Article Text

Abstract
Background Diabetes care has traditionally not included nutrition therapy using carbohydrate restriction, nor has carbohydrate restriction been taught to registered dietitians (RDs) to support patients living with diabetes choosing this dietary approach. We aimed to describe the experiences and views of RDs caring for patients using therapeutic carbohydrate-restricted diets (TCR), particularly metabolic conditions such as type 2 diabetes or prediabetes.
Subjects/Methods A qualitative study design using free-text responses from an online needs assessment survey was employed. RDs who practised in Canada were invited (n=6640) and 274 completed the survey, with 45 respondents who regularly prescribed TCR to their patients providing open-text responses (2987 words), which were analysed using inductive thematic analysis.
Results We identified four themes characterising Canadian RDs’ experiences around prescribing TCR: interpersonal context, personal experience/knowledge, regulatory environment and patient-centredness. While these themes often interacted, each impacted TCR prescription uniquely, with patient-centred care at the core of reported experiences of prescribing.
Conclusions There exists a variety of experiences and perspectives related to prescribing of TCR among Canadian RDs caring for patients with diabetes, and all focus on the patient’s needs, benefits and preferences. Prescribing TCR was often informed by the scientific literature yet also by RDs’ experiential knowledge. Responses highlighted a desire for evidence-based educational materials and greater discussion within the diabetes nutrition community on this topic.
- diabetes mellitus
- nutritional treatment
- precision nutrition
Data availability statement
All relevant data are provided in the manuscript and appendices.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients living with diabetes can benefit from personalised therapeutic nutrition to help manage their condition.
Growing research suggests that some patients living with diabetes may benefit from therapeutic use of carbohydrate (CHO) restriction, but clinical practice guidelines have previously not accepted this dietary approach.
WHAT THIS STUDY ADDS
We thematically analysed written responses from 45 RDs who described their experiences of prescribing CHO restriction to their patients living with metabolic conditions including type 2 diabetes.
Dietitians’ experiences of prescribing CHO-restricted diets to patients living with diabetes were driven by the interpersonal context, personal experience/knowledge, regulatory environment and patient-centredness.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study showed that RDs, along with their healthcare professional colleagues, will need advanced training, interdisciplinary support and strong communication strategies to confidently and safely prescribe CHO-restricted diets.
Continuing education and clinical resources on CHO-restricted diets will be a critical next step towards improving care for patients with diabetes or other metabolic conditions in Canada.
Introduction
Diabetes rates in Canada increased 70% since 2000, and one in three Canadian adults were estimated to have diabetes, prediabetes or undiagnosed diabetes in 2020, with an expected cost to the Canadian healthcare system of $C16 billion in 2020.1 Lifestyle modificationis critical to diabetes management and outcomes are better when patients have access to diabetes educators of any healthcare profession.2 Registered dietitians (RDs) have an important role to play as part of a multidisciplinary team to support patients living with diabetes, however RDs have limited opportunities to support patients with metabolic conditions using carbohydrate (CHO)-restricted diets (specifically below 130g/day CHO) until the change in Canada’s clinical practice guidelines (CPGs) in Spring 2020.3
CHO restriction is increasingly considered a viable treatment option for insulin-resistant conditions such as obesity, type 2 diabetes (T2D) and polycystic ovarian syndrome.4–8 Therapeutic use of CHO restriction (TCR) encompasses any dietary intervention that involves the consumption of <45% of total energy coming from CHO with the level of restriction depending on individual tolerance. While other definitions of CHO restriction exist,9 the Acceptable Macronutrient Distribution Ranges for CHO (45%–65% of total energy), fat and protein was established since 2005 by the Food and Nutrition Board of the Institute of Medicine.10 Extreme CHO restriction has been practised in Western medicine since 1921 for the treatment of childhood epilepsy.11 A lack of CPGs for CHO-restricted diets until 2020 has meant that Canadian RDs had to navigate a conflicting diabetes care landscape: an emerging scientific perspective of neutral-to-positive evidence for CHO-restricted diets in diabetes management3; an existing body of research that is negative-to-neutral3; a traditional clinical perspective of governing bodies (eg, Diabetes Canada, Health Canada) for a Canada Food Guide diet comprising 45%–65% CHO12; and lived experiences of individuals successfully using CHO-restricted diets. Notably, Health Canada’s Food Guide website categorises diets that limit the ‘kinds of food you can eat’ under ‘fad diets’, with dietary advice on why restrictive diets are harmful and how to avoid them.3 Consequently, RDs working in federally funded institutions such as hospitals or care homes have been limited in the extent to which they can recommend or prescribe therapeutic CHO-restricted diets (TCR) for diabetes care, which may impact patient care and health outcomes.
In addition, a lack of clinical support for TCR from other clinicians may also influence an RD’s use of CHO-restricted diets to manage patients living with T2D, which can also lead to inconsistencies in care and treatment outcomes. For example, in an online survey of 2319 active low-CHO dieters, only 56% said their physician was supportive of their choice of diet.13 14 Differences in knowledge and beliefs on therapeutic use of CHO-restricted diets are further compounded by inconsistencies in the evolving scientific literature that make it difficult for RDs to use evidence in their practice and for governing bodies to inform CPGs. These disagreements and mixed results likely stem from a lack of standardisation of the definition and nomenclature of a ‘CHO-restricted diet’,15 specifically: (1) researchers vary widely in the CHO thresholds used to define common terms of ‘low’ or ‘very low’9 16; (2) they differ in the ratio of other macronutrients in the ‘low-carb diet’; and (3) they contrast on the choice of CHO substitution in the diet which has different health effects.7 16 17
Finally, little research attention has been given to the individual RD perspective to better understand an RD’s knowledge, use and information requirements on CHO-restricted diets used in patients living with diabetes and metabolic conditions.13 As a result, current evidence often does not address situations encountered by RDs in healthcare settings,18 and the clinical practice of using CHO-restricted diets for nutrition therapy among Canadian RDs prior to the Diabetes Canada position statement is unknown. Understanding RDs’ experiences of prescribing CHO-restricted diets is a first step to developing new educational resources and tools to support and enhance Canadian RD clinical practice for patients living with T2D and other chronic conditions. The goal of this qualitative study was therefore to explore Canadian RDs’ experiences of prescribing CHO-restricted diets in the conventional diabetes care landscape.
Methods
Participants
Study participants were included if they were RDs currently in practice in Canada. Eligible RDs were invited (n=6640) through electronic list-serves of professional organisations (eg, Dietitians of Canada, Canadian Clinicians for Therapeutic Nutrition Network, the Institute for Personalized Therapeutic Nutrition, Alberta Health Services and a Canadian RD list-serve) and social media RD groups to complete an online semi-structured survey between 1 January 2020 and 31 December 2020. The Institute for Personalized Therapeutic Nutrition funded the survey development by one of the authors (EW), but had no other influence on the study; no other organisation was involved in terms of funding or conducting the study. The survey was titled ‘Therapeutic Carbohydrate Restriction: Assessing Dietitians’ Knowledge, Support Requirements and Barriers’ and was anonymously completed by 274 RDs through the institutionally approved Qualtrics platform (Provo, Utah, USA). The survey had 55 questions with multiple, single-choice or open-text response items on RD demographics, patient demographics, referrals, personal and professional experiences of CHO restriction, TCR information sources, competency level and barriers to prescribing.19 We performed pretesting and pilot-testing of our online survey with five licensed RDs and five nutrition researchers.
Context, data collection and processing
This study focused on the open-text responses to a single survey question about whether TCR had influenced an RD’s practice in terms of prescribing the diet to their patients: 127 had never prescribed TCR; 92 prescribed TCR to a few patients and 45 had regularly prescribed TCR (10 responses were missing).19 There were 47 respondents who wrote more information on how TCR influenced their practice, although one replied they ‘did not understand the question’ and another only stated “changed my whole practice”. This study therefore used qualitative data from the text of the remaining 45 responses which totalled 2987 words (about 64 words per comment). Narrative data were managed and analysed using NVivo software (V.12.6.0 QSR International).
Qualitative data analysis and reflexivity
Written responses were analysed inductively by two coders (AV and KY) using thematic content analysis.20 21 Data analysis involved an iterative process following codified techniques to identify themes and subthemes that emerged from the data and were labelled using language quoted directly from the RDs’ descriptive responses; thus, analysis was not driven by pre-existing coding frames or the researcher’s analytic preconceptions. The first author was a white female dietetic student who had research interests in dietary interventions and the second author was a Chinese female nutrition sciences student who had research interests in diabetes prevention; the third author is a white female RD with clinical expertise in prescribing CHO-restricted diets and the senior author is a white female, mixed-methods researcher with expertise in social nutritional epidemiology and diabetes management evaluation.
The data were read and re-read multiple times by the first author, who also developed initial codes and themes. The first author also developed a reflective report during the coding process to demonstrate self-awareness in the analytical process and enhance qualitative researcher skills. Data were read and coded line-by-line to develop a codebook containing the list of data-driven categories and their definitions (examples from the data); this codebook was used by both coders for the final analytic coding and was iteratively re-organised until consensus was reached among the research team. Thematic analysis consisted of multiple phases of data immersion/familiarisation, coding across the dataset, searching for and re-organising categories, producing a map of provisional (sub)themes and relationships between them, refining themes and finalising analysis.22
Through team discussions, themes were verified or revisited and interpretations were further developed to provide in-depth analysis. Codes were given rich descriptions to facilitate transferability. Discussions occurred between authors throughout the study process to ensure a shared understanding and agreement and to identify and resolve any discrepancies or disagreements in the analytic process. Direct quotes (raw data extracts) from a range of participants provide the evidence to support our interpretation and findings.
Findings
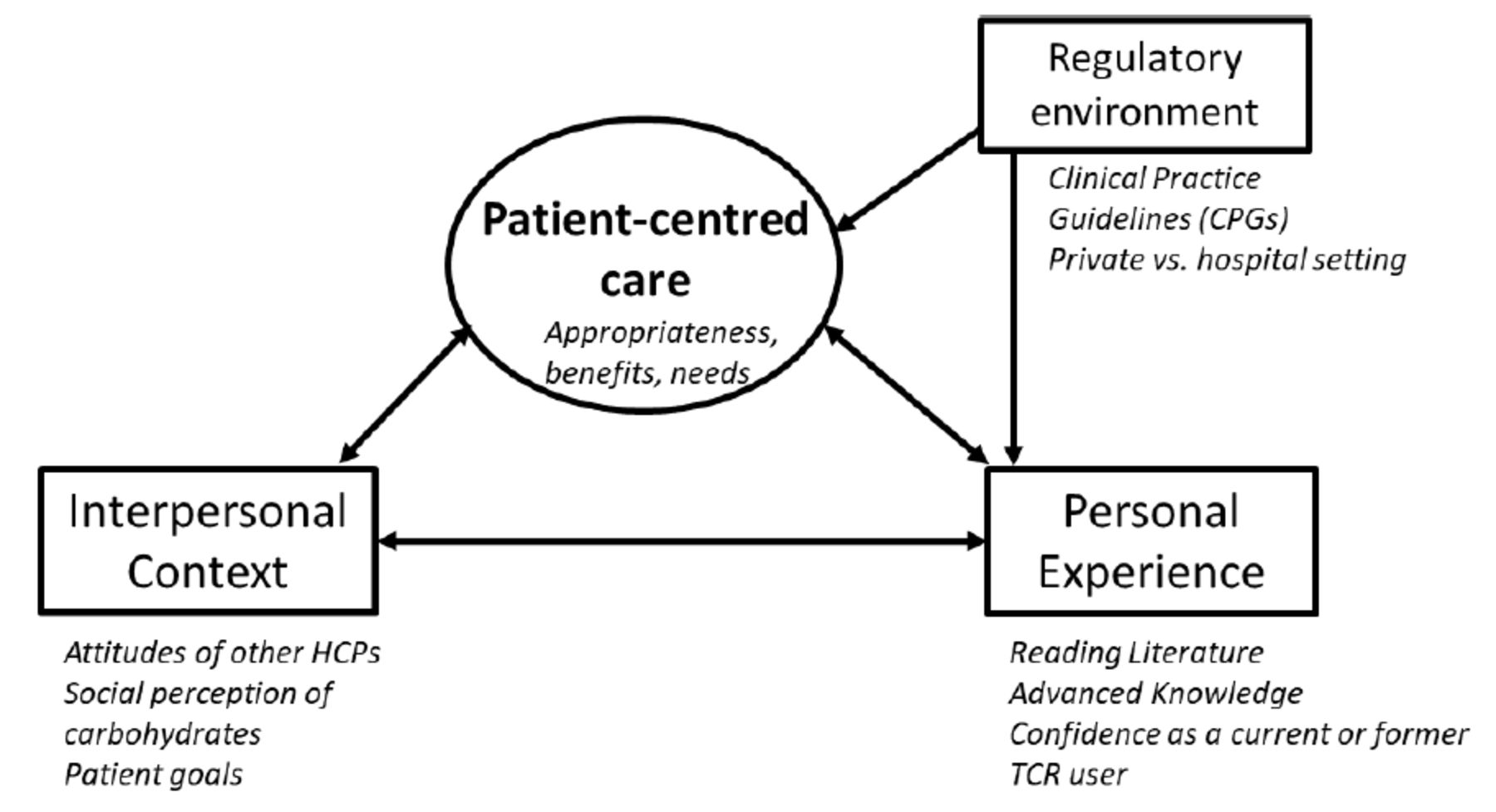
Four main themes emerged related to RDs’ experiences of prescribing TCR: (1) interpersonal context, (2) personal experience and knowledge, (3) regulatory environment and (4) patient-centred care. Table 1 presents exemplary quotes for each theme summarised below. Figure 1 displays these four emergent themes and their inter-relationships.
Main themes and illustrative quotes related to dietitians’ experiences of prescribing therapeutic CHO-restricted diets in Canada

{kind=link}
Diagrammatic representation of four emergent themes related to dietitians’ experiences of prescribing carbohydrate-restricted diets in Canada. Experiences of prescribing therapeutic carbohydrate restriction (TCR) were primarily driven by a patient-centred care (theme 4) approach to nutrition therapy for chronic illness, with key considerations being patient appropriateness, patient benefits and patient needs or preferences. This theme was supported by and mutually reinforcing of the interpersonal context (theme 1), such as the attitudes of other healthcare professionals (HCPs) or social perceptions, and registered dietitians’ personal experience of the benefits from TCR use by patients or themselves, and/or the professional knowledge (theme 2) gained from reading the scientific literature on TCR or teaching the dietary approach to other HCPs. Themes 1 and 2 also appeared to reinforce each other. Professional body practice guidelines and practice setting comprised the regulatory environment (theme 3) that also influenced whether dietitians reported prescribing TCR to their patients living with chronic illness in Canada.
Theme 1: interpersonal context
Participant responses revealed that external factors related to interpersonal context influenced the RD’s decision, or that of their patients, to implement CHO-restricted diets. In particular, the broader social perception, such as ‘the fear of carbs’, was often noted as a factor influencing the RD’s experience of prescribing CHO-restricted diets. Several responses indicated that patients may be influenced by the strongly positive attitudes towards CHO-restricted diets from other healthcare providers (whether or not the diet was appropriate) and that RDs commonly responded by offering multiple, appropriate dietary options. Similarly, interactions with patients appeared to influence whether or not a RD prescribed CHO-restricted diets through the role of patient-centred goals (theme 4, below) with the RD ‘lay(ing) out all the options and the pros and cons’ (table 1). Notably, RDs presented a more critical view of their healthcare colleagues’ involvement in the prescribing of CHO-restricted diets than they presented of their patients’ requests.
Theme 2: personal experience and knowledge
Personal experiences of implementing or using CHO-restricted diets, as well as knowledge of research evidence on CHO-restricted diets, were a key theme related to RDs prescribing CHO-restricted diets to patients in their practice. Some RD responses indicated a good awareness and understanding of the scientific literature in terms of evidence-based care and known benefits for appropriate patients. Notably, having knowledge of the scientific evidence supporting the use of CHO-restricted diets in some patients, led to RDs questioning previous clinical guidelines that “may not have been the best advise [sic] for some of our patients” (table 1). This scientific knowledge was further supported by RDs’ personal experiences of CHO-restricted diets in both practice and personal use. Some RDs noted the direct benefits they saw in their patients who implemented the diet, which contributed to their personal experience in practice. Other RDs gained personal experience from direct use of CHO-restricted diets themselves or among their friends and family. Some responses illustrated a professional confidence in the RD’s knowledge of TCR regarding recommendations around food substitutes and other strategies for dietary implementation; a confidence that enable some RDs to open a private practice to specifically prescribe the diet. Some RDs had knowledge of the complexities of TCR beyond energy and nutrients, including the consumption of processed foods, mental health, physical health and gut microbiota. Finally, some RDs displayed sufficient knowledge and experience to have an educator role, teaching both patients and other professionals about prescribing CHO-restricted diets.
Theme 3: regulatory environment
Several responses concerned RDs’ scope of practice within hospital versus private settings, and suggested that the regulatory environment within Canada acts as a barrier to prescribing CHO-restricted diets. Comments described the conventional model of the CPGs favouring a more liberal intake of CHO and governing the delivery of nutrition care in public institutions, particularly hospitals. Responses around clinical guidelines were either neutral or negative. Some responses even questioned the validity of guidelines. A small number of RDs even described starting a private practice specifically for CHO-restricted diets that would allow for more dietary approaches to manage chronic disease beyond dietary recommendations of Canada’s Food Guide.
Theme 4: patient-centred care
In many responses, patient-centred care was a central feature of RD experiences of prescribing CHO-restricted diets. This included a focus on the health benefits of TCR, the appropriateness for a given patient and the needs and wants of specific clients. Detailed RD responses tended to focus on the characteristics of specific patient populations or on the science of using TCR. More general answers tended to reflect the role of patient preferences in nutrition therapy, with a general reference to how the clients feel and what their interests are as the basis for prescribing CHO-restricted diets. RDs often noted the health benefits of adopting a CHO-restricted diet, either as aspirational or as realised benefits for their patient population.
Most responses that referenced health tended to acknowledge the positive impact of TCR such as reducing postprandial blood glucose. Nevertheless, patient-centred care also entailed that TCR should only be prescribed for specific patients as TCR is more appropriate in some populations and disease states than others. As a result, RDs expressed that the specific patient they see dictates whether they would prescribe a CHO-restricted diet. Responses revealed that RDs aim to find the most sustainable dietary approach for their patients. For example, RDs would consider an appropriate CHO-restricted diet if it is the patient who thinks the diet is ‘enjoyable and sustainable’ (table 1). Both support and reservations among RDs regarding TCR stemmed from patient-centred care, with several respondents indicating that their opinion has changed over time based on patients’ needs or requests.
Discussion
This qualitative study adds novel insights on the experiences of RDs related to prescribing CHO-restricted diets (TCR) to patients with chronic illness in Canada, especially in the context of no pre-existing CPGs. Patient-centred care was a central theme from dietitians’ experiences of prescribing CHO-restricted diets to patients with chronic illness; subthemes focused on patient appropriateness, patient benefits and patient needs or preferences. The use CHO-restricted diets as medical nutrition therapy was also influenced by the interpersonal context, such as the attitudes of other healthcare providers or social perceptions, and by RDs’ personal experiences of the benefits from CHO-restricted diets by patients or themselves, and/or their knowledge of CHO-restricted diets from reading the scientific literature or teaching the diet to other providers. All three themes mutually reinforced one another. Professional guidelines and practice setting were part of the regulatory environment (theme 3) influencing whether dietitians prescribed CHO-restricted diets to their patients living with chronic illness in Canada.
The findings in context
Many factors are known to influence shared decision-making about diabetes care, particularly decisions to prescribe specific diets in patients living with diabetes; personality type,23 different actors (healthcare providers, patients, family)24 and contextual factors25 all affect healthcare decision-making processes. Until recently, decisions to therapeutically use CHO-restricted diets were especially difficult as this dietary choice was absent from the CPGs in Canada.3 Thus, RDs have had to independently navigate this diabetes care decision without formal guidance. This study is the first, to our knowledge, to assess RDs’ experiences of prescribing CHO-restricted diets in the conventional diabetes care landscape in Canada.
Limited research on RD experiences of prescribing other dietary interventions indicates that RDs are more likely to prescribe a given diet (eg, very low-calorie diets) as an intervention when they better understood the particular diet.26 In this study, we found that experiential knowledge was a key factor that influenced RDs’ experiences of TCR; as described in the written responses, such knowledge came from RDs directly observing benefits of CHO-restricted diets in their patients, in themselves and/or in non-clients (eg, family members). RDs also gained knowledge for prescribing CHO-restricted diets through the scientific literature that provided the evidence base to support them in implementing CHO-restricted diets in some patient populations. By corollary and as reported in a descriptive study of the full TCR survey,19 RDs who chose not to prescribe this diet were those who lacked knowledge of CHO-restricted diets or reported having negative beliefs about the diet. Another qualitative study of medical staff in colorectal surgery also reported that perceptions, experience and training combined to influence nutrition prescription preferences.27
Providing patient-centred care was another central and inter-related theme related to RDs’ experiences of prescribing CHO-restricted diets. This theme was most evident from the data of dietitians who reported a willingness to prescribe CHO-restricted diets after patient requests. Nearly half of the responses indicated patient preference played a role in the experiences of prescribing CHO-restricted diets, which is consistent with professional and quality standards for nutrition care.2 Other qualitative research also shows that medical staff modified nutrition prescription practices to align with patient-related factors.27 Patient preferences are likely to continue to grow in future given the 2020 position statement on CHO-reduced diets from Diabetes Canada. Hence, RDs will need to be supported to confidently prescribe and monitor CHO-restricted diets through accessible and accurate resources, educational tools and appropriate training.
Others have also reported that peers influence prescription behaviours and attitudes towards nutrition,27 which is another major theme emerging from this work. The influence of the interpersonal context was most evidence from examples of divergent dietary advice between nurses and dietitians, as reported by the RDs. Some responses suggested that RDs might not prescribe CHO-restricted diets to overcompensate for generic dietary advice based on strong beliefs of other healthcare providers. This disagreement between professionals could have consequences for patient care as research shows that conflicting information lowers patient adherence rates for medical interventions.28–30 Our study findings of the interpersonal context as an important influence on RDs’ experiences of prescribing CHO-restricted diets suggest that the communication between healthcare professionals on nutritional therapy in disease management needs to be improved. The value of having a multidisciplinary team for healthcare quality has been demonstrated in diabetes management, weight loss interventions and care for other chronic diseases.31 Treatment for chronic diseases requires multifaceted interventions that need to be integrated across professional groups including physicians, nurses, pharmacists, dietitians and other health professionals.32
Methodological considerations
Several important considerations must be kept in mind when examining the data collected by the study. First, in April 2020, Diabetes Canada introduced its position statement on TCR. As such, the data may no longer accurately reflect RDs’ perspectives on prescribing CHO-restricted diets, but may reflect RDs’ perspectives for future emerging dietary approaches. Additionally, this paper only analysed the results of one question, and so some context was possibly lost from the broader survey as any answers referencing previous responses were not analysed here. Third, a greater number of RDs responded to the survey than those who provided open-text data for the analysed question (less than half): this is likely due to the fact that open-text questions require more effort, and so responses tend to skew towards those with a strong opinion over those who are neutral or indifferent.33 Fourth, while the online survey was distributed through a range of professional channels, some channels included groups strongly favouring TCR. As a result, our data may not necessarily reflect the broader diversity of RDs in Canada. Fifth, the online nature of the survey also meant that respondents had to interpret the question on their own, resulting in one respondent admitting “I don’t understand this question”. Finally, while our analytic approach was inductive and we used techniques to enable themes to emerge from the data, the qualitative methodology does not preclude that our own perspectives and preconceptions will influence the analysis and contribute to the findings.
Nonetheless, this study has numerous strengths; most notably, it has a large volume of data (nearly 3000 words) that provided a diversity of responses from every province in Canada and internationally. Additionally, the timing of the survey prior to Diabetes Canada’s new position statement allowed an understanding of RDs’knowledge and experience around this dietary approach in a regulatory environment that did not explicitly promote its use in practice. Finally, two researchers separately coded the data, adding strength and validity to this work and study findings.
Practice implications
With the Diabetes Canada release of a new position statement on CHO-restricted diets, there are now guidelines and political support for dietitians to teach and prescribe this diet to appropriate patients. As this study clearly demonstrated, RDs along with their healthcare professional colleagues, will need advanced training, interdisciplinary support and stronger communication strategies to prescribe CHO-restricted diets confidently and safely especially given the medication monitoring required with diabetes and other chronic diseases related to insulin resistance. Moving forward, continuing education and clinical resources around these diets will be a critical next step towards ensuring both patient safety and also improving care for patients with chronic disease in Canada.
Conclusion
This research aimed to investigate the state of therapeutic CHO restriction among RDs practising in Canada. The study uncovered a variety of experiences within the dietetics community, ranging from strongly favourable based on science and experience to strongly unfavourable based on prior beliefs or patient appropriateness. Themes of interpersonal context, personal experience and knowledge, regulatory environment and patient-centred care each informed both if and how RDs prescribe CHO-restricted diets. Results showed a need in the RD community for accessible, trustworthy and evidence-based educational materials on the benefits, drawbacks and appropriateness of CHO-restricted diets for relevant populations. Additionally, dietitians reported a desire for greater discussion on this topic, without fear of reprimand or judgement. Finally, collaboration and shared understanding within a multidisciplinary care team appeared to be necessary for the safe implementation of CHO-restricted diets and for the benefit of patients in receiving consistent professional advice for effective, high-quality nutrition care for diabetes and other metabolic conditions.
Data availability statement
All relevant data are provided in the manuscript and appendices.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from the University of British Columbia Behavioural Research Ethics Board (#H19-03454-A005). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Acknowledgments
The authors would like to thank all the study participants who gave up their time to participate in the survey. They would also like to thank the Institute of Personalised Therapeutic Nutrition for assisting with the needs assessment survey.
References
Footnotes
Twitter @AnnalijnConklin
Contributors AC and EW initiated the project; EW designed the survey as part of a needs assessment. AC and EW were responsible for data collection and supervised AV in conducting the data cleaning and statistical analysis as part of a Directed Studies course. KY was second coder. All authors were involved in data analysis, interpretation and manuscript writing. AC is senior author and is the guarantor of this study
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests EW declares they are CEO of Eat Different, Co., which provides nutrition counselling services in Ontario, Canada.
Provenance and peer review Not commissioned; externally peer reviewed by Dr Paul McArdle, Birmingham, UK.