ, nor with LAZ trajectory over time.
Conclusion FI, but not WI, was associated with poor linear growth among rural Zimbabwean infants. Specifically, low food availability and quality and poor food access was associated with lower LAZ. There is no evidence of an effect of FI or WI on LAZ trajectory.
- Malnutrition
Data availability statement
Data are available on reasonable request. Deidentified participant data are available from the SHINE Trial team and Zvitambo Institute for Maternal and Child Health Research on reasonable request. Please email webadmin@zvitambo.com for requests.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Food insecurity, in the form of inadequate food access, is an underlying risk factor for stunting and poor child growth.
Contaminated drinking water is also a known risk factor for poor child growth and health.
WHAT THIS STUDY ADDS
Different aspects of food insecurity (availability, quality, access) are associated with lower length-for-age Z-score (LAZ).
Poor water access, poor water quality and low water reliability are not associated with LAZ.
Neither food insecurity nor water insecurity is associated with infant growth trajectory.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
For improved child growth, renewed attention should be paid to improving food availability and quality, in addition to ensuring adequate food access.
Further research is needed to investigate the link between water insecurity conceptualised broadly and child growth.
Introduction
Stunting represents the most prevalent form of child malnutrition globally, with a 2020 estimate of 144 million children under 5 years of age affected.1 Stunted growth occurs when infant length or height falls below negative 2 SDs(<−2 SDs), in comparison with the WHO Child Growth Standards for the same age and sex group.2 Several more millions of children suffer from less severe forms of growth faltering,3 and any amount of poor linear growth adversely affects child health and well-being.3 4
Linear growth faltering often begins at conception and continues for about 2 years after the child’s birth,5 beyond which time, it is considered largely irreversible.6 Children with poor linear growth are more likely to experience higher rates of morbidity,7 8 7,8 mortality,9 suboptimal cognitive, motor and social development,10–12 and later incidence of chronic diseases such as obesity and other cardiometabolic diseases during adulthood.13 14 Growth faltering also has intergenerational effects, whereby women who were stunted during childhood are at greater risk of bearing stunted children.5 As a marker for these distal negative outcomes on child health and well-being, stunting represents a valuable measure of public health importance.15
The UNICEF Conceptual Framework for Undernutrition16 and its adapted versions8 17–19 identify a host of risk factors for linear growth faltering at multiple levels. One key underlying determinant is household-level food insecurity (FI), defined as the opposite of when ‘all people at all times have physical, social and economic access to sufficient, safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life’.20 Epidemiological evidence on the association between household FI and linear growth of children under 5 is inconclusive, varying from positive,21–28 to no association,29–32 and even to mixed associations.33 34 These existing studies have focused primarily on poor food access, experiences associated with inadequate food access, or diversity of household diet, as measures of FI. Other aspects of FI such as availability, utilisation and stability of the food supply have not been investigated. Moreover, with the exception of one longitudinal study in rural Bangladesh with infants followed from birth to 24 months,21 all studies have assessed the relationship between FI and infant length at a single time point. Therefore, growth and growth trajectory during early life remain unclear in relation to household FI.
The second major household driver of undernutrition suggested by the UNICEF framework relates to water insecurity (WI), specifically unsafe water. Contaminated water is assumed to compromise infant growth by increasing the risk of diarrhoeal diseases via poor sanitation and hygiene.35–37 The current literature on the association between water and linear growth is inconsistent, perhaps due to the narrow definition of water insecurity as untreated water38–40 or non-piped sources41–44 But household-level WI, such as FI, includes dimensions beyond unsafe water such as availability or sufficiency, access, affordability and reliability of the water supply in order to support well-being and the capacity to undertake economic, social and cultural activities.45–47 For example, WI assessment should consider water for consumption (eg, drinking, cooking), non-drinking hygiene (eg, bathing, cleaning) and subsistence (eg, agriculture, animal care). These WI dimensions may impact growth and growth trajectory by influencing maternal and infant hydration and health, food availability and preparation, and infant feeding behaviours.48–51 Recent nationally representative cross-sectional data employing a broader conceptualisation inclusive of household and regional WI identified an indirect effect of dietary diversity on stunting, but causal evidence is lacking.52 Thus, the limited consideration given to WI constitutes an important gap in the current literature on stunting.
The burden of growth faltering is highly prevalent in South Asia and sub-Saharan Africa (SSA),1 53 where the majority of the world’s 750 million severely food insecure1 and two billion water insecure people live.54 The focus of our study is the rural population of Zimbabwe, a land-locked country in SSA. Due to the political situation, complicated financial and trade situations, and erratic climate, Zimbabweans are highly affected by both FI and WI.55 Furthermore, about one-third of infants in rural Zimbabwe are stunted,56 and many more experience some level of linear growth faltering.57 58 Yet, the contributions of critical household resources, like food and water, on infant growth have not been properly examined. In countries such as Zimbabwe, addressing FI and WI, depending on the type of intervention, may also have long-term impacts that go beyond the improvement of child growth for example, economic development, women empowerment, increase in school attendance and social advancement.
The Sanitation Hygiene and Infant Nutrition Efficacy (SHINE) trial carried out in rural Zimbabwe reported improved length-for-age Z-score (LAZ) (β= +0.16; 95% CI 0.08 to 0.23) and reduced stunting (RR=0.80; 95% CI 0.73 to 0.88) among infants aged 18 months who received a nutrition intervention consisting of infant nutrient supplementation and maternal nutrition counselling,59 compared with those who did not. These improvements, although significant and consistent with other similar studies,39 40 are quite modest. A higher rate of stunting decline is required if Zimbabwe is to meet the World Health Assembly nutrition target of 40% reduction by 2025.60 Given the gaps identified above, we proposed that resource insecurities of households in which children are born and raised prevent higher effectiveness of current nutrition interventions. This is because resource insecurities prevent adequate child caring and feeding practices.61 Therefore, the purpose of our study was to determine the associations between different aspects of household-level FI and WI on infant growth during the first 1000 days of life. We hypothesised that higher levels of FI and WI will be associated with greater growth faltering and deteriorating trajectories of growth among infants under 2 years of age.
Methodology
Study design
The SHINE trial design and primary outcomes have been published previously.59 62 Additional information on the protocol and statistical analysis plan are available elsewhere (https://osf.io/w93hy). In summary, SHINE randomly assigned clusters, in two rural Zimbabwean districts (Shurugwi and Chirumanzu), to receive one of four interventions: (1) standard of care (SOC), (2) infant and young child feeding (IYCF), (3) water, sanitation, hygiene (WASH) and (4) IYCF+WASH. The clusters were defined as the catchment area of 1–4 village health workers employed by the Ministry of Health and Child Care. Between 22 November 2012 and 27 March 2015, pregnant women aged 15–49 years old who were permanent residents of those rural areas were enrolled. The infants born to the pregnant women were followed over time to ascertain stunting and anaemia at M18. The analyses presented in this paper focus on the SOC arm (n=1166 live born infants), which received only the WHO recommended education modules on optimal breastfeeding practices for all infants from birth to M6. Thus, the SOC arm was considered appropriate for investigating the effects of FI and WI on infant growth and growth trajectory, independent of the SHINE interventions.
Data collection
Research nurses made home visits at multiple times to collect relevant information from households, mothers and infants: at baseline (during pregnancy) and at infant ages 1, 3, 6, 12 and 18 months (M1–M18).
Growth: We used LAZ as the indicator for growth. Recumbent length was measured to the nearest 0.1 cm using a Seca 417 infantometer by trained nurses. The length measurements at each time were converted to LAZ based on the 2006 WHO Child Growth Standards.63
FI and WI: The multidimensional household food insecurity (MHFI) and the multidimensional household waterinsecurity (MHWI) measures, developed specifically for the rural Zimbabwean households, were used.64 These measures were created from separate factor analyses using groups of food-related and water-related variables collected at baseline (during pregnancy) from the SHINE trial. From these analyses, FI and WI were characterised by three dimensions each. MHFI includes (1) poor food access, (2) household shocks and (3) low food availability and quality; whereas MHWI includes (1) poor water access, (2) poor water quality and (3) low water reliability. A description of the variables making up each dimension is provided in table 1. Each MHFI and MHWI dimension was scored in postestimation commands in the ‘PCAmix’ package from the R software (R Foundation for Statistical Computing, Vienna, Austria) V.4.0.2. We used each of these three dimensions of FI and WI as the main continuous exposure variables in this study. These variables were included simultaneously in the statistical models. An important note is that higher scores on the dimensions of FI and WI as described in table 1 represent higher levels of insecurity.
Description of MHFI and water insecurity
Covariates: At baseline (during pregnancy), a structured questionnaire was used to collect information on maternal and household characteristics such as maternal age (years), maternal height (cm), maternal education (some primary, some secondary, completed secondary), formal employment outside the home (yes/ no), marital status (married vs other), religion (apostolic, other Christian, other), parity (parous, nulliparous, missing), household size (number of household members), presence of improved latrine (yes/no), household location (Shurugwi/Chirumanzu) and season at baseline (during pregnancy) interview (calendar quarter). The HIV status of women was determined using a rapid test algorithm; those who tested positive were directed to local clinics for follow-up and treatment. Socioeconomic status (SES) was based on a household wealth index created specifically for this population.65 Maternal depression, based on Edinburgh’s Postnatal Depression Scale,66 and mothering self-efficacy67 were collected using validated scales for the Zimbabwean population as described previously. Pregnant women’s diet adequacy was assessed based on food group consumption, as described in the FANTA project Minimum Dietary Diversity for Women (yes/ no).68 Infant characteristics such as date of birth, sex, birth weight and prematurity (born at<37 weeks of gestation) were abstracted from health facility records. Infant breast feeding in the 24 hours prior to interviews at M6, M12 and M18 was self-reported by the mother.
Since SHINE was household based, the intermediate visits were conducted only when mother–infant dyads still lived at the address where they consented. If after two contact attempts the participants remained inaccessible, they were considered missing at those time points. At M18, participants were visited anywhere in Zimbabwe even if they had moved on from their initial residence. In addition to our sample being restricted to infants from the SOC arm, analyses were further limited to infants who had complete information on FI, WI, at least one LAZ measure out of five and the above prespecified covariates. Infants, who had died prior to the end of the trial (n=67), whose mothers signed voluntary consent to exit the study (n=5) and who had implausible LAZ patterns over time, were also excluded (n=3).
Statistical analyses
Descriptive statistics were used to summarise the characteristics of the infants included in the analysis. Frequencies and percentages were used for categorical variables. Medians (p50) and IQRs were used for the distributions of the FI and WI dimensions. After graphically confirming normal LAZ distribution of our sample, LAZ values were summarised using means and SDs. The associations of FI and WI with LAZ and LAZ trajectory were investigated through multivariable growth curve modelling of their fixed effects. We used unstructured covariance structure to account for multiple measurements of length on the same infant over time. Time interactions with FI and WI represented growth trajectory associated with these exposures in our models.
Two groups of variables were defined a priori. Group 1 included only variables that were considered theoretically critical given the main predictors and population: season at baseline (during pregnancy) interview, household SES, infant sex, residence location, improved latrine and maternal HIV status. Group 2 additionally included risk factors for poor growth: maternal age, height, education, religion, parity, maternal depression, mothering self-efficacy, infant birth weight, prematurity, breast feeding and household size. Group 2 variables and time-covariate interactions were selected using backward stepwise regressions with retention at p<0.2 at each modelling stage. Multicollinearity was tested with variance inflation factors (VIF <5). The best subset of covariates for the growth models was identified by comparing AIC and BIC between models. Two models are presented in the results section. Model 1 consists of group 1 variables and time interaction with infant sex (minimally adjusted model (Min-AM)). Model 2 includes Min-AM, plus maternal age, height, education, religion, infant birth weight, preterm birth, household size, continued breast feeding until M18 and time interactions with maternal height, infant birth weight and continued breast feeding until M18 (fully AM (Full-AM)). All analyses were performed in Stata/MP V.17 (StataCorp).
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of the research presented in this paper.
Results
Population characteristics
Of the 1166 infants born to women enrolled in SHINE’s SOC arm, 714 and 710 infants had complete information for growth analysis from M1 to M18 and from M6 to M18 (figure 1). Table 2 describes the characteristics of those infants, their mothers and households. Follow-up of the mother–infant dyads was lowest at M1 and M3 study visits because Zimbabwean women typically move back to their maternal home in the immediate postnatal period. On average, infants weighed 3.08 (±0.48) kg at birth, although 19.9% were born preterm. More than half of the infants were still breastfed at M18 (54.3%). Mean LAZ values at M1, M3 and M6 were similar and did not indicate stunting for the sample, although lower values were observed at M12 (−1.27±1.09) and M18 (−1.60±1.09). Dimension scores of FI and WI were below zero, suggesting modest overall FI and WI levels.

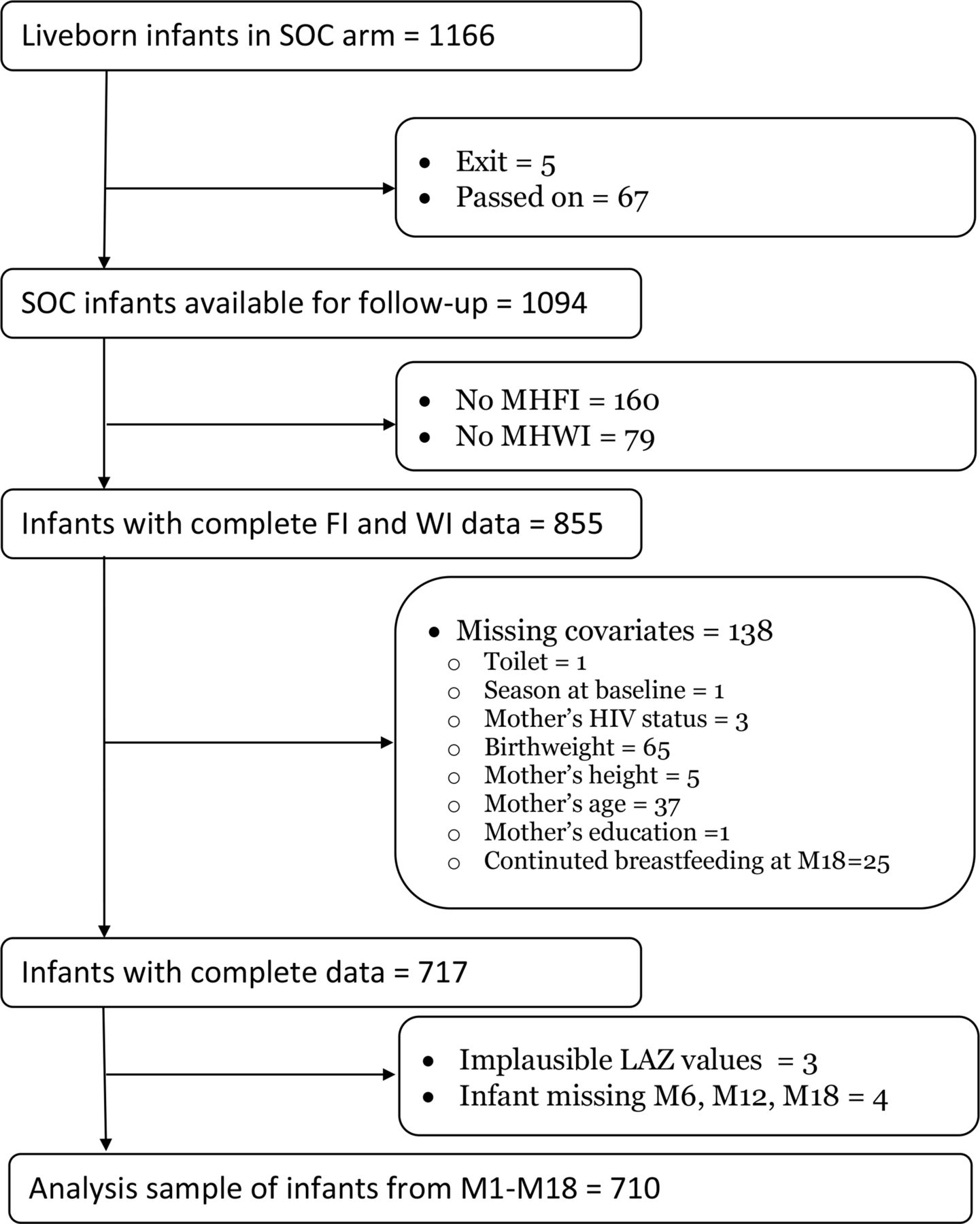{kind=link}
Selection of infants for inclusion in growth analyses. LAZ: Lengthforage Zscore, SOC= Standard of Care; FI= food insecurity; WI= water insecurity; MHFI= Multidimensional Household Food Insecurity; MHWI= Multidimensional Household Water Insecurity; M1, M3, M6, M12, M18= 1, 3, 6, 12, 18 months.
Description of infants, their caregivers and households included in analyses
LAZ, LAZ trajectory and FI
Of the three FI dimensions investigated, the dimension of ‘low food availability & quality’ was the only one associated with LAZ from M1 to M18 in both growth curve models (table 3): βMIN-AM= −0.09; 95% CI −0.17 to –0.01 and βFULL-AM= −0.09; 95% CI −0.17 to –0.01. However, there was no association between any FI dimensions and M1-M18 LAZ trajectory. In growth models from M6 to M18, poor food access (βMIN-AM= −0.12; 95% CI −0.21 to –0.03; βFULL-AM= −0.11; 95% CI −0.20 to –0.03) was associated with lower LAZ, but LAZ trajectory was still not associated with any FI dimension. In post hoc analysis where we explored length instead of LAZ, we found an association between the low food availability and quality dimension and M6–M18 length trajectory (βMIN-AM= −0.03; 95% CI −0.05 to –0.01; online supplemental table S1). However, after adjusting for time interactions with continued breastfeeding until M18, maternal height, infant sex and infant birth weight the association was no longer significant (βFULL-AM= −0.02; 95% CI −0.04 to 0.00).
Supplemental material
Association of infant LAZ and LAZ trajectory with food insecurity and water insecurity
LAZ, LAZ trajectory and WI
None of the WI dimensions were associated with LAZ or LAZ trajectory from M1 to M18, nor from M6 to M18 (table 3).
Discussion
This study examined the associations of household FI and WI on linear growth and growth trajectory of infants from 1 to 18 months of age in rural Zimbabwe. We found evidence that FI, but not WI, is negatively associated with LAZ among these infants. We found no associations of FI or WI with LAZ trajectory (or growth velocity), quantified via time interactions with FI and WI.
Growth, growth trajectory and FI
Two FI dimensions were associated with growth faltering: low food availability and quality (M1–M18), and poor food access (M6–M18). We found no relationship between FI and growth trajectory. These FI results are consistent with some prior literature.
Among cross-sectional studies of the association between food (in)security and LAZ, some show no association,30–34 69 while others show lower LAZ or stunting prevalence.23–26 28 29 34 To our knowledge, only one other longitudinal study investigated the relationship between food security and indicators of infant growth and growth trajectory.21 The Maternal and Infant Nutrition Intervention in Matlab study in rural Bangladesh enrolled women during their pregnancy and followed their infants monthly from one to 24 months after birth.21 Consistent with our results, it found a trend for higher LAZ values with increasing household food security levels, categorised into quartiles (p<0.01). However, the LAZ trajectory remained the same across all four categories of food security.
Contrary to our hypothesis, we found no evidence for an association between FI and LAZ trajectory. This finding suggests that during the first 18 months after birth, FI did not contribute to the deterioration in LAZ trajectory over time among Zimbabwean infants. Nevertheless, this does not mean that absolute length deficits do not worsen with increasing FI. For instance, in the above-mentioned study among Bangladeshi infants, the multilevel models for change showed that infants from food secure households were on average 0.08 cm taller, and had a better growth trajectory based on absolute increase in length (+0.01 cm per month), compared with food insecure infants in that population.21 It has been suggested that inconsistencies in growth findings across studies may be due to the parameterisation of the anthropometric measures. It has been recommended that absolute length-for-age differences (ie, differences between two time points), rather than LAZ or length, may be more efficient at quantifying growth trajectories.70 However, others suggest divergent approaches with different statistical methods and anthropometric parameterisation to better capture the growth faltering phenomenon.71 It is also worth mentioning that households, in the event of FI, may employ certain behaviours to ensure that the children are fed. In post hoc analyses, households’ who were insecure for the three FI dimensions reported coping behaviours such as hunting or gathering wild foods, harvesting green maize, sending children to eat elsewhere, and reducing adult consumption so that there is sufficient food for children. These practices may explain the lack of association between some of the dimensions of FI and LAZ or LAZ trajectory.
Household FI could influence infant growth in multiple ways. As indicated by the FI dimensions identified in our study, different aspects of FI may be important for growth at various times and even in different settings. For example, the low food availability and quality dimension was made up of variables related to quantity of staple food in stock for the household, whether the household had a garden, and whether the household members were able to eat diverse foods; whereas the poor food access dimension was made up of food insufficiency, unavailability of preferred food and insufficient resources to obtain food. Households without a garden are less likely to have infants meeting their nutrient adequacy, which can negatively influence growth.72 The FI experiences of not having sufficient quantities of food, resources to obtain food, and in rural areas, not having staple foods stored for the lean season, may be associated with poor maternal nutritional status,73–75 maternal depressive symptoms,76–79 feelings of inadequacy of mothering ability80 and intimate partner violence.81 82 These factors may contribute to poor parenting, caring and infant feeding practices,67 83–86 which potentially mediate the association from FI to poor infant growth.87–89
Our results may not be directly comparable to other studies because our FI indicators are different from what is commonly used for assessments. First, we have used distinct indicators for separate FI dimensions, while most previous studies have used experience-based and unidimensional measures of FI such as HFIAS or HDDS.90 Second, some studies have only found associations between severe FI and growth, but not at low or mild FI levels.23 32 33 91 Third, the choice of growth parameterisation varies from continuous LAZ, stunting or severity of stunting. Fourth, as discussed above, our longitudinal findings may not be directly compared with the existing cross-sectional studies that mostly account for anthropometric measurement at a single time point. Fifth, the age range of infants in the available literature is primarily from 6 months to 5 years old, while our infant sample was followed from 1 month to 18 months, which is within the critical period of 1000 days of life.
Growth, growth trajectory and WI
We found no evidence of associations between dimensions of household WI and infant growth or growth trajectory from 1 to 18 months of age. This was contrary to our hypothesis that poor water access, poor water quality and low water reliability would be associated with lower LAZ and deteriorating LAZ trajectory.
Traditionally, the contribution of water to infant growth faltering has been investigated in relation to the increased risk of diarrhoeal diseases, and linked to poor sanitation and hygiene.37 92 Both observational and experimental studies have investigated the association between various indicators of water quality and growth faltering, with mixed results. For instance, cluster-randomised trials in Bangladesh39 and in Kenya40 both concluded that their household drinking water treatment interventions with chlorine had no effect on LAZ at the end of 2 years of follow-up. Conversely, Demographic Health Survey data from 70 LMICs showed that compared with surface water used as drinking source, high quality (piped or bottled; OR 0.92, 95% CI 0.89 to 0.94) and intermediate quality (boreholes or wells; OR 0.97, 95% CI 0.95 to 0.97) water sources were associated with lower prevalence of stunting among children under 5 years old.43 In an 8 year retrospective assessment, improved water sources (boreholes, wells, piped, tanks, rainwater and other protected sources) were associated with lower stunting at 1 and 5 years in Ethiopia, but not in Viet Nam, India or Peru.93
The difference in results between these studies and ours may lie in the definition of water quality. We characterised water quality using not only drinking water sources, but also the types of water sources used for non-consumption purposes, and the households’ satisfaction with the organoleptic qualities of their main water source (table 1.). In addition, we assessed growth using the continuous LAZ, rather than the dichotomous stunting indicator. Nevertheless, in a combined analysis with more than 500 000 households from 41 LMICs, including Zimbabwe, unimproved water access (water source off-plot) was not associated with HAZ.49
Many LMICs have poor water access in that households do not have consistent water supplied directly to their homes,94 and often spend more than 30 min for a single water collection round trip.54 In our SHINE trial, the time taken by households to fetch water was on average 20 min for a round trip, varying from <5 min to more than 1 hour.59 SHINE women reported collecting water less frequently, the longer the time required to fetch water.64 Subnational panel data in 59 countries showed that only water piped directly into the home predicted reductions in stunting (β=−0.142; p<0.01),41 but not other water sources whether piped off-plot or ground. This may be an indication of the ease of water access. In SSA, a 15 min decrease in water fetching time is associated with improved HAZ (β= +0.3; 95% CI 0.2 to 0.3).95 Moreover, in a case–control study in Ethiopia, malnourished children under 5 were more likely than well-nourished children to be from households that had to collect drinking water from sources situated at more than 1 km from the home (OR 4.77; 95% CI 1.01 to 22.71).96 In our analyses, where water access was defined by both distance and time to water sources, we found no association with LAZ.
Our hypothesis that WI is related to growth is based on strong theoretical and qualitative studies that suggest pathways from different water dimensions to child growth. Women are usually responsible for water collection in rural LMICs.97 Pregnant and postpartum women have stated that the high time and physical burdens associated with water collection compromise their pregnancy and birthing experiences, as well as their postpartum ability to properly care for and feed their children.48 49 98 Women in SSA who must collect water outside the home are more likely to leave their young children alone for hours or days at a time.49 Women collecting water are also more likely than their male counterparts to experience bodily pain and injuries.99 100 Pregnant women having to carry large containers of water can experience physical trauma that affects the development of the fetus. Since growth faltering begins in utero, ensuring water security implies ensuring the safety of the pregnant woman and her offspring. Moreover, such activities leave women with less time and energy to engage in economic or agricultural activities that will ensure adequate diet for themselves and their children.48 WI is also disproportionately associated with anxiety and depressive symptoms among women.85 101–103 As the primary caregivers of infants and young children, poor maternal physical or mental health can affect growth via poor infant feeding and other caring practices.48 98 104 Finally, WI results in dehydration and has been shown to affect lactation among Kenyan women105 and breastfeeding practices in other LMICs.48 In the Zimbabwean SHINE population, households had approximately 10 L/person of water in the 24 hours prior to their interview,59 whereas the WHO recommends a minimum of 50 L/day/person to ensure all basic needs.106 For lactating women engaged in even moderate physical activity, drinking water requirement is at least 7.5 L/person.107
It is possible that no true association exists between WI and infant growth. However, it is more likely that the association is obscured by complex socioenvironmental confounders and lack of measures to assess these.108 Zimbabwean households may be implementing coping behaviours that mitigate the negative health outcomes of WI. Some strategies that have been reported in other water insecure LMICs include: (A) varying water sources based on availability of water bodies above or below ground,109 (B) water sharing among neighbours in SSA and in Latin America,110–112 (C) modifying water usage to ensure that the available water lasts longer113 and (D) boiling or treating water for consumption, although chemical water purification is rare among rural Zimbabwean households.114 Truly embracing a broader conceptualisation of household water insecurity that encompass social and behavioural practices for availability, access, quality and utilisation may be necessary to identify pathways towards effective ‘comprehensive’ and ‘transformative’ WASH interventions.
Strengths and limitations
Our study presents multiple strengths. With increasing occurrence of natural hazard events (eg, droughts, floods, cyclones, hurricanes, windstorms, rising temperatures), population growth and disease outbreaks like the COVID-19 pandemic, the prevalence of growth faltering, WI and FI will worsen in the next few years.1 54 115–117 This is predicted to exacerbate all related health and social problems.117 Our study is therefore very timely. To our knowledge, this is the first study to investigate the association between growth and growth trajectory by considering FI and WI simultaneously. By using data from a longitudinal cohort, we were able to use repeated measures of infant growth which constitutes an important strength. For anthropometric data, quality control was ensured by repeated training of the nurses who performed data collection.
Based on our literature review, this study is also the first to use multiple indicators of FI and WI in the nutrition sector. The distinction between the FI and WI dimensions increases our understanding of how specific factors are associated with growth faltering in resource-poor settings. For example, instead of solely looking at the problematic food access experiences, we have been able to identify that food availability and food quality are also relevant contributors to infant growth in rural Zimbabwe. Further breakdown of these dimensions may allow specific targets to be set for improving not only infant growth in this population, but also the environment that contributes to poor health and well-being. Using a dimensional approach may help an interdisciplinary approach with both WI and FI, such that intervening on one aspect does not cause negative burdens on the other. This addresses some critical research gaps highlighted by several expert bodies: the Food and Agriculture Organisation,118 the Joint Monitoring Programme for Water Supply, Sanitation and Hygiene,94 the Development Initiatives,119 and various researchers from the food security, water security and nutrition arena.48 50 120
Our study is not without limitations. First, the MHFI and MHWI measures were collected when mothers were pregnant. Therefore, we assumed that FI and WI were relatively static, and that FI and WI during pregnancy were valid estimates for the postpartum period up to 18 months. There are two seasons for FI and WI in Zimbabwe: lean (or hungry: January to March) and dry (April to October). The seasons are such that at the time that households are the most food insecure, they are also potentially the least water insecure. Therefore, availability, quality, access and household shocks are likely to be affected during the lean season.64 FI during that time is particularly severe for the rural farming communities. This is because the lean period represents low employment opportunities in agriculture and the dwindling of staple food reserves for the household. Similarly, water access, quality and reliability tend to be worse during the dry season.108 120 However, in certain instances, due to heavy rains and run-offs water quality may be poor even during the rainy (or wet) season. Future research will need to investigate these seasonal variations in FI and WI on infant growth. This may be done by measuring FI and WI during the postpartum period, ideally at multiple time points so that they can be explored as time-varying predictors of infant growth. Moreover, WI and its dimensions have been strongly associated with FI in LMICs and in fact theorised to drive FI.50 Previous publications have reported synergistic effects of FI and WI on health outcomes such as anxiety121 and depression.78 122 There is also the potential for the mediating effects of FI in the association between WI and health outcomes.121 Future studies with adequate power should aim at exploring this association.
The second limitation lies in the exclusion of 35% of mother–infant dyads due to missing observations, potentially resulting in selection bias. The higher percentage of preterm infants and poorer breastfeeding practices within the excluded group may have biased our observed association towards the null since those who were included were likely healthier and more adequately fed. However, in sensitivity analyses adding inverse probability weights to account for missingness yielded results consistent with our main findings (online supplemental table S2). In addition, although we controlled for and tested a large set of covariates, we cannot exclude the probability of unknown confounding, especially for growth trajectory. Some factors that could have led to missingness in the intermediate anthropometric measures lie in the fact that our analyses were based on secondary data. The SHINE trial only aimed at collecting baseline (prior to childbirth) household characteristics and infant data at 18 months. Data at the intermediate time points were only collected when mothers and infants were present during home visits.
Conclusion
Linear growth, indicated by LAZ, was consistently poorer among infants belonging to households with higher levels of FI, but not WI. Specifically, poor food availability, quality and access were associated with growth faltering from 1 month to 18 months among Zimbabwean infants. There was no evidence of an association between dimensions of FI or WI on infant growth trajectory over time. Our findings support interventions meant to improve food access, availability and quality in rural resource-poor settings. Further research embracing a broader conceptualisation of WI is needed to understand WI in relation to infant growth.
Data availability statement
Data are available on reasonable request. Deidentified participant data are available from the SHINE Trial team and Zvitambo Institute for Maternal and Child Health Research on reasonable request. Please email webadmin@zvitambo.com for requests.
Ethics statements
Patient consent for publication
Ethics approval
The SHINE trial protocol was reviewed and approved by the Medical Research Council of Zimbabwe (MRCZ) and the Institutional Review Board (IRB) of the Johns Hopkins Bloomberg School of Public Health. Informed consent was obtained from women in writing in the local language (Ndebele, Shona and English).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NK performed the main statistical analyses, wrote the main article including the introduction, methods, results and discussion; NK, LES, C-SL and KK were involved in the conceptualisation of the study hypothesis; LES and JH provided SHINE data resources and funding for the analyses; C-SL and RN provided guidance on all statistical analyses; MNNM, ADJ and JH were involved in the initial conceptualisation of the SHINE study and contributed to the food insecurity planning; RCS contributed to idea generation and provided guidance for the water insecurity hypothesis testing, NVT and FDM provided in-depth cultural and contextual information from the rural Zimbabwean population. All authors were involved in reviewing and editing this manuscript. LES accepts full responsibility for the finished work, had access to the data, and controlled the decision to publish. The authors thank all the mothers, infants and their families who participated in the SHINE trial. The authors gratefully acknowledge the leadership and staff of the Ministry of Health and Child Care in Chirumanzu and Shurugwi districts and Midlands Province (especially environmental health, nursing and nutrition) for their roles in the operationalisation of the SHINE trial procedures. The authors acknowledge the Ministry of Local Government officials in each district who supported and facilitated field operations. We would also like to thank our colleagues at Zvitambo Institute for Maternal and Child Health Research in Harare, Zimbabwe. We also thank all members of the SHINE Trial team for their incredible work (https://doi.org/10.1093/cid/civ844).
Funding The SHINE trial (NCT01824940) was funded by the Bill & Melinda Gates Foundation (OPP1021542 and OPP113707); Department for International Development (DFID), UK; Wellcome Trust, UK (093768/Z/10/Z, 108065/Z/15/Z and 203905/Z/16/Z); Swiss Agency for Development and Coop-eration (SDC); National Institutes of Health, USA (2R01HD060338‐06); and UNICEF (PCA2017-0002). The study funders approved the trial design, but were not involved in data collection, analysis, interpretation, manuscript preparation, nor decisions related to publications. The lead author and corresponding author had full access to the study data included in this paper and ultimate responsibility for the decision to submit this manuscript for publication. NK was supported by the Saxon Graham Research Award of the Department of Epidemiology and Environmental Health, the University at Buffalo, the State University of New York. NK also obtained funding from the Community of Global Health Equity at the University at Buffalo, and the Mark Diamond Research Fund of the Graduate Student Association at the University at Buffalo, the State University of New York to support this work.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed by Christine P. Stewart, UK of Great Britain and Northern Ireland.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.