Article Text

Abstract
Objective Household food insecurity is positively associated with depression; however, the association among adolescents is not well known. We examined the association between household food insecurity and depression among adolescent girls in Northern Ghana.
Methods We analysed data from the Ten2Twenty-Ghana randomised controlled trial end-line for adolescent girls aged 10–17 years (n=582). The girls were chosen at random from 19 primary schools in the Mion District of Ghana’s northern region. The children’s depression inventory and the Food Insecurity Experience Scale were used in face-to-face interviews to assess depression and household food insecurity. Hierarchical survey binary logistic regression and linear mixed models were used to examine the association between household food insecurity and depressive symptoms. We took into account a number of potential confounders in the analysis, such as life satisfaction, self-efficacy, self-esteem, health complaints, child’s age, menarche status, pubertal development, anaemia, stunting, frequency of consuming fruits and vegetables, frequency of consuming animal-sourced foods, maternal age, household wealth index and size, and the intervention group the girl was assigned to in the trial.
Results About 20.1% of adolescent girls were classified as likely depressed, and 70.3% of their households were food insecure, with 22.9% and 18.0% being moderately and severely food insecure, respectively. Compared with girls from food-secure households, those from moderately (adjusted OR (AOR) 2.63, 95% CI (1.35 to 5.12)) and severely (AOR 3.28, 95% CI (1.66 to 6.49)) food insecure households had about three times the odds of being classified as depressed, after controlling for potential confounders. The odds of being likely depressed were about twice for adolescent girls from food-insecure households compared with their peers from food-secure households in both the crude and final adjusted model.
Conclusion The study discovered high levels of household food insecurity and depression in adolescent girls in Northern Ghana, with a dose-response association between the two.
- Mental health
- Dietary patterns
Data availability statement
Data are available on reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Depression is prevalent in Ghana, particularly among the adolescent population and girls. In addition, while household food insecurity is positively associated with depression among adults, little is known regarding the link between household food insecurity and depression among adolescent girls.
WHAT THIS STUDY ADDS
We observed a positive association between household food insecurity and depression among adolescent girls.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The current study's findings highlight the need to provide adolescent girls with constant access to healthy food at home, which could improve food intake and reduce depression or mental .
Introduction
Depression is a common mental disorder and a major public health issue that is the world’s second-biggest cause of sickness and mortality.1 2 Globally, about 322 million people have been estimated to suffer from depressive symptoms, with the highest prevalence occurring among women of reproductive age.2 Mental disorders in children and adolescents, including depression, anxiety and behavioural disorders are estimated to account for approximately 16% of the global disease burden; the prevalence is twice as high in girls as it is in boys, especially in postmenarche girls3; lifetime prevalence rates range from 8% to 16%.4 According to estimates, depression affects one-fourth of the adolescent populations in sub-Saharan Africa.5 In Ghana, depression is on the rise, especially among adolescents.5 6 About 32.5% of adolescents in Ghana’s rural areas experience depressive symptoms.5
The determinants of depression are multifaceted and can be explained by the ‘social determinants of health in adolescents and young women’.7 The framework proposes that socioeconomic status, such as income, education and occupation, as well as national-level policies, are structured determinants of health and well-being. Physical conditions, such as family structure and access to food, as well as behavioural, biological and psychosocial factors, serve as intermediary elements that affect health and well-being. Known correlates of depression among children and adolescents from previous research include older age, sex, low self-esteem, school attendance, school performance, household structure and relations, socioeconomic status and residence.8 9 According to the WHO,3 failing to address adolescent mental health disorders has long-term effects that affect adult opportunities for leading satisfying lives as well as physical and mental health.
Food insecurity is a growing concern since inadequate food intake and nutrition can have a severe impact on adolescents’ and children’s mental health and physical well-being.10 11 A little over one-third of households in Ghana’s Northern Region experience food insecurity, which affects about 1 in 10 households nationwide.12 Household food insecurity has also been linked to low income, bigger family sizes, lower educational status, high food prices and a poor quality of life.13 14 Although the possible mechanism linking food insecurity to poor mental health or depression is unknown, it is hypothesised that the underlying mechanism is related to the influence of insufficient micronutrient intake in the diet. Poor myelination and diminished oligodendrocyte function are potential mechanisms through which micronutrient deficiencies during adolescence may cause behavioural problems.15 Iron deficiency has been demonstrated to change the metabolism of neurochemicals in the hippocampus, including phosphocreatine, glutamate, N-acetyl aspartate, aspartate and aminobutyric acid, which may result in some cognitive and mental problems. A previous study found a link between micronutrients and depression as well as their importance in brain physiological functions.16 For optimum health, enough micronutrient intake is essential, notably iron, zinc, vitamin A and B vitamins, including folate and B12, as well as vitamin C.17 18 Antioxidant micronutrients, in particular, have been shown to promote mental wellness.19
Data on the association between food insecurity and depression in sub-Saharan Africa is scanty. However, one recent study in France found an association between household food insecurity and depression among young adults aged 18–36 years.20 A qualitative study in San Francisco found that food insecurity contributes to psychological distress among children aged 7–14 years.21 In the present study, we examined the association between household food insecurity and depression among adolescent girls in Northern Ghana. We hypothesised that household food insecurity is positively associated with depression among adolescent girls.
Methods
Study area
The research was carried out in the Mion district, which is located in the north-eastern corridor of Ghana’s northern region.22 Farming is the primary source of income for more than 90% of people in the District; the illiteracy rate is very high (~71%) for both males and females.22 The World Food Programme estimated in 2020 that about 46% of households in the district experience food insecurity.12
Study design
We analysed data from the end-line survey of the Ten2Twenty-Ghana randomised controlled trial (RCT) among adolescent girls aged 10–17 years. The data were collected in September 2019, at the beginning of the farm harvest season. In brief, Ten2Twenty-Ghana was a 26-week RCT in which premenarche and postmenarche adolescent girls were randomly assigned to eat either multiple-micronutrient-fortified biscuits or unfortified biscuits 5 days per week. Data on participants’ nutritional status, psychosocial and behavioural aspects, maternal factors, and household factors were all included in the study using one-on-one interviews. We employed a sample of 582 girls who completed the RCT and had comprehensive data on the outcome (depression), exposure (household food security status) and covariates. The neighbouring Yendi Municipality served as a pretest site for the questionnaire. Because some questions on reproductive health were sensitive, interviewers were trained ladies recruited from the University for Development Studies, Tamale, Ghana. Throughout the fieldwork, supervisors checked and validated every questionnaire for consistency and completeness. The sample size selection and data collection are described in detail elsewhere.23 The RCT was also prospectively registered with the Netherlands Clinical Trials Register (NL7487). Parents and guardians signed/thumb or thumbprinted informed consent for their girl to participate in the study. The girls also signed to give their informed assent before participating in the study.
Study population and population for analysis
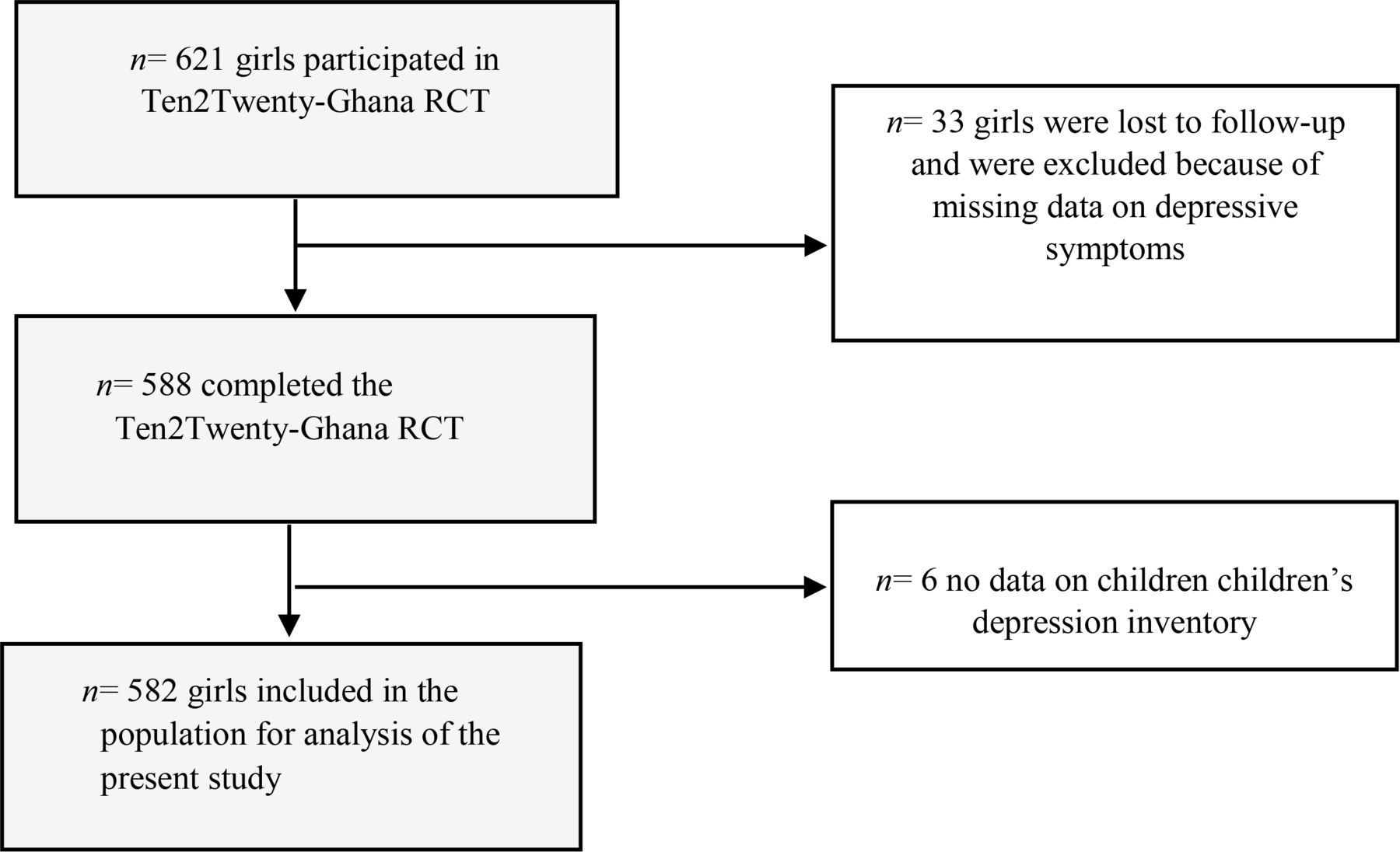
In brief, adolescent girls were selected from 19 different primary schools across the Mion district. Four clusters were included in the sampling, where 15 larger schools from the rural area and 4 urban schools were selected. Based on a 16-item questionnaire, premenarche or-postmenarche girls who were not pregnant, not lactating and healthy with no clear sign of poor health were first selected for a survey (n=1057). Girls (n=621) who met additional criteria, such as not being seriously anaemic or severely underweight, being willing to consume biscuits for 6 months, and having their parents' informed consent, were then enrolled in the RCT. The RCT subjects who were lost to follow-up and/or without data on depression (n=39) in the end-line survey were not included in this study. Figure 1 demonstrates the selection process for the study’s population.
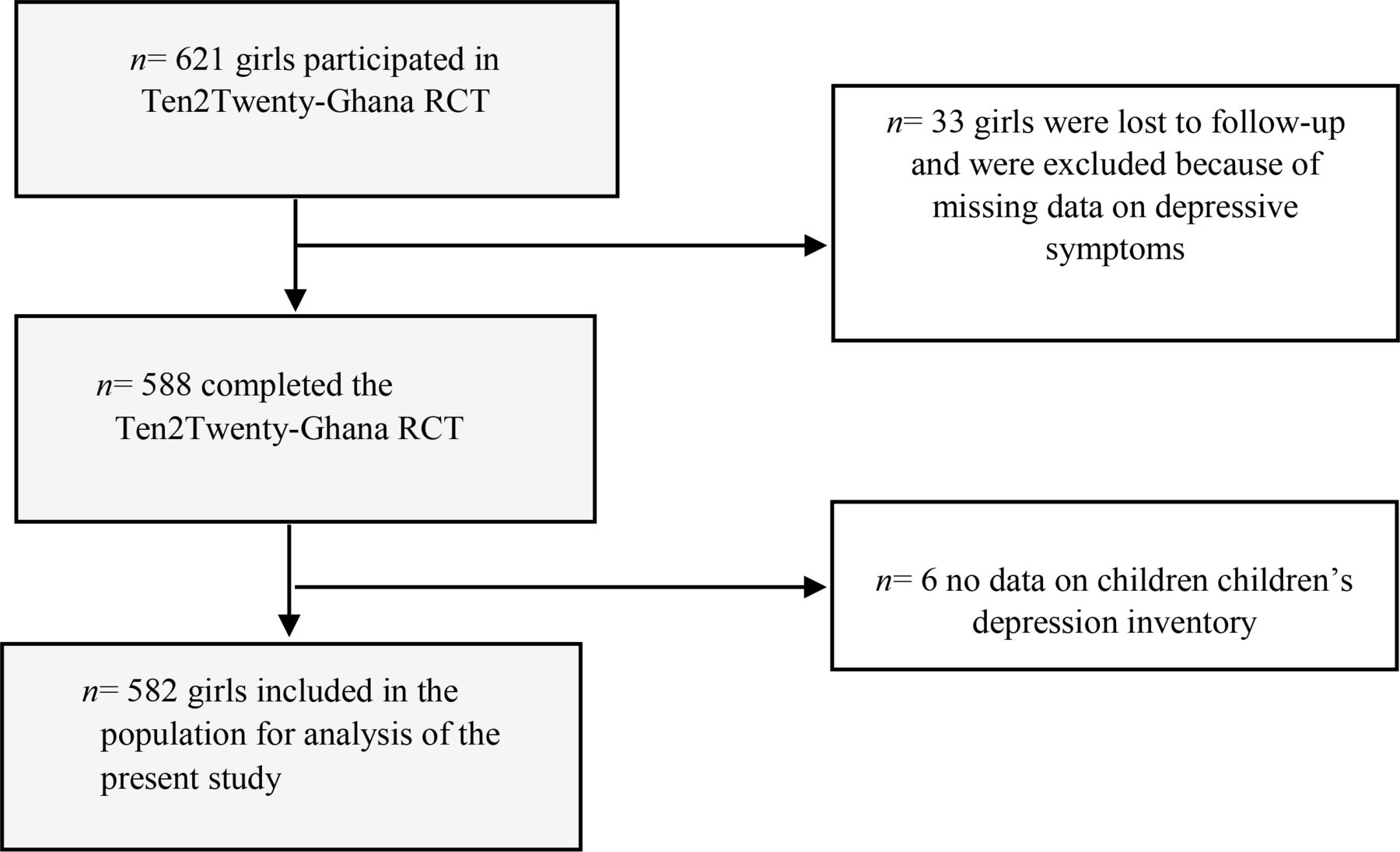
Selection of the population for analysis from the Ten2Twenty-Ghana randomised controlled trial.
Dependent variable
Depressive symptoms: The Children’s Depression Inventory (CDI)24 was only used to assess depression at the end-line. The CDI is a 10-item questionnaire with three Likert scale ratings: ‘once in a while (0)’, ‘many times (1)’ and ‘all the time (2)’. A summed CDI score ranging from 0 to 20 was calculated based on the 10 items, with a higher score indicating more depressive symptoms and a score of 0 indicating no depressive symptoms. A binary variable was also created whereby girls with a CDI score greater or equal to three (CDI score ≥3) were classified as likely depressed, whereas those with a CDI score of less than three (CDI score <3) were classified as not likely depressed; the cut-off point has been shown to have high sensitivity (>90%) and specificity (>70) in diagnosing depression with the CDI.25
Independent variable
We used the Food Insecurity Experience Scale (FIES)26 to determine the household food security status of the girls. The FIES presents the behaviours and self-reported experiences related to food access owing to the absence of money and other resources for 12 months. The scale consists of eight yes/no questions ranging from minimal food insecurity (question 1) to severe food insecurity (question 8), with a yes response receiving a score of 1 and a no response receiving a score of 0. Overall scores ranging from 0 to 8 were calculated from the responses. FIES was divided into four groups, with scores ranging from 0 to 2 indicating food security, 3 to 4 indicating mild food insecurity, 4 to 6 indicating moderate food insecurity and 7 to 8 indicating severe food insecurity. In a dichotomous variable, households with mild, moderate or severe food insecurity were defined as food insecure (ie, FIES ≥3), and households without any form of food insecurity were classified as food secure (ie, FIES <3).
Covariates
We chose girl-level, maternal-level and household-level probable confounding variables for the link between household food insecurity and depression based on the conceptual framework and the available data. In the paragraphs that follow, these confounding variables are detailed under the subheadings ‘girl-level’, ‘maternal-level’ and ‘household-level’ factors.
Girl-level factors
Anthropometric measurement
We used WHO Anthro Plus (V.1.0.4) to calculate the girls’ height-for-age z-scores (HAZ) and body mass index-for-age z-scores (BAZ) based on their age, height and weight, as well as the WHO 200727 growth reference for adolescent girls aged 10–19. Stunting was defined as HAZ <−2, thinness as BAZ <−2, normal weight as −2 SD≤BAZ ≤+1 SD, overweight as +1 SD<BAZ<+2 SD and finally obesity as BAZ≥+2 SD.27 In the analysis, overweight and obesity were combined as overweight/obesity.
Anaemia
Using a sample of venous blood and the HemoCue 301 (Angelholm, Sweden; 1 g/L precision), trained phlebotomists from the Tamale Teaching Hospital determined the adolescent girls’ haemoglobin (Hb) concentration. Anaemia was defined as Hb <115 g/L for girls aged <12 years and Hb <120 g/L for girls with age ≥12 years.28 The severity of anaemia was classified as mild (110 g/L≤Hb ≤119 g/L), moderate (80 g/L≤Hb ≤109 g/L) and severe (Hb<80 g/L).28
Demographic characteristics of the girl
The demographic parameters of the girls included age, coded as a continuous variable, as well as ethnicity, religion and educational status, which were all coded as categorical variables. Other child-level factors included literacy (dichotomous) and school attendance for the academic year (continuous).
Dietary intake
We used a 10-food-group indicator from a qualitative 24-hour dietary recall to assess the adolescent girls’ dietary diversity. If the girl ate at least one food item from the food group, she received a score of ‘1’ and if she did not consume any food items from the food group, she received a score of ‘0’. A dietary diversity score (DDS) was created by summing individual food group scores, ranging from a minimum attainable score of 0 to a maximum of 10. We defined the minimum DDS (dichotomous) as having a DDS of at least 5. The data also included the frequency of consuming fruits, vegetables and animal-source foods (ASF) in the last month using a 1-month semiquantitative food-frequency questionnaire. The food-frequency questionnaire captured the frequency of consumption of food items from the 10-food group indicator in the last month.
Behavioural level factors
In conformity with Haugland et al,29 a subjective-health complaints score was calculated. The score ranged from a minimum of 0 to a maximum attainable score of 32; a higher score implied better health. The girls were also ranked into high (≥6) and low (≤ 5) life satisfaction categories based on their scores on a life-satisfaction ladder.30 The 8-item self-efficacy scale31 assessed the self-efficacy of the girls; the scale uses a 5-point Likert scale ranging from ‘strongly disagree’ (1) to ‘strongly agree’ (5). A summated self-efficacy score ranging from 8 to 40 was computed for each subject by summing each subject’s scores for the 8 items; a higher score represented a higher self-efficacy. Additionally, self-esteem was assessed with the Rosenberg 10-item self-esteem scale.32 The scale uses a 4-point Likert scale, which ranges from ‘strongly disagree’ (1) to ‘strongly agree’ (4). A summed score of self-esteem ranged from a minimum of 10 to a maximum of 40; a higher score indicated higher self-esteem for the subject. The self-reported Pubertal Development Scale (PDS)33 34 assessed pubertal development. Pubertal category scores were computed as the mean score, using the scoring algorithms of Crockett and Petersen.34 The score varied from a minimum of 1 to a maximum attainable score of 4. Finally, the menarche status (dichotomous) of the girls was based on the recall method.33 34
Maternal-level factors
Maternal covariates included parity of the mother (continuous), age of the mother in years (dichotomous), literacy (dichotomous) and occupation of the mother (categorical).
Household-level factors
We assessed the household-level factors of the girls with a household rooster, including household size (continuous), female-to-male sex ratio, dependency ratio and household literacy ratio. We also assessed the household’s socioeconomic status using the International Wealth Index (IWI), which ranges from a minimum score of 25 to a maximum attainable score of 100.35 The IWI ranks households based on the ownership of durable assets such as TV, refrigerator, phone, bicycle, car, household utensils classified as cheap (<US$50) or expensive (>US$300), access to electricity, the type of water and toilet facilities used by the household and the material of the floor.
Data analysis
Data from the present study were analysed using SPSS V.23.0 (IBM). The characteristics of the sampled population were presented as frequencies and percentages for categorical variables, while means and SD were calculated for continuous data. Normality histogram curves as well as Q-Q plots were used to examine data normality. We assessed the association between household food insecurity and depression using survey binary logistic regression. The complex sample module in SPPS was used, in which the school was included as a stratum. In the linear mixed model analysis, the school was included as a random intercept. In the analysis, household food security (food secure or mild, moderate, or severe food insecurity) was the exposure variable; the analysis was repeated after reclassifying the households as food secure or food insecure. The outcome variable for the analysis was a binary variable for the depression status of the girl (likely depressed or not). The variance inflation factor <10 and tolerance values <0.1 were used in a linear regression step to assess multicollinearity between the independent variables.
Six hierarchical models were evaluated, controlling for child-level, maternal-level and household-level confounding variables, which were identified a priori based on literature.8 9 Model 1 included only the main exposure variable (household food insecurity). Model 2 was adjusted for child psychological factors such as life satisfaction, self-efficacy, self-esteem and health complaints; model 3 was adjusted for additional child-level factors such as the child’s age, menarche status, PDS, anaemia, stunting, frequency of consuming fruits and vegetables and frequency of consuming ASFs; model 4 was further adjusted for maternal age. Model 5 was adjusted for household factors, including wealth index, and household size. Model 6 finally adjusted for the intervention group (MMB or UB) the girl was assigned to in the trial. Despite having data on the mother’s parity, an index of maternal decision-making, and the mother’s education, literacy and occupation, we did not control for these variables in our statistical models due to their homogeneity. Similarly, we did not control for the sex of the household head due to homogeneity in the data. Finally, we conducted a sensitivity analysis using a linear mixed model analysis in which the outcome variable was replaced with a log-transformed (Ln) variable of the depressive symptoms score of the girls; the log transformation was used to normalise the data.
Results
Sociodemographic and household characteristics of the girls
The average age of the adolescent girls was 13.8±1.9 years (table 1). The mean DDS was 5.7±1.1 food groups, with about 88.1% meeting the minimum dietary diversity for women of reproductive age. The mean frequency of consuming fruits and vegetables in the last 30 days was 15.9±4.9 days, and the mean frequency of ASF consumption over the last 30 days was 9.8±3.5 days. Many of the girls (63.4%) had higher life satisfaction, and the mean scores for self-esteem, self-efficacy and health complaints were 33.6±3.3, 29.8±5.5 and −0.9±2.9, respectively. The average PDS was 2.1±0.7. About half of the girls (48.5%) were postmenarche. The average household size was 12.1±5.3, with a 1.6 female-to-male sex ratio. Additionally, the household dependency ratio, and household literacy ratio were 1.1±0.8 and 0.6±0.3, respectively (table 1).
Descriptive statistics of the school children (n=582)
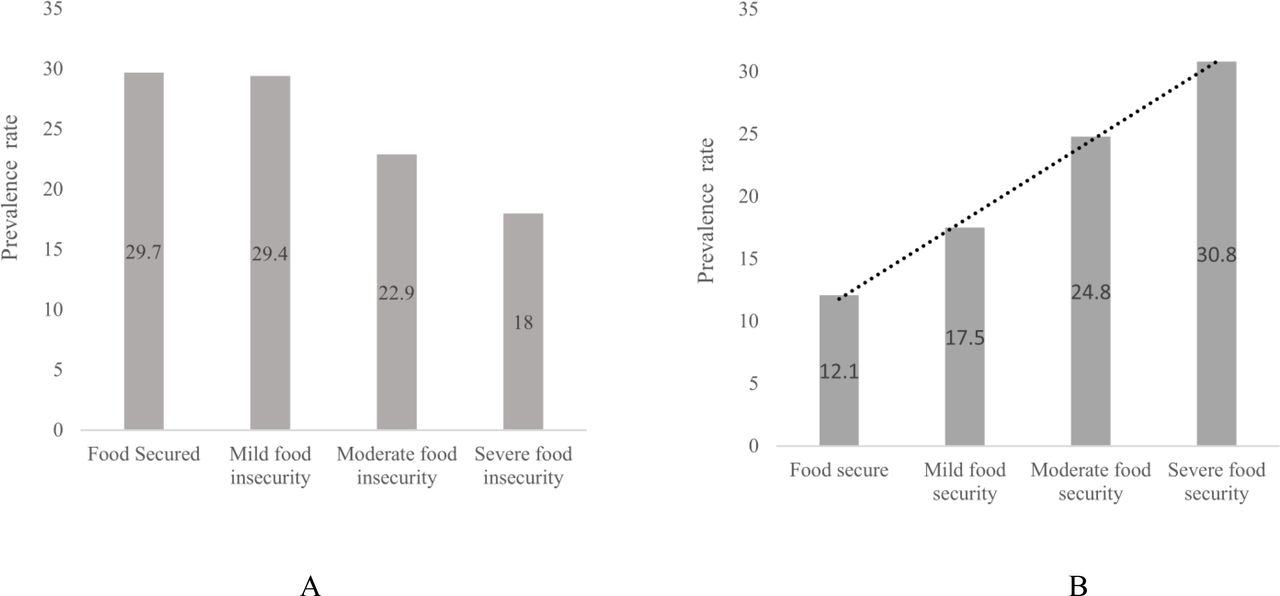
In our study, a little over two-thirds of the girls were from food-insecure households, and one-fifth of them were classified as likely depressed; the prevalence of depression increased with the severity of food insecurity (p=0.001) (figure 2A,B). Adolescent girls from food-insecure households consumed fewer animal-sourced foods in the last month compared with their peers from food-secure households (9.5±3.0 days vs 10.6±4.2 days, p<0.0001). Girls from food-insecure households also had a lower DDS compared with their peers from food-secure households (5.6±1.1 vs 5.9±1.1, p=0.02).
{kind=link}
{kind=link}
The (A) prevalence of household food insecurity (B) and the prevalence of depressive symptoms among the adolescent girls by household food security status.
Association between household food insecurity and depressive symptoms among adolescent girls
Table 2 shows that there was no statistically significant link between mild food insecurity and depressive symptoms in the girls (adjusted OR (AOR) 1.52, 95% CI (0.80 to 2.90)). However, compared with adolescent girls from food-secure households, those from households with moderate food insecurity had almost three times the odds of being likely depressed, and the observed association was statistically significant in all models (AOR 2.63, 95% CI (1.35 to 5.12)). Finally, the odds of being likely depressed were about three times higher among adolescent girls from households with severe food insecurity compared with their peers in food-secure households; adjusting for potential confounding factors did not attenuate the observed association (AOR 3.28, 95% CI (1.66 to 6.49)) (table 2). When households were reclassified as food secure or insecure, adolescent girls from food insecure households had about twice the odds of being likely depressed compared with their peers from food secure households; the adjusted model (AOR 2.21, 95% CI (1.26 to 3.85)) remained similar to the crude model (OR 2.10, 95% CI (1.27 to 3.47)) (table 3). The Wald test statistic for all models was statistically significant with a p<0.0001. The final adjusted model indicating the odds of being likely depressed and the covariates is presented in table 4.
A binary logistic regression analysis of the association between household food insecurity and depressive symptoms among adolescent girls in north-eastern Ghana
A binary logistic regression analysis of the association between household food insecurity compared with food security and depressive symptoms among adolescent girls in north-eastern Ghana
The final adjusted model of the multivariable logistic regression showing the association between household food insecurity and depressive symptoms among adolescent girls
When using linear mixed methods to investigate the relationship between household food security status and depressive symptoms (online supplemental table S1), we found an increasing trend (P-trend=0.0003) in the depression symptoms score as the severity of food insecurity increased, with moderate and severe household food insecurity increasing depressive symptoms by 63.9% (95% CI −18.9% to 146.6%) and 120.9% (95% CI 33.3% to 208.5%), respectively, compared with household food security.
Supplemental material
Discussion
The current study examined the association between household food insecurity and depression symptoms in adolescent girls in Ghana’s Mion district. About 20% of the girls in our study were probably depressed, which is similar to the 22.4% who were identified as having depressive symptoms in a previous study carried out in Ethiopia.36 However, the prevalence is lower than the estimated 32.5% documented for adolescents in rural Ghana by Jörns-Presentati et al.5 Furthermore, the prevalence of household food insecurity (70.3%) was higher in our study compared with the national rate of 12% and an estimate of about 46% for the district.12 Poor socioeconomic status, as reflected in the low scores of the IWI, may explain our finding; poverty is a known determinant of food insecurity as the poor have low purchasing power and are unable to reliably meet their dietary intake requirements. Although the survey was conducted at the start of the farm crop harvest, the peak harvest period is often in October and November, implying most farm produce was still not available. Overall, the high prevalence of food insecurity in the study area emphasises the need for targeted intervention programmes to improve household food security. Skills training and revenue generation to promote household economic access, as well as agricultural interventions to boost household agricultural productivity for year-round availability of food, are examples of such programmes.
The results of the current investigation revealed a positive association between household food insecurity and depressive symptoms among adolescent girls. Regardless of the statistical strategy utilised (logistic regression or linear mixed approaches), the observed association remained, which was consistent with previously conducted studies among adults.20 36 The mechanism behind the link between household food insecurity and depressive symptoms in adolescents remains unknown. However, previous research has shown that psychological stress can be caused by uncertainty in the household food supply; children’s awareness of the unstable food supply and efforts to regulate it can be destabilising, leading to depressive symptoms.21 Furthermore, food insecurity is a known determinant of dietary and nutrient inadequacies, and research has shown that poor micronutrient intake may result in behavioural issues via poor myelination and reduced oligodendrocyte function.15
Furthermore, food insecurity may cause financial issues in the home, which may lead to cultural sensitivity and poor mental health.37 In addition, good mental health, including not being depressed, necessitates adequate micronutrient intake, such as iron, zinc, vitamin A, B vitamins and vitamin C.17 18 Antioxidant micronutrients have also been shown to greatly boost mental health.19 Because our study used data from the endpoint of a RCT, we included the intervention effect (MMB vs UB) as a covariate, but this had no effect on the odds of being likely depressed. In reality, the primary outcomes of the trial included micronutrient status, and we did not anticipate any effect of the trial on depression within 6 months.
Recent studies show that adolescents who experience food insecurity are more likely to eat fewer fruits and vegetables, fewer ASFs, skip breakfast and family meals, consume fast foods and drink high-sugar beverages, restricting their access to healthier foods and adequate nutrition.38 However, eating fruits and vegetables and consuming ASFs were not associated with depression in this study. According to a prior study, DDS is linked to depression.39 However, when included in the statistical models, it was not a significant covariate, and the model fit was better with the food frequency data for fruits and vegetables and ASF consumption. The DDS in this study reflects recent or current dietary consumption rather than habitual dietary intake, which is more valuable for causal inferences.
We included several potential confounding factors in the association studied, including girl-level psychosocial and demographic factors, as well as mother-level and household-level factors. However, none of the maternal or household-related covariates was associated with depressive symptoms in the girls. Although not the focus of the present study, increasing age, a higher health complaints score, and lower self-esteem all increased the likelihood of the girls being likely depressed. On the contrary, higher life satisfaction was associated with lower odds of being likely depressed.
The findings of the current study highlight the need to provide adolescent girls with constant access to healthy food at home, which could improve food intake and reduce depression related to food access. To address food insecurity and depression, intervention initiatives should target economically disadvantaged households and incorporate coping and broad mental health measures.
Some limitations of the present study should be considered when interpreting our findings. First, a cross-sectional survey, based on the end-line data of the Ten2Twenty Ghana RCT, was used to assess the association between household food insecurity and depressive symptoms among adolescent girls; this makes the inference of causality speculative, and our findings are limited to the description of observed associations. Second, some portions of the data, including food patterns, dietary diversity and household food insecurity, may be subject to short-term memory bias. However, regarding dietary intake and household food insecurity, the mother assisted the girls when it was necessary.
The findings of the present study may not be extrapolated to the whole of Ghana or to include boys, as only girls were sampled. While only school-going adolescent girls were selected, most adolescents are presently enrolled in school; hence, the study population may be generalised to all rural adolescent girls in northern Ghana and similar settings. To our knowledge, this is the first study in sub-Saharan Africa to examine the association between household food insecurity and depression among adolescent girls.
Conclusion
This study found high levels of both household food insecurity and depression among adolescent girls in Northern Ghana, with the two showing a dose–response association. Food security programmes may help adolescent girls’ mental health by preventing depression. The government and other stakeholders should pay special attention to improving food security and developing intervention measures to prevent and cure depressive symptoms among adolescent girls.
Data availability statement
Data are available on reasonable request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Navrongo Health Research Centre Institutional Review Board (NHRCIRB323). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @boahmichael
Contributors Conceived and designed the study: FA and IDB. The data were collected by FA and IDB. NS and FA did the statistical analysis; wrote the first draft of the manuscript: NS, FA and AW. IDB, HYAY and MB both contributed to the writing of the manuscript. Guarantor: FA. All authors approved of the final content.
Funding There is no funding for the present study. The data analysed were collected as part of the lead author’s completed PhD research project in 2019. The PhD project was funded by the Edema Steernberg Foundation, Judith Zwartz Foundation, Nutricia Foundation, and Sight, and Life Foundation. None of the funders contributed to the study design, conduct, analysis of the data, interpretation of findings, or the preparation of this manuscript.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed by Emmanuel Baah, University of North Carolina System.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.